Ulcerative Colitis vs. Crohn’s Disease: List the primary differences between these two inflammatory conditions with unani treatment
Reading File
Finding Sources
Finding Sources
Searching the Web
Unani treatment ulcerative colitis Crohn's disease IBD herbal remedies
Reading File
Finding Sources
Searching the Web
Unani medicine IBD inflammatory bowel disease Habb-e-Papita Itrifal Zafrani treatment
Reading File
Reading Web Page
https://www.ejbps.com/ejbps/abstract_id/7489
Loading Image
Finding Sources
Finding Sources
I now have comprehensive data from the medical library and Unani sources. Let me compile the full answer.
Ulcerative Colitis vs. Crohn's Disease: Key Differences + Unani Treatment
Part 1: Primary Differences - UC vs. Crohn's Disease
Location & Distribution
| Feature | Crohn's Disease (CD) | Ulcerative Colitis (UC) |
|---|---|---|
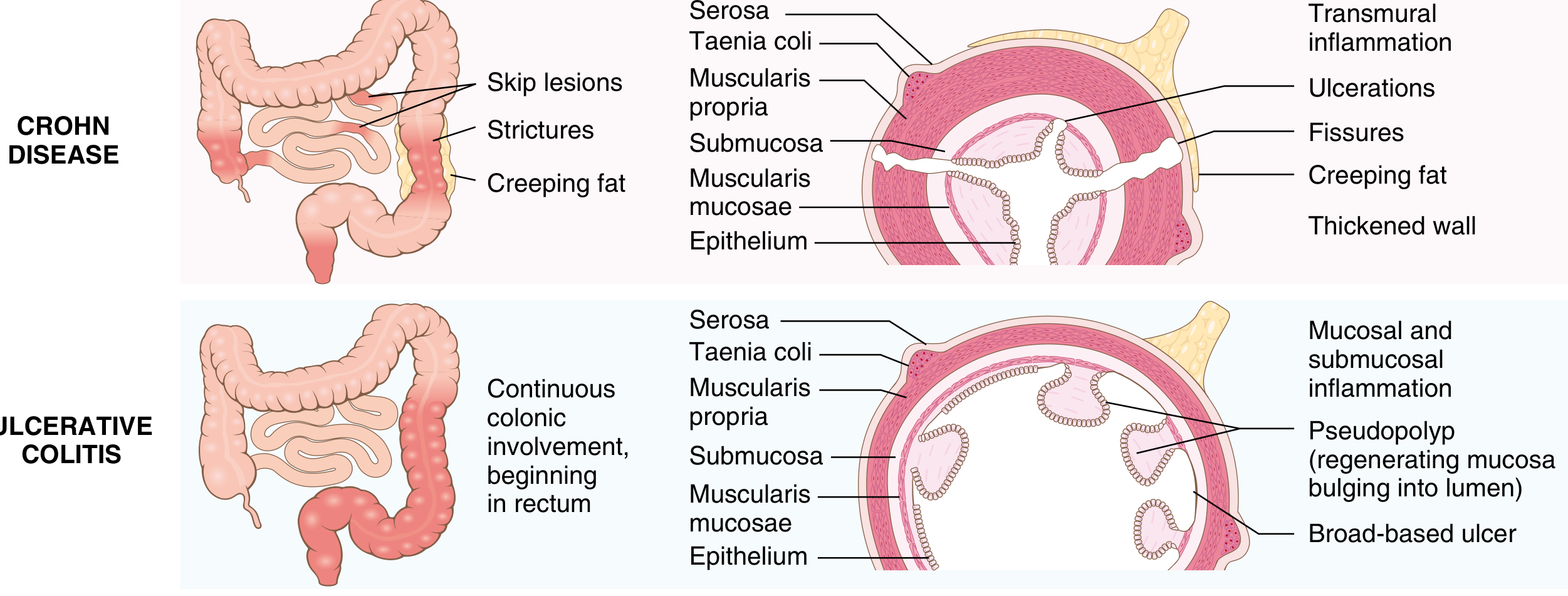
| Sites involved | Anywhere from esophagus to anus | Colon and rectum ONLY |
| Most common site | Terminal ileum + proximal colon (~70% ileum involvement) | Begins in rectum, spreads proximally |
| Distribution pattern | Skip lesions (normal bowel between inflamed segments) | Continuous, diffuse inflammation |
| Rectal involvement | Variable | Almost always involved |
Depth of Inflammation
| Feature | Crohn's Disease | Ulcerative Colitis |
|---|---|---|
| Depth | Transmural (full bowel wall thickness) | Limited to mucosa and submucosa |
| Wall appearance | Thickened ("hose pipe" feel) | Normal thickness |
| Ulcer type | Deep, knife-like ("rose thorn" ulcers) | Superficial, broad-based |
| Serositis | Marked | Mild to none |
Pathological Features
| Feature | Crohn's Disease | Ulcerative Colitis |
|---|---|---|
| Granulomas | Yes (~35% of cases) | No |
| Fistulae/sinuses | Yes (20-40% develop fistulae) | No |
| Strictures | Yes (transmural scarring) | Rare |
| Fibrosis | Marked | Mild to none |
| Pseudopolyps | Moderate | Marked |
| Lymphoid reaction | Marked | Moderate |
| "Creeping fat" | Yes (mesenteric fat wrapping) | No |
- Robbins Pathologic Basis of Disease, Table 17.8, p. 744
- Goldman-Cecil Medicine, Table 127-1, p. 1481
Clinical & Symptomatic Differences
| Feature | Crohn's Disease | Ulcerative Colitis |
|---|---|---|
| Peak age of onset | 15-30 yrs (2nd peak in 7th decade) | 20-40 yrs (smaller 2nd peak after 7th decade) |
