Explain where a needle is inserted into intercoastal space to drain a pleural effusion nd the anatomical basis. Name structures in order from skin to pleural that must be piereced
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive, authoritative information from multiple textbooks. Here is the full answer:
Thoracocentesis (Pleural Aspiration): Needle Insertion Site and Anatomy
Where the Needle Goes
The needle is inserted into a posterior or posterolateral intercostal space, typically in the midscapular or posterior axillary line, 1-2 intercostal spaces below the highest level of the effusion (confirmed by ultrasound). The usual target spaces are the 7th-9th intercostal spaces posteriorly, or the 4th-5th intercostal spaces in the midaxillary/anterior axillary line for chest drain insertion.
Critical rule: the needle must always pass over the superior (upper) border of the lower rib - never near the inferior border of the upper rib. This is the single most important anatomical point of the procedure.
The Anatomical Basis: Why the Superior Rib Border?
Each rib carries a neurovascular bundle - the intercostal vein, artery, and nerve - running in a groove on the inferior (subcostal) surface of the rib. The arrangement from superior to inferior within this groove is:
Vein - Artery - Nerve (mnemonic: VAN)
The nerve lies lowest and is most vulnerable. This bundle sits in the plane between the innermost intercostal and internal intercostal muscle layers, sheltered within the costal groove of the rib above. By inserting the needle at the superior border of the lower rib (i.e., the lowest point in the intercostal space), you stay well away from this bundle and avoid causing haemothorax, arterial puncture, or intercostal neuralgia.
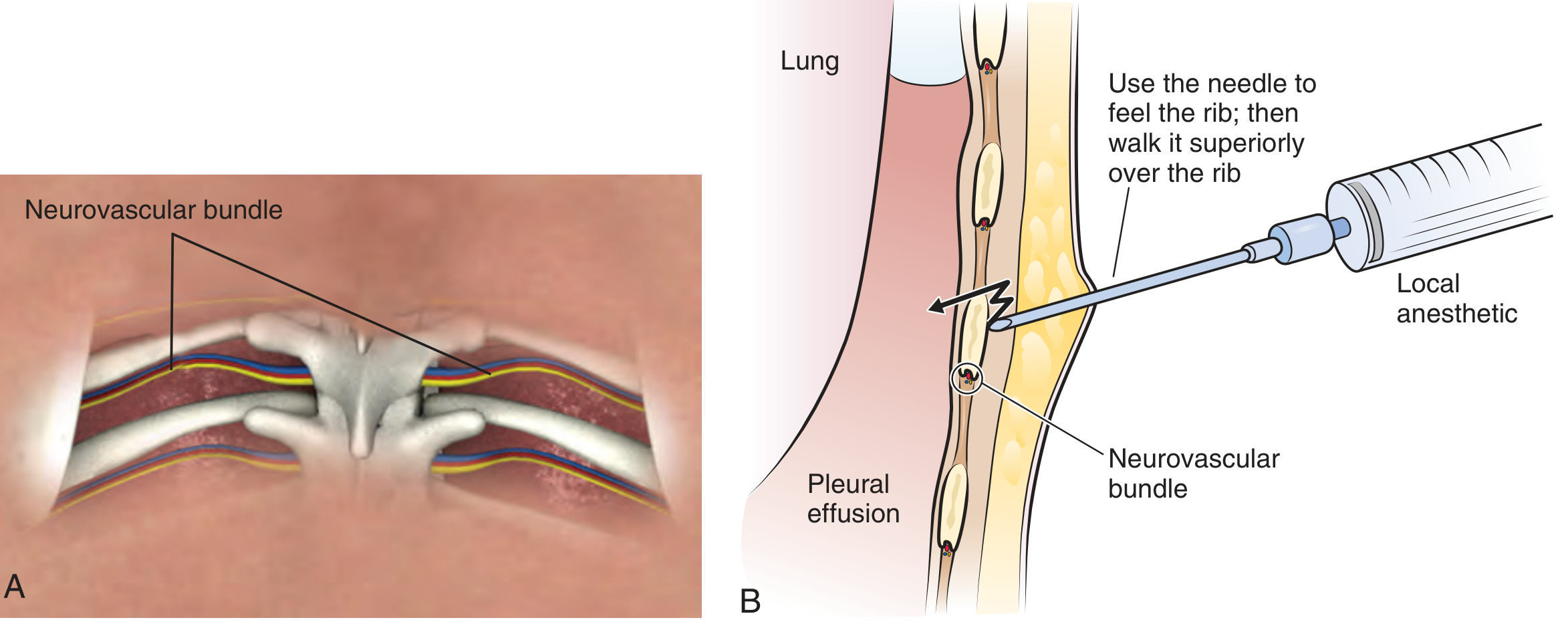
Figure from Roberts and Hedges' Clinical Procedures in Emergency Medicine - showing the neurovascular bundle at the inferior rib margin (A), and the correct technique of walking the needle superiorly over the rib surface to avoid the bundle (B).
