Retrocalcenious bursitis, tell about everything, feom anatomy to management
retrocalcaneal bursitis treatment
Retrocalcaneal Bursitis - A Complete Guide
1. Anatomy
The Retrocalcaneal Bursa
- Fibrocartilage on the anterior tendon surface
- Fibrocartilage on the opposing calcaneal surface
- The retrocalcaneal bursa (the space between these cartilaginous layers)
- A synovial-lined fat wedge (Kager's fat pad) that slides in and out of the bursa during ankle dorsiflexion/plantarflexion
- Underlying trabecular bone
- Goldman-Cecil Medicine, p. 2780
Bursae Around the Heel (Distinguishing Anatomy)
| Bursa | Location | Also Called |
|---|---|---|
| Retrocalcaneal bursa | Between Achilles tendon and posterosuperior calcaneal tuberosity (deep) | Subachilles bursa |
| Retroachilles (pre-tendinous) bursa | Between Achilles tendon and overlying skin (superficial) | Subcutaneous calcaneal bursa |
- Roberts and Hedges' Clinical Procedures in Emergency, p. 1210
2. Pathophysiology
- Repeated microtrauma and friction
- Inflammation of the bursa (retrocalcaneal bursitis)
- With prolonged inflammation: degenerative changes and osteophyte formation within the tendon
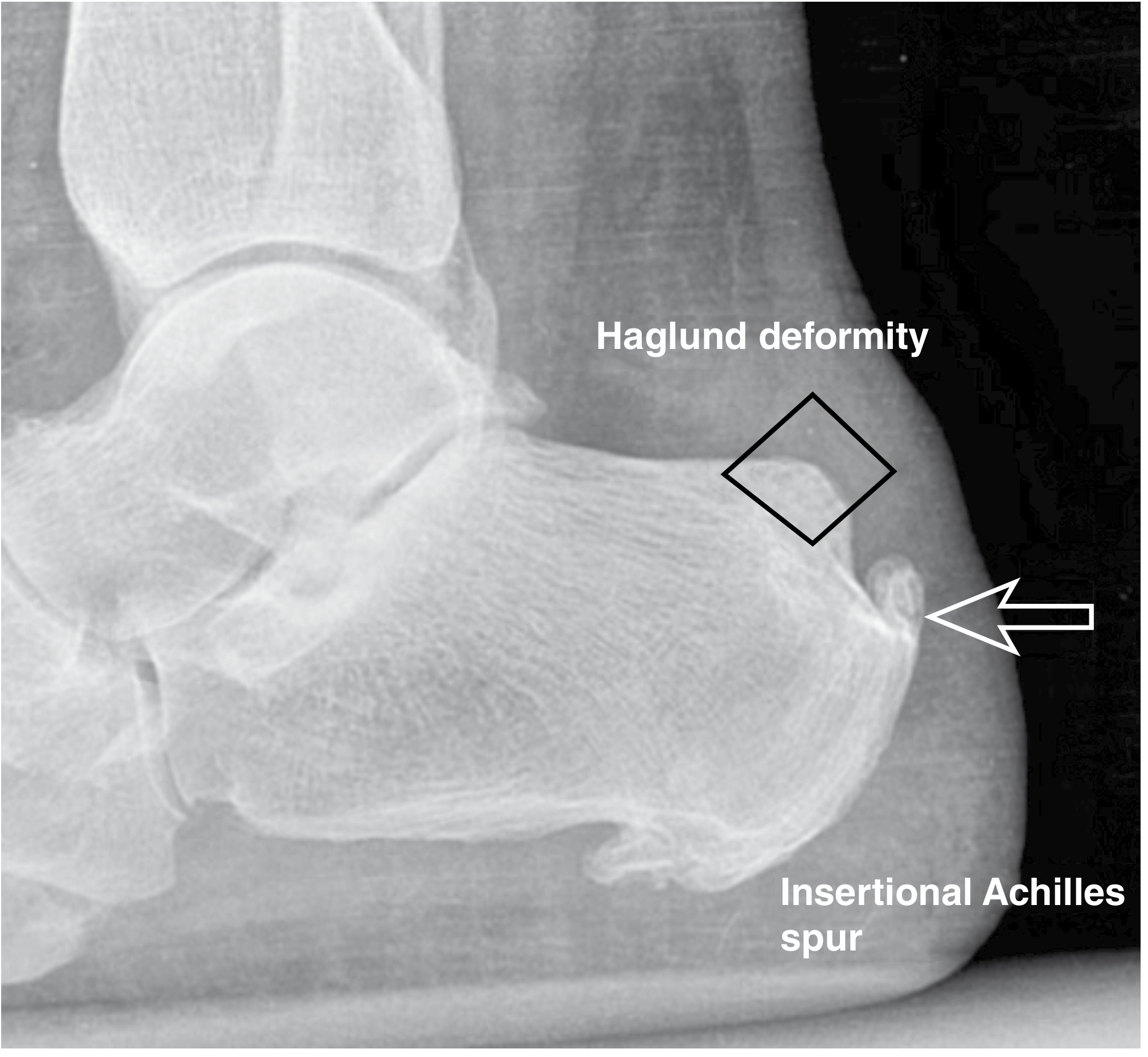
A true Haglund deformity is a large exostosis off the posterosuperior aspect of the calcaneal tuberosity, located anterior to the Achilles tendon. The term is often incorrectly used to describe any posterior heel swelling.
- Campbell's Operative Orthopaedics 15th Ed, p. 4878
Systemic Associations
- Spondyloarthropathies (ankylosing spondylitis, psoriatic arthritis) - the entheseal organ is a hallmark site
- Rheumatoid arthritis
- Gout (urate crystal deposition in bursa)
- Calcium pyrophosphate dihydrate (CPPD) disease
- Ochronosis (homogentisic acid deposition)
3. Clinical Presentation
Symptoms
- Deep posterior heel pain - insidious onset, not typically from acute injury
- Pain worsened by ankle dorsiflexion (tightens Achilles against calcaneal exostosis)
- Pain when first arising in the morning (distinct from plantar fasciitis which is purely plantar)
- Difficulty wearing closed-back shoes
- Progressive fullness/swelling medial and lateral to the Achilles tendon
Pain only when wearing shoes may indicate pretendinous bursitis; pain on first arising in the morning is more consistent with retrocalcaneal bursitis.
- Campbell's Operative Orthopaedics, p. 4878
Signs
- Fullness and tenderness on direct palpation medial and lateral to the Achilles tendon (just anterior to it, over the calcaneal tuberosity)
- Fluid fluctuation test: clinician places thumb and index finger at either side of the insertional tendon; the other index finger presses repeatedly over the tendon, and fluctuation is perceived by the exploring fingers
- Increased pain with passive ankle dorsiflexion
- Gastrocsoleus contracture on examination (especially with knee in extension)
- Visible bony bump at the posterosuperior heel (Haglund prominence)
- Goldman-Cecil Medicine, p. 2780
4. Imaging
Plain Radiograph (Lateral Foot X-ray) - First-Line
- Standing lateral view is the standard
- Shows the Haglund deformity (prominent posterosuperior calcaneal tuberosity)
- Look for insertional Achilles spur, intratendinous calcification, and increased calcaneal pitch angle
- Note: the size of the Haglund deformity has not been statistically different between symptomatic patients and controls - clinical correlation is required
Ultrasound
- Demonstrates bursal fluid (anechoic/hypoechoic collection anterior to Achilles tendon)
- Fusiform thickening and mixed echogenicity of the tendon if tendinopathy is concurrent
- Doppler shows hyperaemia within the tendon and Kager's fat pad in active inflammation
- Dynamic imaging is useful
- Cost-effective and widely available
MRI
- Rarely necessary for diagnosis of isolated retrocalcaneal bursitis, but useful when:
- Extent of Achilles tendon degeneration needs quantification (for surgical planning)
- Rule out partial tear
- Confirm less than 50% intrasubstance degeneration (if Zadek osteotomy is being considered)
- Shows the Haglund syndrome triad: insertional Achilles tendinopathy + retrocalcaneal bursitis + posterosuperior calcaneal exostosis
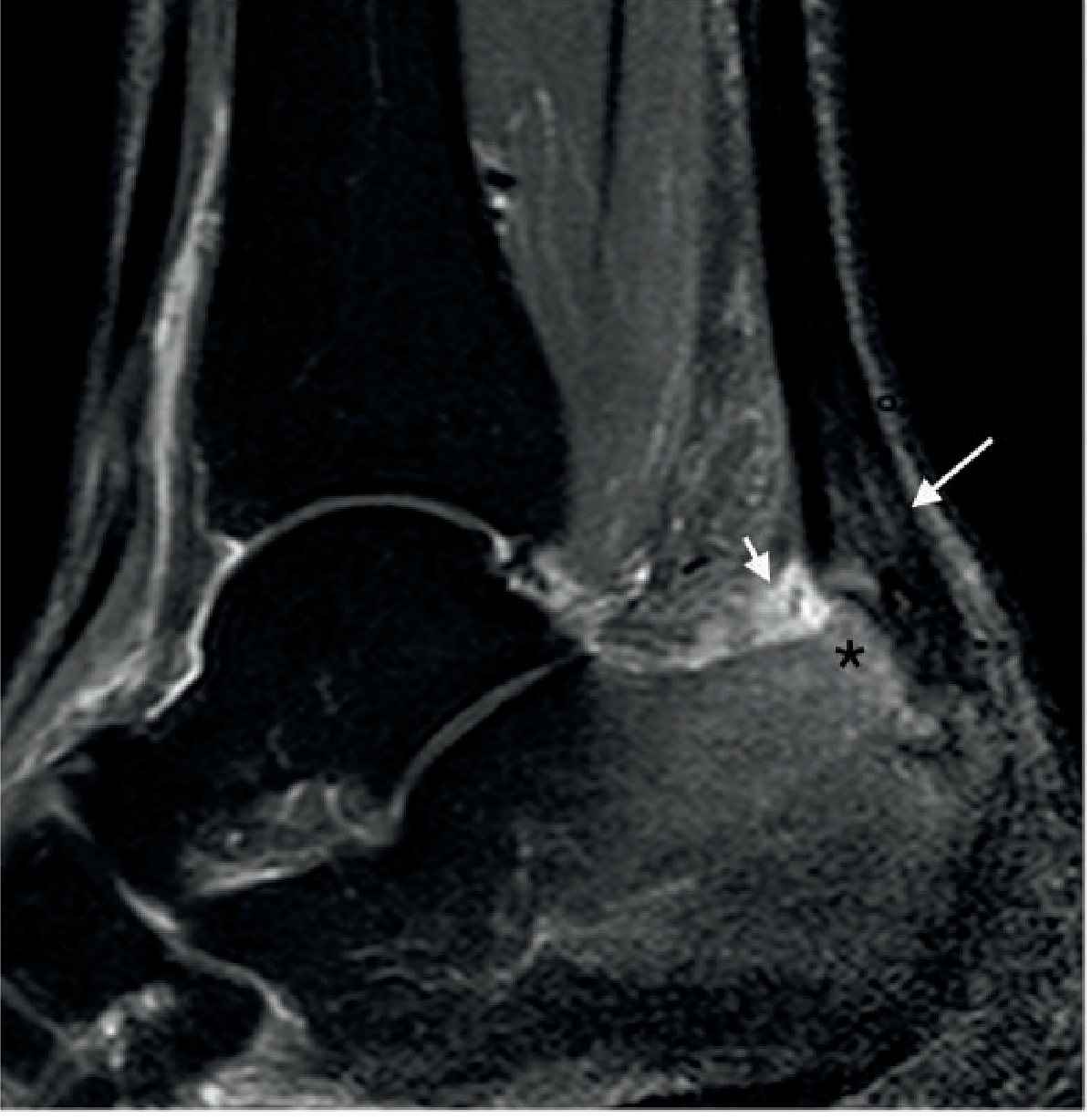
- Grainger & Allison's Diagnostic Radiology, p. 1000
- Miller's Review of Orthopaedics 9th Ed, p. 594
5. Differential Diagnosis
| Condition | Key Distinguishing Feature |
|---|---|
| Insertional Achilles tendinopathy | Tenderness directly at/over the tendon insertion, midline |
| Pretendinous (subcutaneous) bursitis | Pain only with shoe-wear, tenderness superficial to tendon |
| Plantar fasciitis | Plantar heel pain, maximum at medial calcaneal tubercle |
| Sever's disease (calcaneal apophysitis) | Children 7-10 years, posterior heel tenderness, activity-related |
| Gout / pseudogout | Crystal-proven, acute attacks, hyperuricemia |
| Spondyloarthritis | Bilateral, enthesitis elsewhere, systemic features |
| Achilles tendon rupture | Acute onset, Thompson test positive, palpable gap |
6. Management
Non-operative (First-Line, Try for at Least 3-6 Months)
- Activity restriction and shoe wear modification (open-back shoes to eliminate pressure on the posterior heel counter)
- Heel lift orthotics - reduce tension on the Achilles tendon and decrease impingement against calcaneus
- External heel padding / silicone pads
- Avoid high-heeled or stiff-backed footwear
- NSAIDs (oral or topical) - reduce inflammation
- Short course useful in acute flares
- Stretching of the gastrocsoleus complex - especially with knee in extension (Silfverskiöld test guides this)
- Eccentric training with heavy, slow resistance exercises