| Sex distribution | Slight female predominance (F:M = 1.2:1) | Equal (F:M = 1:1) |
| Abdominal pain | Right lower quadrant (ileal) | Lower left quadrant/diffuse |
| Rectal bleeding | Less common | Common (hallmark) |
| Bloody diarrhea | Less prominent | Very prominent |
| Perianal disease | Yes - fissures, fistulae, skin tags (~30%) | No |
| Malabsorption | Yes - fat and vitamin B12 (ileal involvement) | No |
| Obstruction | Yes (due to strictures) | Rare |
| Toxic megacolon | No | Yes |
| Recurrence after surgery | Common | None (curative colectomy) |
| Malignant potential | With colonic involvement | Yes (high with pancolitis) |
| Nausea/vomiting | Yes | Less common |
Extra-intestinal Manifestations
Both conditions share extra-intestinal features, but perianal disease, uveitis, and malabsorption-related complications (anemia, vitamin D/B12 deficiency, osteoporosis) are more prominent in Crohn's disease. Toxic megacolon and primary sclerosing cholangitis are more associated with UC.
Part 2: Unani (Tibb-e-Unani) Treatment
Unani Conceptual Framework for IBD
In Unani medicine, IBD is understood under the concepts of:
- Zusantariya (dysentery-like condition) - passage of stool mixed with blood, mucus, or both
- Sahej - erosion of the intestinal mucosa (ulceration)
- Aanton ki Sozish - intestinal inflammation
The pathophysiology is explained through:
- Su'-Mizaj Har Ya Barid of Am'a - deranged intestinal temperament (hot or cold)
- Ghalba-e-Dam or Safra - dominance of blood or bile humour
- Safra and Balgham-e-shore - hot bile and salty phlegm damaging the intestinal mucosa, scraping off the mucous lining (reflecting mucosal breakdown)
- Weak Quwwat-e-Hazima and Maskah - weakened digestive and retentive faculties
Core Principles of Unani Management
- Islah-e-Mizaj - Correction of deranged temperament
- Tanqiyah-e-Mawad-e-Fasida - Elimination of morbid/pathological matter
- Taqwiyat-e-Jigar - Strengthening of the liver (source of humoral balance)
- Taqwiyat-e-Am'a - Strengthening the intestines
- Iltiyam-e-Quruh - Healing of ulcers
- Daf'-e-Iltihab - Control of inflammation
Unani Pharmacotherapy (Ilaj bil Dawa)
Medicines are selected based on the patient's Mizaj (individual temperament) and disease severity.