Layers Pierced in Order: Skin to Pleural Space
| # | Layer | Notes |
|---|---|---|
| 1 | Skin | Anaesthetised first with a 25-gauge needle and lidocaine |
| 2 | Subcutaneous fat / superficial fascia | Variable thickness |
| 3 | Deep fascia | Thin investing layer over the chest wall muscles |
| 4 | Serratus anterior (lateral approach) or Trapezius / Latissimus dorsi (posterior approach) | These superficial back/chest wall muscles overlie the intercostal space at lateral or posterior sites |
| 5 | External intercostal muscle | Fibres run inferolaterally (like hands in pockets) |
| 6 | Internal intercostal muscle | Fibres run superomedially, at 90° to external |
| 7 | Innermost intercostal muscle (intercostalis intimus) | Deepest of the three intercostal muscle layers; the neurovascular bundle runs between this layer and the internal intercostal above it |
| 8 | Endothoracic fascia | A thin but distinct layer lining the thoracic cage internally; costal pleura is adherent to it |
| 9 | Parietal pleura | Extremely sensitive - anaesthetised separately; once punctured, a distinct "pop" may be felt |
| 10 | Pleural space | Fluid aspirated here to confirm correct placement |
The visceral pleura (covering the lung) is not pierced - the needle stops in the pleural space, which widens as effusion accumulates.
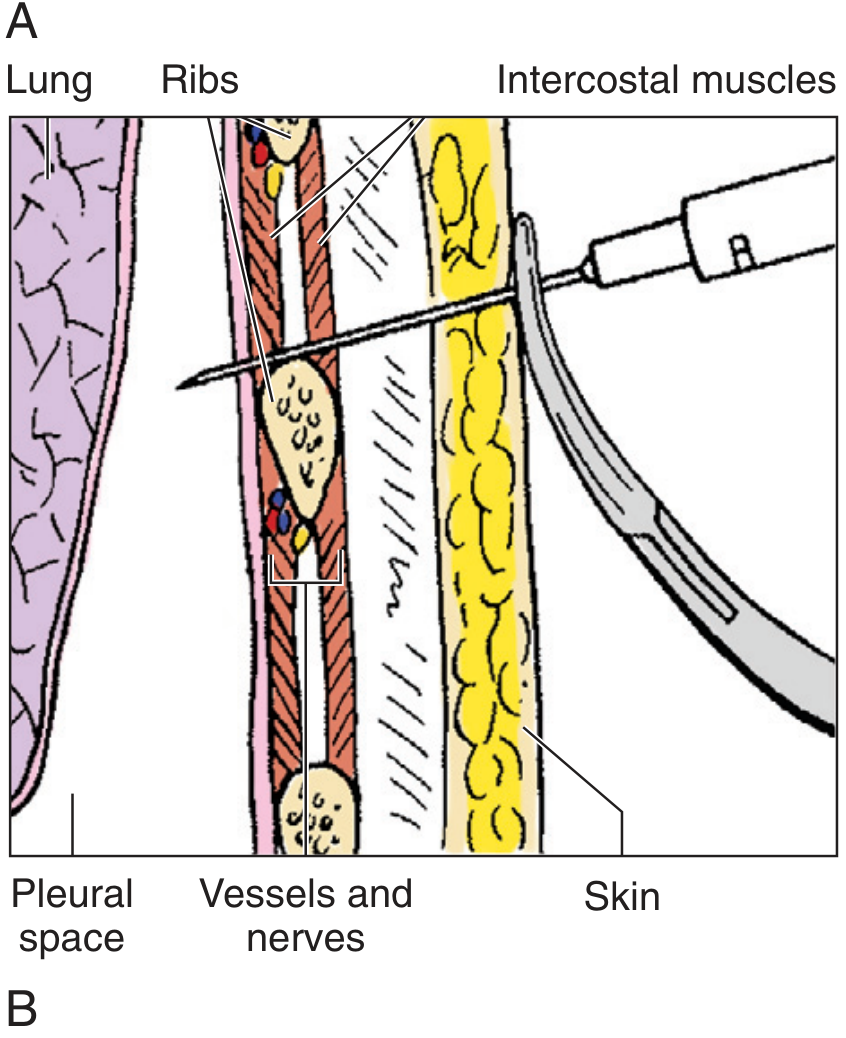
From Pfenninger and Fowler's Procedures for Primary Care - cross-sectional diagram of needle path through all layers.
Key Anatomical Boundaries and Safety Points
- Do not go below the 9th rib - risk of traversing the pleural recess and entering the liver (right) or spleen (left).
- Do not go medial to the midscapular line posteriorly - the intercostal artery runs more tortuous and centrally close to the vertebral column before entering the costal groove, increasing arterial injury risk.
- Do not go within 3-5 cm of the sternal border anteriorly - risk of puncturing the internal mammary (thoracic) artery.
- The parietal pleura must be separately anaesthetised - it is exquisitely pain-sensitive (supplied by intercostal nerves); the visceral pleura has no somatic innervation.
- At the midaxillary line, the serratus anterior muscle must also be traversed before reaching the intercostal muscles.
Summary
The procedure succeeds because gravity pools the effusion at the most dependent posterior/lateral aspect of the pleural space, and by entering at the superior border of a rib between the 7th-9th intercostal spaces, the clinician passes through 9 distinct tissue planes while completely avoiding the intercostal neurovascular bundle tucked safely into the subcostal groove above.
Sources: - Gray's Anatomy for Students (4th ed.), p. 197, 282-283 | Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 252-255 | Fischer's Mastery of Surgery (8th ed.), p. 2150 | Pfenninger and Fowler's Procedures for Primary Care, p. 683
This is a shared conversation. Sign in to Orris to start your own chat.