- Astym therapy
- Dry needling
- Dorsiflexion night splints to maintain a stretch overnight
- 3D walking boot for acute severe inflammation
- Short-leg walking cast for recalcitrant cases
⚠️ Corticosteroid injection should be avoided owing to the inherent risk of Achilles tendon rupture. Repeated steroid injection is strongly associated with Achilles tendon rupture.
- Miller's Review of Orthopaedics 9th Ed; Roberts and Hedges' Clinical Procedures in Emergency
- If corticosteroid is used (e.g., by an expert in non-tendinous disease), strict needle placement into the bursa (not tendon) is required, and repeat injections are to be avoided
- Platelet-rich plasma (PRP): The biologic rationale is sound, but clinical studies supporting efficacy in Achilles tendinopathy remain inconclusive - recently published studies have failed to demonstrate short- or long-term improvement over placebo
- Prolotherapy, autologous blood injection, sclerosing agents: evidence evolving
- Low-energy ESWT is an established option for chronic retrocalcaneal bursitis and insertional Achilles tendinopathy failing conservative treatment
- Campbell's Operative Orthopaedics 15th Ed, Box 88.1 (p. 4877)
- Goldman-Cecil Medicine, p. 2780
Operative Treatment (After Failure of Non-operative Management)
- Most common procedure
- Removal of the inflamed bursa + resection of the Haglund exostosis
- Can be performed via open or endoscopic (arthroscopic) approach
- Isolated endoscopic calcaneal exostectomy is suitable for recalcitrant retrocalcaneal bursitis without significant tendinosis
- Return to sport: approximately 67% at 8 months after exostectomy
- For later-stage disease when insertional tendinosis accompanies bursitis
- Tendon debridement with calcaneal exostectomy
- If >50% of the tendon footprint is debrided, augmentation with flexor hallucis longus (FHL) tendon transfer is typically required
- Large incisions and prolonged recovery with open techniques; 78% return to sport at 10 months after reconstruction
- Decompresses the Achilles insertion by reducing calcaneal pitch angle
- Best for patients with less than 50% intrasubstance tendinosis on MRI
- Minimally invasive / percutaneous approaches reduce wound complications and sural nerve injury risk
- A 2023 systematic review and meta-analysis (PMID: 37088671) confirms good clinical outcomes with this technique
- Addresses the gastrocnemius contracture component
- Reported success in both insertional and non-insertional tendinopathy
- Associated with continued plantarflexion weakness at 18 months post-operatively
- Campbell's Operative Orthopaedics 15th Ed, pp. 4879-4880
- Miller's Review of Orthopaedics 9th Ed, p. 594
7. Prognosis
- The majority of patients respond well to conservative management
- Surgical outcomes are generally favorable; most patients return to prior activity levels
- Risk of wound complications and sural nerve injury exist with open techniques - minimally invasive approaches reduce this risk
- Patients with systemic inflammatory disease (spondyloarthritis, RA, gout) require concurrent systemic management for best results
Summary Table
| Domain | Key Points |
|---|---|
| Anatomy | Synovial bursa between Achilles tendon and posterosuperior calcaneus; part of Achilles entheseal organ |
| Pathophysiology | Mechanical impingement (Haglund deformity) or systemic inflammation (SpA, RA, gout) |
| Symptoms | Deep posterior heel pain, worse with dorsiflexion, morning stiffness, difficulty with closed-back shoes |
| Examination | Mediolateral tenderness anterior to Achilles, fluctuation test |
| Imaging | X-ray (Haglund deformity), US (bursal fluid, Doppler), MRI rarely needed |
| Non-operative | NSAIDs, heel lifts, shoe modification, stretching, ESWT; avoid corticosteroid injection near tendon |
| Operative | Bursal debridement + exostectomy (open or endoscopic); Zadek osteotomy; tendon debridement ± FHL transfer |
- Campbell's Operative Orthopaedics 15th Ed 2026, Chapter 88
- Miller's Review of Orthopaedics 9th Ed
- Goldman-Cecil Medicine (International Edition)
- Grainger & Allison's Diagnostic Radiology
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
- Zadek osteotomy meta-analysis: Poutoglidou et al., Foot Ankle Surg 2023 [PMID: 37088671]
- General heel pain review: Morancie et al., Am Fam Physician 2025 [PMID: 41533410]
Continue
retrocalcaneal bursitis endoscopic calcaneoplasty outcomes
retrocalcaneal bursitis shock wave therapy platelet rich plasma
PMID: 33216187
PMID: 36060327
8. Radiological Measurement Tools
Fowler-Philip Angle
- The angle between the line connecting the posterior tuberosity to the posterior calcaneal process, and the line connecting the posterior tuberosity to the plantar surface
- Normal: <69° - angles >75° are associated with symptomatic Haglund deformity
Parallel Pitch Lines (PPL) Method
- A line is drawn parallel to the plantar calcaneal surface, passing through the posterior lip of the subtalar facet
- A second parallel line is drawn through the medial talar process (inferior surface)
- If the posterosuperior calcaneal process protrudes above the upper parallel pitch line, Haglund deformity is present
Calcaneal Pitch Angle
- Measured between the plantar surface of the calcaneus and the floor
- Increased calcaneal pitch angle has been associated with insertional Achilles tendinopathy (whereas Haglund size alone has not)
Important caveat
The size of the Haglund deformity in symptomatic patients has not been statistically different from control groups in studies. An insertional Achilles osteophyte, insertional calcification, or an increased calcaneal pitch angle has a stronger association with symptoms.