Single Drug Preparations (Mufradat)
| Drug | Botanical Name | Action |
|---|---|---|
| Mako | Solanum nigrum | Anti-inflammatory, hepatoprotective |
| Kasni | Cichorium intybus | Liver tonic, anti-inflammatory |
| Kundur | Boswellia serrata | Anti-inflammatory (5-LOX inhibitor) |
| Post-e-Anar | Pomegranate rind (Punica granatum) | Astringent, anti-inflammatory, antidiarrheal |
| Tabasheer | Bamboo manna (Bambusa arundinacea) | Mucosal cooling, demulcent |
| Gul-e-Surkh | Rosa damascena | Anti-inflammatory, mucosal healer |
| Mochras | Bombax ceiba resin | Astringent, stops bleeding |
| Maghz-e-Tukhm-e-Kharpaza | Melon seed kernel | Demulcent, soothing |
Note: Boswellia serrata (Kundur) is particularly well-researched. A randomized trial in Yamada's Textbook of Gastroenterology notes that Indian patients with chronic colitis given B. serrata gum resin had a higher response/remission rate than those treated with sulfasalazine. It is a specific inhibitor of the enzyme 5-lipoxygenase.
Compound Formulations (Murakkabat)
| Formulation | Predominant Use |
|---|---|
| Habb-e-Rasaut | Anti-inflammatory, anti-infective for intestines |
| Habb-e-Raal | Intestinal healing and astringency |
| Jawarish Mastagi | Gut strengthening, anti-inflammatory (mastic gum base) |
| Jawarish Anarain | Strengthens colon, checks loose motions |
| Jawarish Aamla | Liver and digestive tonic |
| Majoon Dabidul Ward | Rose-based, anti-inflammatory for intestinal ulcers |
| Majoon Sang Dana Murgh | Intestinal astringent and tonic |
| Qurs-e-Gulnar | Pomegranate flower-based; astringent, mucosal healer |
| Sufoof-e-Sat-e-Gilo | Tinospora cordifolia extract; immunomodulatory |
| Sharbat Deenar | Cooling, anti-inflammatory syrup |
| Sharbat Belgiri | Bael-based; antidiarrheal, mucosal strengthening |
| Arq-e-Kasni / Arq-e-Mako | Distillates for liver and intestinal inflammation |
Dietotherapy (Ilaj bil Ghiza)
Recommended during flares:
- Soft rice and barley water (Maa-ul-Shaeer)
- Pomegranate juice (diluted) - astringent, anti-inflammatory
- Apple stew
- Curd/yogurt if tolerated
- Isabgol (psyllium husk) in moderation
Avoid:
- Spicy, fried, and heavy foods
- Excessive sour/acidic foods
- Alcohol
- Raw vegetables during flares
- Heavy meats
Regimental Therapy (Ilaj bil Tadbeer)
- Rest and stress reduction (mental temperament affects gut in Unani theory)
- Huqna (enema) with herbal decoctions for local colonic healing (applicable for UC due to colonic location)
- Appropriate physical rest during acute exacerbations
Key Distinction in Unani Treatment Context
| Feature | Crohn's (Zusantariya of upper intestine/Ileum) | UC (Zusantariya of lower intestine/Colon) |
|---|---|---|
| Predominant focus | Ileal healing, B12/fat malabsorption support, fistula management | Colonic mucosal healing, rectal astringents |
| Route of drug delivery | Oral emphasis (to reach small bowel) | Oral + Huqna (rectal enema) possible |
| Complication management | Stricture prevention, abscess | Toxic megacolon vigilance |
Important Note
Unani medicine does not have a direct classical term equivalent to "Crohn's disease" vs. "Ulcerative Colitis" as distinct entities. Classical texts classify them together under intestinal lesion conditions (Zusantariya/Sahej/Ishaal), distinguished by whether the upper or lower intestine is affected. Modern Unani practitioners increasingly use contemporary diagnosis to guide the classical formulation choice.
Always consult a qualified Unani physician (Hakim) for prescription of specific formulations and dosages, as medicine selection depends on individual Mizaj assessment.
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Table 17.8 & Fig. 17.35
- Goldman-Cecil Medicine, Table 127-1
- Yamada's Textbook of Gastroenterology (Boswellia serrata data)
- Sultana et al., "Clinical Efficacy of Unani Medicine in IBD" (EJBPS)
- Tibb-e-Unani clinical framework (Unani Medicine practitioner sources)
This is a shared conversation. Sign in to Orris to start your own chat.