- Campbell's Operative Orthopaedics 15th Ed, p. 4878
9. Endoscopic (Tendoscopic) Surgery - In Depth
Surgical Technique (Endoscopic Calcaneoplasty)
- Two portals are used: a medial and a lateral portal, both placed just anterior to the Achilles tendon at the level of the superior calcaneal tuberosity
- Arthroscope inserted through one portal; shaver/burr through the other
- Sequence: debridement of inflamed retrocalcaneal bursa → identification of Haglund exostosis → bony resection with motorised burr
- The Achilles tendon is protected throughout
- The procedure can be performed under regional or local anaesthesia
Outcomes Data
| Outcome | Open | Endoscopic | p-value |
|---|---|---|---|
| AOFAS score | 87.1 ± 5.9 | 90.7 ± 4.2 | <0.001 |
| Complication rate | 15.5% | 4.1% | <0.001 |
| Failure rate | 6.0% | 1.2% | <0.001 |
| Return to daily activities | 17.2 weeks | 6.3 weeks | <0.001 |
| Return to sport | 20.7 weeks | 11.9 weeks | <0.001 |
Advantages of Endoscopic Over Open Surgery
- Significantly lower complication rate (4.1% vs. 15.5%)
- Faster return to daily activities and sport (nearly half the recovery time)
- Lower failure rate (1.2% vs. 6.0%)
- Avoids large posterior incision and its wound complications
- Reduced risk of sural nerve injury
- Better cosmesis
Complications of Open Surgery (worth knowing)
- Wound dehiscence and infection
- Sural nerve injury (most common nerve at risk)
- Prolonged recovery
- Skin necrosis (especially with posterior midline incisions)
- Achilles tendon weakening if excessive tendon debridement required
10. Zadek Osteotomy - More Detail
Mechanism
- A dorsal wedge of bone is removed from the calcaneus
- Closing the wedge rotates the posterior calcaneal tuberosity downward and forward
- This decompresses the retrocalcaneal space and reduces Achilles tendon insertion tension
Patient Selection
- Best for patients with <50% intrasubstance Achilles tendinosis on MRI
- High calcaneal pitch angle (the osteotomy directly corrects this deformity)
- Retrocalcaneal bursitis ± Haglund deformity without severe tendinosis
Outcomes
- Continued improvement in pain and function at 2 years (28-patient series, Campbell's)
- Minimally invasive / percutaneous approaches now described - fewer wound complications and lower sural nerve injury risk compared to open Zadek
- 2023 meta-analysis (PMID 37088671) confirms good outcomes; controversy remains over optimal patient selection
11. FHL Tendon Transfer (When Indicated)
Rationale
- FHL (flexor hallucis longus) is the workhorse augmentation tendon
- It runs in close anatomical proximity to the calcaneus (nearby musculotendinous unit)
- It provides strong, well-vascularized tissue
- The great toe loses some active plantarflexion strength, but this is generally well tolerated
Approach options
- Open FHL transfer: reliable, established technique; significant incision required
- All-endoscopic FHL transfer: technically demanding with steep learning curve; outcomes and complication rates comparable to percutaneous Achilles repair; minimises wound complications
12. Endoscopic Gastrocnemius Recession
- Open vs. endoscopic approaches both effective
- Endoscopic: fewer wound complications (1 dehiscence vs. 10 complications in open group in one comparative series - Harris et al.)
- Associated with persistent plantarflexion weakness at 18 months
- Tendoscopic gastrocnemius tendon recession (Phisitkul technique): prospective study of 320 patients showed improvement in ankle dorsiflexion, pain, and validated outcome scores at 1 year
13. Specific Populations
Athletes
- High demand for return to sport - endoscopic approach preferred
- Eccentric training programs (e.g., Alfredson protocol) should be trialled for at least 12 weeks before surgery is considered
- Haglund deformity ("pump bump") common in distance runners and those in stiff-backed footwear (the condition was classically described in women wearing high-heeled "pump" shoes)
Spondyloarthritis / Inflammatory Arthropathy
- Retrocalcaneal bursitis in spondyloarthritis requires systemic disease-modifying treatment (NSAIDs, biologics targeting TNF-α or IL-17) in addition to local measures
- Corticosteroid injection of the bursa may be used more liberally in inflammatory arthritis (less concern about tendon rupture when the primary pathology is synovitis rather than tendinosis)
- Bilateral presentation strongly suggests a systemic cause
Paediatrics (Sever's Disease vs. Retrocalcaneal Bursitis)
- True retrocalcaneal bursitis is rare in children
- Posterior heel pain in children aged 7-10 years is most commonly Sever's disease (calcaneal apophysitis) - traction injury at the apophysis
- Self-limited; treat with rest, ice, heel pads; radiographs not needed unless another diagnosis is suspected
Fluoroquinolone Use
- Quinolone antibiotics (e.g., ciprofloxacin, levofloxacin) predispose to Achilles tendinopathy and rupture - can occur during or up to weeks after therapy
- Immediate discontinuation required if recognised
- Retrocalcaneal bursitis emerging during fluoroquinolone therapy should prompt drug cessation
14. Physical Therapy Protocols (Detailed)
Phase 1 - Acute Phase (Weeks 1-4)
- Rest and activity modification (avoid aggravating dorsiflexion loading)
- Ice (15-20 min, 3-4x daily)
- NSAIDs / topical anti-inflammatories
- Heel lift in shoe (raises calcaneus, reduces dorsiflexion impingement)
- Night splint if morning pain significant
- Boot immobilisation for severe acute flares
Phase 2 - Subacute / Loading Phase (Weeks 4-12)
- Eccentric heel drops (the cornerstone of Achilles tendinopathy rehab):
- Patient stands on the edge of a step, rises on toes bilaterally, then lowers slowly on the affected leg only
- 3 sets × 15 reps, twice daily
- Initially with straight knee (targets gastrocnemius), then with bent knee (targets soleus)
- Heavy slow resistance (HSR) training: shown equivalent or superior to eccentric-only in clinical trials for tendinopathy
- Gastrocnemius and soleus stretching
- Astym soft tissue mobilisation
- Dry needling of the posterior calf chain
Phase 3 - Sport/Activity Return (Weeks 12+)
- Progressive plyometric loading
- Sport-specific drills
- Footwear optimisation (appropriate heel counter, cushioning)
- ESWT can be added for recalcitrant cases at any phase from 6 weeks onwards
15. Complete Management Algorithm
POSTERIOR HEEL PAIN
↓
Clinical Examination
├─ Mediolateral tenderness anterior to Achilles → Retrocalcaneal bursitis
├─ Tenderness over tendon at insertion → Insertional Achilles tendinopathy
└─ Superficial tenderness with shoes only → Pretendinous bursitis
↓
X-ray (standing lateral)
├─ Haglund deformity present? → Haglund syndrome likely
├─ Insertional spur / calcification? → Tendinopathy component
└─ Normal? → Consider systemic cause, US/MRI
↓
Systemic features? (bilateral, SpA, RA, gout, fluoroquinolone use)
YES → Address systemic disease concurrently
NO → Mechanical/overuse pathway
↓
NON-OPERATIVE (minimum 3-6 months)
• Heel lifts, open-back shoes, padding
• NSAIDs (short course)
• Eccentric / HSR exercise programme
• Night splint, ESWT for chronic cases
• Boot for acute severe inflammation
⚠ Avoid corticosteroid injection near Achilles tendon
↓
FAILED CONSERVATIVE?
↓
MRI to assess tendinosis extent (<50% vs >50% involvement)
↓
<50% tendinosis >50% tendinosis
↓ ↓
Endoscopic calcaneoplasty Debridement + exostectomy
± Zadek osteotomy + FHL transfer (augmentation)
(preferred - faster recovery, (open or endoscopic)
lower complications)
Quick Reference Summary
| Topic | Key Facts |
|---|---|
| Bursa location | Deep to Achilles, between tendon and posterosuperior calcaneal tuberosity |
| Haglund deformity | Enlarged posterosuperior calcaneal exostosis - the mechanical cause |
| Haglund syndrome triad | Insertional tendinopathy + retrocalcaneal bursitis + calcaneal exostosis |
| Key exam sign | Mediolateral squeeze test anterior to Achilles = fluid fluctuation |
| First imaging | Standing lateral X-ray |
| Avoid | Corticosteroid injection near Achilles (rupture risk) |
| ESWT | Effective for chronic cases (>6 weeks) |
| Surgery threshold | After 3-6 months failed conservative care |
| Preferred surgery | Endoscopic calcaneoplasty (AOFAS 90.7, 4.1% complications) |
| If >50% tendinosis | Debridement + FHL transfer |
| Zadek osteotomy | Best with <50% tendinosis, high calcaneal pitch |
| Fluoroquinolones | Stop immediately if Achilles tendinopathy develops |
| Systemic causes | SpA, RA, gout, CPPD, ochronosis |
- Endoscopic vs. open surgery: Alessio-Mazzola et al., KSSTA 2021 [PMID 33216187] - 1,260 ankles, Level IV systematic review
- Surgical treatment review: Yuen et al., Cureus 2022 [PMID 36060327]
- Zadek osteotomy meta-analysis: Poutoglidou et al., Foot Ankle Surg 2023 [PMID 37088671]
- Campbell's Operative Orthopaedics 15th Ed 2026, Chapters 55 (Tendoscopy) and 88 (Insertional Achilles)
- Miller's Review of Orthopaedics 9th Ed, Chapter 6
Now make PPT of whats all details you mentioned, including more images and diagrams for reference and add some local marathi language to exting data
node /home/daytona/skills/shared/scripts/fetch_images.js \ "https://cdn.orris.care/cdss_images/2552b51a06c8a672790c07de779e7740ecda895a9121397a5dbe9030ffd1be7b.png" \ "https://cdn.orris.care/cdss_images/9b682c75f07ccfac7ba9b8d23ff7c9904f583b6b7c2192404d29d8fc94b2e094.png" \ "https://cdn.orris.care/cdss_images/719c92d190cc775d327fad8c132f988df02c80348f8743f56d24d142ed9b3d16.png" \ "https://cdn.orris.care/cdss_images/c77cd37ed2dea1c94a909acb623717a5af67bc5cdfce3b60828ec6eef9b15dd8.png" \ 2>/dev/null | node -e "const d=require('fs').readFileSync('/dev/stdin','utf8'); const arr=JSON.parse(d); arr.forEach((x,i)=>console.log(i, x.error?'ERROR:'+x.error : 'OK len='+x.base64.length));"
mkdir -p /home/daytona/workspace/retrocalcaneal-ppt
~/retrocalcaneal-ppt/make_ppt.js
const pptxgen = require("pptxgenjs");
const { execSync } = require("child_process");
// ── Fetch all images ──────────────────────────────────────────────────────────
const imageUrls = [
"https://cdn.orris.care/cdss_images/2552b51a06c8a672790c07de779e7740ecda895a9121397a5dbe9030ffd1be7b.png", // Haglund X-ray
"https://cdn.orris.care/cdss_images/9b682c75f07ccfac7ba9b8d23ff7c9904f583b6b7c2192404d29d8fc94b2e094.png", // MRI Haglund syndrome triad
"https://cdn.orris.care/cdss_images/719c92d190cc775d327fad8c132f988df02c80348f8743f56d24d142ed9b3d16.png", // Pre/intraop radiograph
"https://cdn.orris.care/cdss_images/c77cd37ed2dea1c94a909acb623717a5af67bc5cdfce3b60828ec6eef9b15dd8.png", // Ultrasound Achilles
];
const imgs = JSON.parse(
execSync(
`node /home/daytona/skills/shared/scripts/fetch_images.js ${imageUrls.map(u => `"${u}"`).join(" ")}`
).toString()
);
const [imgXray, imgMRI, imgIntraop, imgUS] = imgs.map(i => i.base64);
// ── Theme colours ─────────────────────────────────────────────────────────────
const C = {
navy: "0D2B55",
teal: "0A7E8C",
gold: "E8A020",
white: "FFFFFF",
offwht: "F4F8FB",
lgray: "D0DCE8",
mgray: "7A8FA6",
red: "C0392B",
green: "1A7A4A",
orange: "E07020",
accent: "17A8C6",
};
// ── Presentation setup ────────────────────────────────────────────────────────
const pres = new pptxgen();
pres.layout = "LAYOUT_WIDE"; // 13.3 × 7.5
pres.title = "Retrocalcaneal Bursitis - Complete Guide";
pres.author = "Orris Medical";
// ══════════════════════════════════════════════════════════════════════════════
// HELPERS
// ══════════════════════════════════════════════════════════════════════════════
function addDarkBg(slide, leftColor = C.navy) {
slide.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 13.3, h: 7.5, fill: { color: leftColor }, line: { type: "none" }
});
}
function addSplitBg(slide, leftColor = C.navy, rightColor = C.offwht, split = 4.5) {
slide.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: split, h: 7.5, fill: { color: leftColor }, line: { type: "none" }
});
slide.addShape(pres.shapes.RECTANGLE, {
x: split, y: 0, w: 13.3 - split, h: 7.5, fill: { color: rightColor }, line: { type: "none" }
});
}
function addLightBg(slide) {
slide.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 13.3, h: 7.5, fill: { color: C.offwht }, line: { type: "none" }
});
}
function slideTitle(slide, title, sub = "", yPos = 0.22) {
// gold accent bar
slide.addShape(pres.shapes.RECTANGLE, {
x: 0.4, y: yPos - 0.02, w: 0.08, h: sub ? 0.9 : 0.55,
fill: { color: C.gold }, line: { type: "none" }
});
slide.addText(title, {
x: 0.6, y: yPos, w: 12.3, h: 0.55,
fontSize: 24, bold: true, color: C.navy, fontFace: "Calibri", margin: 0
});
if (sub) {
slide.addText(sub, {
x: 0.6, y: yPos + 0.55, w: 12.3, h: 0.32,
fontSize: 13, color: C.teal, fontFace: "Calibri", italic: true, margin: 0
});
}
}
function darkSlideTitle(slide, title, sub = "") {
slide.addShape(pres.shapes.RECTANGLE, {
x: 0.4, y: 0.22, w: 0.08, h: sub ? 0.9 : 0.55,
fill: { color: C.gold }, line: { type: "none" }
});
slide.addText(title, {
x: 0.6, y: 0.22, w: 12.3, h: 0.55,
fontSize: 24, bold: true, color: C.white, fontFace: "Calibri", margin: 0
});
if (sub) {
slide.addText(sub, {
x: 0.6, y: 0.77, w: 12.3, h: 0.32,
fontSize: 13, color: C.gold, fontFace: "Calibri", italic: true, margin: 0
});
}
}
function bullet(txt, marathi = "", indent = 0) {
const items = [
{ text: txt, options: { bullet: { type: "bullet" }, color: C.navy, fontSize: 13,
fontFace: "Calibri", bold: false, paraSpaceAfter: 2, indentLevel: indent } }
];
if (marathi) {
items.push({ text: " " + marathi, options: {
color: C.teal, fontSize: 11, italic: true, fontFace: "Noto Sans Devanagari",
paraSpaceAfter: 4, indentLevel: indent + 1, breakLine: true
}});
}
return items;
}
function infoBox(slide, x, y, w, h, heading, body, headColor = C.teal, bodyColor = C.navy) {
slide.addShape(pres.shapes.RECTANGLE, {
x, y, w, h, fill: { color: C.white },
line: { color: headColor, width: 1.5, type: "solid" },
shadow: { type: "outer", color: "000000", blur: 4, offset: 2, angle: 135, opacity: 0.1 }
});
slide.addShape(pres.shapes.RECTANGLE, {
x, y, w, h: 0.38, fill: { color: headColor }, line: { type: "none" }
});
slide.addText(heading, {
x: x + 0.1, y: y + 0.04, w: w - 0.2, h: 0.3,
fontSize: 11, bold: true, color: C.white, fontFace: "Calibri", margin: 0
});
slide.addText(body, {
x: x + 0.12, y: y + 0.42, w: w - 0.24, h: h - 0.5,
fontSize: 10.5, color: bodyColor, fontFace: "Calibri", valign: "top", margin: 0, wrap: true
});
}
function sectionDivider(slide, number, title, marathiTitle, colorL = C.teal) {
addDarkBg(slide, C.navy);
slide.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 0.5, h: 7.5, fill: { color: colorL }, line: { type: "none" }
});
slide.addShape(pres.shapes.RECTANGLE, {
x: 0.5, y: 3.1, w: 12.8, h: 1.4, fill: { color: colorL }, line: { type: "none" }
});
slide.addText(number, {
x: 0.7, y: 3.15, w: 1.5, h: 1.3,
fontSize: 64, bold: true, color: C.white, fontFace: "Calibri", valign: "middle", align: "left", margin: 0
});
slide.addText(title, {
x: 2.3, y: 3.18, w: 9.5, h: 0.72,
fontSize: 30, bold: true, color: C.white, fontFace: "Calibri", valign: "middle", align: "left", margin: 0
});
slide.addText(marathiTitle, {
x: 2.3, y: 3.88, w: 9.5, h: 0.5,
fontSize: 16, color: C.gold, fontFace: "Calibri", italic: true, margin: 0
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 1 — TITLE SLIDE
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addDarkBg(s, C.navy);
// Decorative teal band
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 5.5, w: 13.3, h: 2.0, fill: { color: C.teal }, line: { type: "none" }
});
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 5.4, w: 13.3, h: 0.15, fill: { color: C.gold }, line: { type: "none" }
});
// Title
s.addText("Retrocalcaneal Bursitis", {
x: 0.6, y: 1.1, w: 12.1, h: 1.1,
fontSize: 44, bold: true, color: C.white, fontFace: "Calibri",
align: "center", charSpacing: 1
});
// Marathi subtitle
s.addText("रेट्रोकॅल्केनियल बर्सायटिस", {
x: 0.6, y: 2.18, w: 12.1, h: 0.7,
fontSize: 26, color: C.gold, fontFace: "Calibri", align: "center", italic: true
});
// Tagline
s.addText("Anatomy • Pathophysiology • Diagnosis • Imaging • Management", {
x: 0.6, y: 2.95, w: 12.1, h: 0.45,
fontSize: 14, color: C.lgray, fontFace: "Calibri", align: "center", charSpacing: 2
});
// Marathi tagline
s.addText("शरीररचना • रोगनिर्मिती • निदान • प्रतिमाशास्त्र • उपचार", {
x: 0.6, y: 3.4, w: 12.1, h: 0.38,
fontSize: 12, color: C.accent, fontFace: "Calibri", align: "center", italic: true
});
// Footer
s.addText("Campbell's Operative Orthopaedics 15th Ed | Miller's Review | Goldman-Cecil Medicine | Grainger & Allison Radiology", {
x: 0.6, y: 5.55, w: 12.1, h: 0.4,
fontSize: 10, color: C.white, fontFace: "Calibri", align: "center"
});
s.addText("Orris Medical Reference | May 2026", {
x: 0.6, y: 5.98, w: 12.1, h: 0.32,
fontSize: 10, color: C.lgray, fontFace: "Calibri", align: "center"
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 2 — TABLE OF CONTENTS
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addLightBg(s);
slideTitle(s, "Table of Contents", "विषयसूची (Vishayasuchi)");
const topics = [
["1", "Anatomy & Bursal Architecture", "शरीररचना"],
["2", "Pathophysiology & Haglund Deformity", "रोगनिर्मिती"],
["3", "Clinical Presentation", "नैदानिक सादरीकरण"],
["4", "Imaging (X-ray, US, MRI)", "प्रतिमाशास्त्र"],
["5", "Differential Diagnosis", "विभेदक निदान"],
["6", "Non-operative Management", "शस्त्रक्रियारहित उपचार"],
["7", "Operative Management", "शस्त्रक्रिया उपचार"],
["8", "Radiological Measurements", "रेडिओलॉजिकल मोजमाप"],
["9", "Endoscopic Surgery & Outcomes", "दुर्बीण शस्त्रक्रिया"],
["10", "Physical Therapy Protocol", "भौतिक चिकित्सा"],
["11", "Special Populations", "विशेष रुग्णगट"],
];
const colW = 5.9;
const startX = [0.4, 6.8];
const startY = 1.2;
const rowH = 0.52;
topics.forEach(([num, eng, mar], i) => {
const col = i < 6 ? 0 : 1;
const row = i < 6 ? i : i - 6;
const x = startX[col];
const y = startY + row * rowH;
s.addShape(pres.shapes.RECTANGLE, {
x, y, w: colW, h: rowH - 0.06,
fill: { color: i % 2 === 0 ? C.white : "EDF3F8" },
line: { color: C.lgray, width: 0.5 },
shadow: { type: "outer", color: "000000", blur: 2, offset: 1, angle: 135, opacity: 0.07 }
});
s.addShape(pres.shapes.RECTANGLE, {
x, y, w: 0.38, h: rowH - 0.06,
fill: { color: C.teal }, line: { type: "none" }
});
s.addText(num, {
x, y: y + 0.06, w: 0.38, h: rowH - 0.18,
fontSize: 13, bold: true, color: C.white, align: "center", fontFace: "Calibri", margin: 0
});
s.addText(eng, {
x: x + 0.44, y: y + 0.04, w: colW - 0.52, h: 0.27,
fontSize: 12, bold: true, color: C.navy, fontFace: "Calibri", margin: 0
});
s.addText(mar, {
x: x + 0.44, y: y + 0.28, w: colW - 0.52, h: 0.2,
fontSize: 10, italic: true, color: C.teal, fontFace: "Calibri", margin: 0
});
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SECTION DIVIDER — ANATOMY
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
sectionDivider(s, "01", "Anatomy & Bursal Architecture", "शरीररचना व बर्साची रचना", C.teal);
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 3 — ANATOMY
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addLightBg(s);
slideTitle(s, "Anatomy of the Retrocalcaneal Bursa", "रेट्रोकॅल्केनियल बर्साची शरीररचना");
// Left column — text
s.addText([
...bullet("Synovial bursa located DEEP to Achilles tendon", "अकिलीस कंडराच्या खाली असलेली सायनोव्हियल पिशवी"),
...bullet("Between Achilles tendon & posterosuperior calcaneal tuberosity", "अकिलीस कंडरा व कॅल्केनियसच्या वरच्या मागील बाजूमध्ये"),
...bullet("Part of the Achilles Entheseal Organ:", "अकिलीस एन्थेसल ऑर्गनचा भाग:"),
...bullet("→ Fibrocartilage on anterior tendon surface", "", 1),
...bullet("→ Fibrocartilage on calcaneal surface", "", 1),
...bullet("→ Retrocalcaneal bursa (space between)", "", 1),
...bullet("→ Kager's fat pad (synovial-lined, slides in/out with ankle motion)", "कागरचा फॅट पॅड", 1),
...bullet("→ Underlying trabecular bone", "", 1),
...bullet("Prime enthesitis site in Spondyloarthropathy (SpA)", "स्पॉन्डिलोआर्थ्रोपॅथीमध्ये प्रमुख ठिकाण"),
], {
x: 0.4, y: 1.15, w: 6.5, h: 6.0,
fontSize: 12, color: C.navy, fontFace: "Calibri", valign: "top"
});
// Right column — Two Bursae table
const bx = 7.2;
s.addText("Two Clinically Important Bursae", {
x: bx, y: 1.15, w: 5.7, h: 0.36,
fontSize: 13, bold: true, color: C.navy, fontFace: "Calibri", margin: 0
});
s.addText("दोन महत्त्वाच्या बर्सा", {
x: bx, y: 1.48, w: 5.7, h: 0.26,
fontSize: 11, italic: true, color: C.teal, fontFace: "Calibri", margin: 0
});
infoBox(s, bx, 1.8, 5.7, 1.6,
"Retrocalcaneal Bursa (Deep) | रेट्रोकॅल्केनियल बर्सा (खोल)",
"Between Achilles tendon and posterosuperior calcaneus.\nClinically more significant.\nAffected in Haglund syndrome & SpA.",
C.teal
);
infoBox(s, bx, 3.5, 5.7, 1.6,
"Retroachilles Bursa (Superficial) | रेट्रोअकिलीस बर्सा (वरवरची)",
"Between Achilles tendon and overlying skin.\nIrritated by stiff shoe heel counters.\nAlso called pre-tendinous / subcutaneous bursa.",
C.orange
);
infoBox(s, bx, 5.2, 5.7, 1.85,
"Systemic Associations | प्रणालीगत कारणे",
"• Spondyloarthritis (SpA) — prime entheseal site\n• Rheumatoid Arthritis (RA)\n• Gout — urate crystal deposition\n• CPPD disease\n• Ochronosis (homogentisic acid)\n• Fluoroquinolone-induced tendinopathy",
C.red
);
}
// ══════════════════════════════════════════════════════════════════════════════
// SECTION DIVIDER — PATHOPHYSIOLOGY
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
sectionDivider(s, "02", "Pathophysiology & Haglund Deformity", "रोगनिर्मिती व हॅग्लंड विकृती", C.orange);
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 4 — PATHOPHYSIOLOGY + HAGLUND X-RAY
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addSplitBg(s, C.navy, C.offwht, 5.2);
darkSlideTitle(s, "Pathophysiology & Haglund Deformity", "रोगनिर्मिती");
s.addText([
{ text: "Haglund Deformity", options: { bold: true, color: C.gold, fontSize: 14, breakLine: true } },
{ text: "हॅग्लंड विकृती", options: { italic: true, color: C.accent, fontSize: 12, breakLine: true } },
{ text: " ", options: { fontSize: 6, breakLine: true } },
{ text: "• Large exostosis off posterosuperior calcaneal tuberosity (ANTERIOR to Achilles tendon)\n", options: { color: C.white, fontSize: 12 } },
{ text: "• Repeated dorsiflexion → tendon abraded against tuberosity\n", options: { color: C.white, fontSize: 12 } },
{ text: "• Chronic microtrauma → bursal inflammation\n", options: { color: C.white, fontSize: 12 } },
{ text: "• Prolonged inflammation → degenerative changes + osteophytes\n\n", options: { color: C.white, fontSize: 12 } },
{ text: "Cascade of Events | घटनाक्रम:\n", options: { bold: true, color: C.gold, fontSize: 13, breakLine: true } },
], { x: 0.35, y: 1.2, w: 4.65, h: 5.9, fontFace: "Calibri", valign: "top" });
// Cascade boxes
const cascade = [
["Haglund Exostosis", "हॅग्लंड एक्झोस्टोसिस", C.orange],
["Mechanical Impingement", "यांत्रिक दाब", C.teal],
["Bursal Inflammation", "बर्साची जळजळ", C.red],
["Tendinosis + Osteophytes", "टेंडिनोसिस + अस्थिवृद्धी", C.mgray],
];
cascade.forEach(([eng, mar, col], i) => {
const y = 1.5 + i * 1.1;
s.addShape(pres.shapes.RECTANGLE, {
x: 0.4, y: y + 1.3, w: 4.3, h: 0.62,
fill: { color: col }, line: { type: "none" },
shadow: { type: "outer", color: "000000", blur: 4, offset: 2, angle: 135, opacity: 0.2 }
});
s.addText(eng + "\n" + mar, {
x: 0.4, y: y + 1.3, w: 4.3, h: 0.62,
fontSize: 11.5, bold: true, color: C.white, align: "center", valign: "middle",
fontFace: "Calibri"
});
if (i < 3) {
s.addShape(pres.shapes.RECTANGLE, {
x: 2.35, y: y + 1.92, w: 0.5, h: 0.18,
fill: { color: C.gold }, line: { type: "none" }
});
}
});
// Right side — X-ray image
if (imgXray) {
s.addImage({ data: imgXray, x: 5.4, y: 1.0, w: 7.5, h: 5.8 });
}
s.addText("Lateral Heel X-ray: Haglund deformity (box) + Insertional Achilles Spur (arrow)\nपार्श्व टाच क्ष-किरण: हॅग्लंड विकृती (चौकट) + अकिलीस स्पर (बाण)", {
x: 5.4, y: 6.8, w: 7.5, h: 0.55,
fontSize: 9.5, color: C.mgray, fontFace: "Calibri", italic: true, align: "center"
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SECTION DIVIDER — CLINICAL PRESENTATION
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
sectionDivider(s, "03", "Clinical Presentation", "नैदानिक सादरीकरण", C.green);
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 5 — CLINICAL PRESENTATION
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addLightBg(s);
slideTitle(s, "Clinical Presentation", "नैदानिक सादरीकरण — लक्षणे व चिन्हे");
// Symptoms box
infoBox(s, 0.4, 1.15, 6.0, 2.8,
"Symptoms | लक्षणे",
"• Deep posterior heel pain (खोल मागील टाचदुखी)\n• Insidious onset — NOT acute\n• Morning pain / stiffness on first steps\n (सकाळी पहिल्या पावलांवर वेदना)\n• Worse with ankle dorsiflexion\n (घोट्याच्या वरच्या दिशेने हालचालीत वाढते)\n• Difficulty wearing closed-back shoes\n (बंद टाचेचे शूज घालण्यात अडचण)\n• Visible posterior heel swelling / bony bump",
C.teal
);
// Signs box
infoBox(s, 0.4, 4.1, 6.0, 2.85,
"Physical Signs | शारीरिक चिन्हे",
"• Mediolateral tenderness ANTERIOR to Achilles tendon\n (अकिलीस कंडराच्या आधी मध्य-पार्श्व कोमलता)\n• Fluid fluctuation test (द्रव चाचणी):\n Thumb + index finger on each side of tendon;\n other index presses over tendon → perceive fluctuation\n• Palpable Haglund bony prominence\n• Gastrosoleus contracture on exam\n (गॅस्ट्रोसोलियस आकुंचन)\n• Increased pain with passive dorsiflexion",
C.orange
);
// Key Distinction box
infoBox(s, 6.65, 1.15, 6.25, 2.0,
"Key Clinical Distinction | महत्त्वाचा फरक",
"Pain on FIRST ARISING in morning\n→ Retrocalcaneal bursitis / Achilles tendinopathy\n\nPain ONLY WITH SHOES\n→ Pretendinous (superficial) bursitis",
C.navy
);
// Warning box fluoroquinolone
infoBox(s, 6.65, 3.3, 6.25, 1.8,
"⚠ Fluoroquinolone Warning | सावधान",
"Ciprofloxacin / Levofloxacin can cause Achilles\ntendinopathy ± rupture — during or weeks AFTER use.\nIMPORTANT: Stop drug immediately if recognised!\n(फ्लुरोक्विनोलोन चालू असताना अकिलीस कंडरा फुटण्याचा धोका)",
C.red
);
// Haglund syndrome triad
s.addShape(pres.shapes.RECTANGLE, {
x: 6.65, y: 5.2, w: 6.25, h: 1.75,
fill: { color: "EAF6FF" }, line: { color: C.teal, width: 1 }
});
s.addText("Haglund Syndrome Triad | हॅग्लंड सिंड्रोम त्रिकूट", {
x: 6.75, y: 5.25, w: 6.05, h: 0.32,
fontSize: 12, bold: true, color: C.navy, fontFace: "Calibri", margin: 0
});
s.addText(
"1. Insertional Achilles Tendinopathy\n2. Retrocalcaneal Bursitis\n3. Posterosuperior Calcaneal Exostosis (Haglund deformity)",
{ x: 6.75, y: 5.6, w: 6.05, h: 1.2, fontSize: 11.5, color: C.navy, fontFace: "Calibri" }
);
}
// ══════════════════════════════════════════════════════════════════════════════
// SECTION DIVIDER — IMAGING
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
sectionDivider(s, "04", "Imaging", "प्रतिमाशास्त्र — क्ष-किरण, अल्ट्रासाउंड, MRI", C.accent);
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 6 — X-RAY + MEASUREMENTS
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addSplitBg(s, C.offwht, C.navy, 6.9);
slideTitle(s, "Plain Radiograph — Lateral Heel X-ray", "पार्श्व टाच क्ष-किरण");
s.addText([
...bullet("Standing lateral view — FIRST-LINE imaging", "उभे राहून पार्श्व दृश्य — प्रथम पसंती"),
...bullet("Shows: Haglund deformity, insertional spur, calcification", "दाखवते: हॅग्लंड विकृती, स्पर, कॅल्सिफिकेशन"),
{ text: "\nRadiological Measurements | रेडिओलॉजिकल मोजमाप:\n", options: { bold: true, color: C.navy, fontSize: 13, fontFace: "Calibri", breakLine: true } },
...bullet("Fowler-Philip Angle: >75° = abnormal (normal <69°)", "फॉलर-फिलिप कोन: >७५° = असामान्य"),
...bullet("Parallel Pitch Lines (PPL): calcaneal process projects above upper line = Haglund", "समांतर पिच रेषा"),
...bullet("Calcaneal Pitch Angle: ↑ angle associated with insertional tendinopathy", "कॅल्केनियल पिच कोन"),
{ text: "\n⚠ Caveat:", options: { bold: true, color: C.red, fontSize: 12, fontFace: "Calibri", breakLine: true } },
...bullet("Haglund size is NOT statistically different between symptomatic patients and controls!", "हॅग्लंड आकार आणि लक्षणे यांचा थेट संबंध नाही!"),
...bullet("Insertional osteophyte + calcaneal pitch angle have stronger association", ""),
], {
x: 0.4, y: 1.15, w: 6.2, h: 6.1,
fontSize: 12, color: C.navy, fontFace: "Calibri", valign: "top"
});
// X-ray image on right
if (imgXray) {
s.addImage({ data: imgXray, x: 7.1, y: 0.9, w: 5.9, h: 5.6 });
}
s.addText("Haglund deformity (box) + Insertional Achilles spur (arrow)\nहॅग्लंड विकृती (चौकट) + अकिलीस स्पर (बाण)\nSource: Campbell's Operative Orthopaedics 15th Ed", {
x: 7.1, y: 6.52, w: 5.9, h: 0.65,
fontSize: 9, color: C.lgray, italic: true, fontFace: "Calibri", align: "center"
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 7 — MRI IMAGING
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addLightBg(s);
slideTitle(s, "MRI & Ultrasound Imaging", "MRI व अल्ट्रासाउंड प्रतिमाशास्त्र");
// MRI image
if (imgMRI) {
s.addImage({ data: imgMRI, x: 0.4, y: 1.1, w: 4.5, h: 5.6 });
}
s.addText("Sagittal PD fat-sat MRI — Haglund Syndrome:\nInsertional tendinopathy (→), Retrocalcaneal bursitis (short →), Haglund exostosis (*)\nसॅजिटल MRI: हॅग्लंड सिंड्रोम त्रिकूट\nSource: Grainger & Allison's Diagnostic Radiology", {
x: 0.4, y: 6.72, w: 4.5, h: 0.65,
fontSize: 8.5, italic: true, color: C.mgray, fontFace: "Calibri", align: "center"
});
// Ultrasound image
if (imgUS) {
s.addImage({ data: imgUS, x: 5.1, y: 1.1, w: 4.2, h: 5.0 });
}
s.addText("Ultrasound: Achilles tendinopathy (*) with retrocalcaneal bursitis\nDoppler = new vessel formation\nअल्ट्रासाउंड: अकिलीस टेंडिनोपॅथी + रेट्रोकॅल्केनियल बर्सायटिस\nSource: Grainger & Allison Radiology", {
x: 5.1, y: 6.12, w: 4.2, h: 0.78,
fontSize: 8.5, italic: true, color: C.mgray, fontFace: "Calibri", align: "center"
});
// MRI vs US comparison
infoBox(s, 9.55, 1.1, 3.35, 2.5,
"MRI Indications | MRI कधी?",
"• Quantify tendinosis extent\n• Rule out partial tear\n• Pre-op: confirm <50% tendinosis\n (for Zadek osteotomy)\n• Rarely needed for diagnosis alone\n (निदानासाठी क्वचितच लागते)",
C.teal
);
infoBox(s, 9.55, 3.75, 3.35, 2.5,
"Ultrasound Advantages | US फायदे",
"• Real-time, dynamic imaging\n• Cheap & widely available\n• Bursal fluid (anechoic collection)\n• Doppler: hyperaemia in active\n inflammation\n• No radiation\n (रेडिएशन नाही)",
C.green
);
}
// ══════════════════════════════════════════════════════════════════════════════
// SECTION DIVIDER — DIFFERENTIAL DIAGNOSIS
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
sectionDivider(s, "05", "Differential Diagnosis", "विभेदक निदान", C.red);
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 8 — DIFFERENTIAL DIAGNOSIS TABLE
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addLightBg(s);
slideTitle(s, "Differential Diagnosis of Posterior Heel Pain", "मागील टाचदुखीचे विभेदक निदान");
const rows = [
["Condition", "Key Feature", "Distinguishing Sign", "Treatment Difference"],
["Retrocalcaneal Bursitis\n(रेट्रोकॅल्केनियल बर्सायटिस)", "Deep, anterior to Achilles", "Mediolateral fluctuation test +ve", "Avoid steroid near tendon"],
["Insertional Achilles\nTendinopathy", "Midline tenderness at insertion", "Tender directly OVER tendon", "Eccentric loading"],
["Pretendinous Bursitis\n(वरवरची बर्सायटिस)", "Pain ONLY with closed-back shoes", "Superficial, posterior to tendon", "Shoe modification"],
["Plantar Fasciitis\n(प्लांटर फॅसिटिस)", "Plantar heel, worst first step", "Medial calcaneal tubercle tender", "Plantar stretch"],
["Sever's Disease\n(मुलांमध्ये - सेव्हर आजार)", "Children 7-10 yrs, activity pain", "Posterior heel apophysis tender", "Rest, self-limiting"],
["Gout / CPPD\n(गाउट)", "Acute attack, red hot joint", "Serum uric acid ↑, crystals", "Colchicine / NSAIDs"],
["Spondyloarthropathy\n(स्पॉन्डिलोआर्थ्रोपॅथी)", "Bilateral, systemic features", "HLA-B27, bilateral enthesitis", "DMARDs / biologics"],
["Achilles Tendon Rupture\n(फाटलेला कंडरा)", "Acute onset, pop felt", "Thompson test +ve, palpable gap", "Surgery / boot"],
];
const colW = [3.0, 2.8, 3.3, 3.7];
const colX = [0.3, 3.35, 6.2, 9.55];
const rowH = 0.56;
rows.forEach((row, ri) => {
row.forEach((cell, ci) => {
const isHeader = ri === 0;
s.addShape(pres.shapes.RECTANGLE, {
x: colX[ci], y: 1.15 + ri * rowH, w: colW[ci], h: rowH,
fill: { color: isHeader ? C.teal : ri % 2 === 0 ? C.white : "EDF3F8" },
line: { color: C.lgray, width: 0.5 }
});
s.addText(cell, {
x: colX[ci] + 0.08, y: 1.18 + ri * rowH, w: colW[ci] - 0.16, h: rowH - 0.06,
fontSize: isHeader ? 11 : 10, bold: isHeader,
color: isHeader ? C.white : ci === 0 ? C.navy : C.mgray,
fontFace: "Calibri", valign: "middle"
});
});
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SECTION DIVIDER — MANAGEMENT
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
sectionDivider(s, "06", "Non-operative Management", "शस्त्रक्रियारहित उपचार", C.green);
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 9 — NON-OPERATIVE MANAGEMENT
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addLightBg(s);
slideTitle(s, "Non-operative Management", "शस्त्रक्रियारहित उपचार — ३-६ महिने प्रयत्न करावेत");
infoBox(s, 0.4, 1.15, 4.0, 2.1,
"Mechanical | यांत्रिक उपाय",
"• Heel lift orthotics (टाच उशी)\n• Open-back shoes (मागे उघड्या चपला)\n• Silicone heel pad / doughnut pad\n• Activity modification\n• 3D walking boot (acute flares)",
C.teal
);
infoBox(s, 4.65, 1.15, 4.0, 2.1,
"Pharmacological | औषधोपचार",
"• NSAIDs — oral or topical\n (दाहविरोधी औषधे)\n• Short course only\n• Topical diclofenac gel useful",
C.orange
);
infoBox(s, 9.3, 1.15, 3.6, 2.1,
"Immobilisation | स्थिरीकरण",
"• Walking boot for acute\n inflammation\n• Short-leg cast for\n recalcitrant cases\n• Night splint for morning pain",
C.navy
);
infoBox(s, 0.4, 3.4, 4.0, 2.2,
"Physical Therapy | भौतिक चिकित्सा",
"• Eccentric heel drops\n (एकाग्र टाच खाली करणे)\n• Heavy slow resistance (HSR)\n• Gastrosoleus stretching\n• Dry needling\n• Astym therapy",
C.green
);
infoBox(s, 4.65, 3.4, 4.0, 2.2,
"ESWT | शॉक वेव्ह थेरपी",
"• Low-energy extracorporeal\n shock wave therapy\n• For chronic cases (>6 weeks)\n• Good evidence for insertional\n tendinopathy + bursitis\n (जुनाट बर्सायटिससाठी उपयुक्त)",
C.accent
);
// Red box — avoid steroid
s.addShape(pres.shapes.RECTANGLE, {
x: 9.3, y: 3.4, w: 3.6, h: 2.2,
fill: { color: "FFF0F0" }, line: { color: C.red, width: 2 }
});
s.addShape(pres.shapes.RECTANGLE, {
x: 9.3, y: 3.4, w: 3.6, h: 0.38, fill: { color: C.red }, line: { type: "none" }
});
s.addText("⚠ AVOID | टाळावे", {
x: 9.4, y: 3.44, w: 3.4, h: 0.3,
fontSize: 12, bold: true, color: C.white, fontFace: "Calibri", margin: 0
});
s.addText("Corticosteroid injection\nnear Achilles tendon!\n(कॉर्टिकोस्टेरॉइड इंजेक्शन\nअकिलीस कंडराजवळ देऊ नये)\n→ Risk of tendon RUPTURE\n→ Repeated injections = danger!\n\nPRP: Inconclusive evidence\n(PRP: अपुरा पुरावा)", {
x: 9.4, y: 3.84, w: 3.4, h: 1.7,
fontSize: 10.5, color: C.red, fontFace: "Calibri", bold: true
});
// Duration note
s.addShape(pres.shapes.RECTANGLE, {
x: 0.4, y: 5.75, w: 12.5, h: 0.65,
fill: { color: C.teal }, line: { type: "none" }
});
s.addText("⏱ Try conservative treatment for MINIMUM 3-6 months before considering surgery | शस्त्रक्रियेपूर्वी किमान ३-६ महिने पुराणमतवादी उपचार करावेत", {
x: 0.55, y: 5.82, w: 12.2, h: 0.5,
fontSize: 12.5, bold: true, color: C.white, fontFace: "Calibri", align: "center"
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 10 — PHYSICAL THERAPY PROTOCOL (DETAILED)
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addLightBg(s);
slideTitle(s, "Physical Therapy Protocol — 3 Phases", "भौतिक चिकित्सा — ३ टप्पे");
const phases = [
{
title: "Phase 1 — Acute (Weeks 1-4)",
marathi: "टप्पा १ — तीव्र अवस्था (आठवडे १-४)",
color: C.red,
content: "• Rest + activity modification\n• Ice 15-20 min, 3-4x daily (बर्फ शेक)\n• NSAIDs / topical anti-inflammatories\n• Heel lift in shoe (टाच उशी)\n• Night splint if morning pain\n• Walking boot for severe flares\n (तीव्र वेदनांसाठी वॉकिंग बूट)",
},
{
title: "Phase 2 — Subacute / Loading (Weeks 4-12)",
marathi: "टप्पा २ — भार टाकण्याचा टप्पा (आठवडे ४-१२)",
color: C.orange,
content: "• Eccentric heel drops (एकाग्र टाच व्यायाम):\n Stand on step edge, rise bilateral,\n lower on AFFECTED leg slowly\n 3 sets × 15 reps, twice daily\n Straight knee (gastrocnemius)\n Bent knee (soleus)\n• Heavy Slow Resistance (HSR) training\n• Gastrosoleus stretch\n• Astym / dry needling\n• ESWT from week 6+ if needed",
},
{
title: "Phase 3 — Return to Sport (Week 12+)",
marathi: "टप्पा ३ — खेळात परतणे (आठवडा १२+)",
color: C.green,
content: "• Progressive plyometric loading\n (हळूहळू उडी-प्रकारचे व्यायाम)\n• Sport-specific drills\n• Footwear optimisation\n (योग्य बूट निवड)\n• Continue ESWT if needed\n• Gradually increase training load",
},
];
phases.forEach((ph, i) => {
const x = 0.4 + i * 4.3;
s.addShape(pres.shapes.RECTANGLE, {
x, y: 1.15, w: 4.1, h: 5.9,
fill: { color: C.white },
line: { color: ph.color, width: 2 },
shadow: { type: "outer", color: "000000", blur: 5, offset: 2, angle: 135, opacity: 0.1 }
});
s.addShape(pres.shapes.RECTANGLE, {
x, y: 1.15, w: 4.1, h: 0.9,
fill: { color: ph.color }, line: { type: "none" }
});
s.addText(ph.title, {
x: x + 0.1, y: 1.18, w: 3.9, h: 0.48,
fontSize: 12, bold: true, color: C.white, fontFace: "Calibri", margin: 0
});
s.addText(ph.marathi, {
x: x + 0.1, y: 1.65, w: 3.9, h: 0.35,
fontSize: 10, italic: true, color: C.white, fontFace: "Calibri", margin: 0
});
s.addText(ph.content, {
x: x + 0.15, y: 2.15, w: 3.8, h: 4.8,
fontSize: 11, color: C.navy, fontFace: "Calibri", valign: "top"
});
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SECTION DIVIDER — OPERATIVE
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
sectionDivider(s, "07", "Operative Management", "शस्त्रक्रिया उपचार", C.navy);
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 11 — OPERATIVE OPTIONS (with intraop image)
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addSplitBg(s, C.navy, C.offwht, 5.5);
darkSlideTitle(s, "Operative Management", "शस्त्रक्रिया उपचार — अपयशी पुराणमतवादी उपचारानंतर");
s.addText([
{ text: "Indications | संकेत:\n", options: { bold: true, color: C.gold, fontSize: 13, breakLine: true } },
{ text: "• Failure of 3-6 months conservative care\n", options: { color: C.white, fontSize: 11 } },
{ text: "• Intractable posterior heel pain\n\n", options: { color: C.white, fontSize: 11 } },
{ text: "MRI before surgery: Quantify tendinosis\n", options: { bold: true, color: C.gold, fontSize: 12, breakLine: true } },
{ text: "• <50% tendinosis → Endoscopic / Zadek\n", options: { color: C.white, fontSize: 11 } },
{ text: "• >50% tendinosis → Debridement + FHL transfer\n\n", options: { color: C.white, fontSize: 11 } },
{ text: "Procedures | प्रक्रिया:\n", options: { bold: true, color: C.gold, fontSize: 13, breakLine: true } },
{ text: "1. Endoscopic Calcaneoplasty\n", options: { bold: true, color: C.accent, fontSize: 12, breakLine: true } },
{ text: " Preferred — 80-100% good/excellent results\n (दुर्बीण शस्त्रक्रिया — प्रथम पसंती)\n\n", options: { color: C.white, fontSize: 11 } },
{ text: "2. Zadek Osteotomy (Dorsal Closing Wedge)\n", options: { bold: true, color: C.accent, fontSize: 12, breakLine: true } },
{ text: " <50% tendinosis; reduces calcaneal pitch\n\n", options: { color: C.white, fontSize: 11 } },
{ text: "3. Open Debridement + Exostectomy\n", options: { bold: true, color: C.gold, fontSize: 12, breakLine: true } },
{ text: " For >50% tendinosis cases\n\n", options: { color: C.white, fontSize: 11 } },
{ text: "4. FHL Tendon Transfer (Augmentation)\n", options: { bold: true, color: C.gold, fontSize: 12, breakLine: true } },
{ text: " If >50% Achilles footprint debrided\n", options: { color: C.white, fontSize: 11 } },
], { x: 0.4, y: 1.15, w: 4.8, h: 6.1, fontFace: "Calibri", valign: "top" });
// Right — intraop image
if (imgIntraop) {
s.addImage({ data: imgIntraop, x: 5.8, y: 1.0, w: 5.0, h: 4.0 });
}
s.addText("Pre- and intraoperative radiographs — Haglund deformity excision\nहॅग्लंड विकृतीची शस्त्रक्रिया — पूर्व व दरम्यान क्ष-किरण\nSource: Miller's Review of Orthopaedics 9th Ed", {
x: 5.8, y: 5.02, w: 5.0, h: 0.55,
fontSize: 8.5, italic: true, color: C.mgray, fontFace: "Calibri", align: "center"
});
infoBox(s, 5.8, 5.65, 7.1, 1.65,
"Gastrocnemius Recession | गॅस्ट्रोकनेमियस लांबवणे",
"For cases with significant gastrosoleus contracture. Endoscopic > Open (fewer wound complications). Phisitkul prospective study: 320 patients — improved dorsiflexion + pain scores at 1 yr. Associated with plantarflexion weakness at 18 months.",
C.mgray
);
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 12 — ENDOSCOPIC vs OPEN (Evidence Table)
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addLightBg(s);
slideTitle(s, "Endoscopic vs Open Surgery — Evidence", "दुर्बीण वि. उघडी शस्त्रक्रिया — पुरावा");
// Systematic review citation
s.addShape(pres.shapes.RECTANGLE, {
x: 0.4, y: 1.1, w: 12.5, h: 0.55,
fill: { color: C.teal }, line: { type: "none" }
});
s.addText("Systematic Review: Alessio-Mazzola et al. (KSSTA 2021) — 1,260 ankles, 1,147 patients | PMID: 33216187", {
x: 0.55, y: 1.15, w: 12.2, h: 0.42,
fontSize: 11, bold: true, color: C.white, fontFace: "Calibri", align: "center"
});
const cols = ["Outcome", "Open Surgery", "Endoscopic Surgery", "p-value"];
const data = [
["AOFAS Score", "87.1 ± 5.9", "90.7 ± 4.2", "< 0.001"],
["Complication Rate", "15.5%", "4.1%", "< 0.001"],
["Failure Rate", "6.0%", "1.2%", "< 0.001"],
["Return to Daily Activities", "17.2 weeks", "6.3 weeks", "< 0.001"],
["Return to Sport", "20.7 weeks", "11.9 weeks", "< 0.001"],
];
const cw = [3.8, 2.8, 3.2, 2.5];
const cx = [0.4, 4.25, 7.1, 10.35];
const rh = 0.62;
[...[cols], ...data].forEach((row, ri) => {
row.forEach((cell, ci) => {
const isHeader = ri === 0;
const isBetter = !isHeader && ci === 2;
s.addShape(pres.shapes.RECTANGLE, {
x: cx[ci], y: 1.75 + ri * rh, w: cw[ci], h: rh,
fill: { color: isHeader ? C.navy : isBetter ? "E8F9F0" : ri % 2 === 0 ? C.white : "F2F6FA" },
line: { color: C.lgray, width: 0.5 }
});
s.addText(cell, {
x: cx[ci] + 0.1, y: 1.78 + ri * rh, w: cw[ci] - 0.2, h: rh - 0.08,
fontSize: isHeader ? 12 : 12.5, bold: isHeader || isBetter,
color: isHeader ? C.white : isBetter ? C.green : ci === 3 ? C.red : C.navy,
fontFace: "Calibri", align: "center", valign: "middle"
});
});
});
// Advantages list
infoBox(s, 0.4, 5.42, 5.8, 1.83,
"Advantages of Endoscopic Approach | दुर्बीण शस्त्रक्रियेचे फायदे",
"• 4× lower complication rate\n• 5× lower failure rate\n• Return to sport almost HALF the time\n• Smaller incisions, better cosmesis\n• Lower sural nerve injury risk\n(कमी गुंतागुंत, जलद पुनर्प्राप्ती, कमी चट्टा)",
C.green
);
infoBox(s, 6.55, 5.42, 6.35, 1.83,
"Zadek Osteotomy Evidence | झाडेक ऑस्टिओटॉमी",
"Poutoglidou et al. Systematic Review + Meta-analysis (Foot Ankle Surg 2023) — PMID: 37088671\nGood outcomes at 2 years. Best for <50% intrasubstance tendinosis on MRI. Minimally invasive approach preferred: fewer wound complications + lower sural nerve injury.\n(५०% पेक्षा कमी टेंडिनोसिससाठी उत्तम — जखमेचे कमी प्रश्न)",
C.teal
);
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 13 — SPECIAL POPULATIONS
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addLightBg(s);
slideTitle(s, "Special Populations & Clinical Pearls", "विशेष रुग्णगट व महत्त्वाचे मुद्दे");
infoBox(s, 0.4, 1.15, 6.1, 1.95,
"Athletes | खेळाडू",
"High return-to-sport demand → endoscopic approach preferred.\nEccentric training (Alfredson protocol) for 12 weeks before surgery.\n'Pump bump' — Haglund classically described in women's high-heeled shoes.\n(खेळाडूंसाठी दुर्बीण शस्त्रक्रिया उत्तम — जलद परत येणे)",
C.teal
);
infoBox(s, 6.75, 1.15, 6.15, 1.95,
"Spondyloarthropathy / RA | स्पॉन्डिलोआर्थ्रोपॅथी / RA",
"Systemic DMARDs / biologics (anti-TNF, anti-IL17) required.\nBilateral presentation → always suspect systemic cause.\nCorticosteroid injection more acceptable in inflammatory arthritis\n(synovitis not tendinosis).\n(द्विपक्षीय असेल तर प्रणालीगत कारण शोधा)",
C.orange
);
infoBox(s, 0.4, 3.25, 6.1, 1.95,
"Children — Sever's Disease | मुलांमध्ये — सेव्हर आजार",
"True retrocalcaneal bursitis rare in children.\nSever's disease (calcaneal apophysitis): ages 7-10, activity-related posterior heel.\nTreatment: Rest, ice, heel pads — self-limiting.\nX-rays NOT needed unless other diagnosis suspected.\n(बहुतांश वेळी हा आजार स्वतःहून बरा होतो)",
C.green
);
infoBox(s, 6.75, 3.25, 6.15, 1.95,
"Gout / Crystal Arthropathy | गाउट",
"Urate crystals may deposit in retrocalcaneal bursa.\nAcute attacks → colchicine / NSAIDs / corticosteroid (in bursa, not tendon).\nSerum uric acid, joint aspirate for crystals.\nRheumatoid arthritis can also affect the bursa.\n(युरेट क्रिस्टल बर्सात साचतात — तीव्र वेदना)",
C.red
);
// Fluoroquinolone big warning
s.addShape(pres.shapes.RECTANGLE, {
x: 0.4, y: 5.35, w: 12.5, h: 1.9,
fill: { color: "FFF3CD" }, line: { color: C.orange, width: 2 }
});
s.addShape(pres.shapes.RECTANGLE, {
x: 0.4, y: 5.35, w: 12.5, h: 0.42, fill: { color: C.orange }, line: { type: "none" }
});
s.addText("⚠ Fluoroquinolone-Induced Tendinopathy | फ्लुरोक्विनोलोन-प्रेरित टेंडिनोपॅथी", {
x: 0.55, y: 5.38, w: 12.2, h: 0.35,
fontSize: 12, bold: true, color: C.white, fontFace: "Calibri", align: "center", margin: 0
});
s.addText(
"Ciprofloxacin / Levofloxacin → Achilles tendinopathy ± rupture | Can occur during or WEEKS AFTER drug use\n" +
"STOP fluoroquinolone IMMEDIATELY on recognition | Inform patient before prescribing!\n" +
"फ्लुरोक्विनोलोन वापरताना किंवा वापरल्यानंतर काही आठवड्यांनी कंडरा फुटण्याचा धोका — औषध त्वरित बंद करावे",
{
x: 0.55, y: 5.82, w: 12.2, h: 1.3,
fontSize: 11.5, color: C.navy, fontFace: "Calibri", align: "center"
}
);
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 14 — MANAGEMENT ALGORITHM
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addLightBg(s);
slideTitle(s, "Management Algorithm", "उपचाराचा मार्गदर्शक आराखडा");
// Flow boxes
const boxes = [
{ x: 4.3, y: 1.1, w: 4.7, h: 0.6, text: "Posterior Heel Pain\nमागील टाचदुखी", col: C.navy },
{ x: 4.3, y: 1.9, w: 4.7, h: 0.6, text: "Clinical Exam + Standing Lateral X-ray\nशारीरिक तपासणी + क्ष-किरण", col: C.teal },
{ x: 4.3, y: 2.7, w: 4.7, h: 0.6, text: "Systemic Cause? (SpA/RA/Gout)\nप्रणालीगत कारण?", col: C.orange },
];
boxes.forEach(b => {
s.addShape(pres.shapes.RECTANGLE, {
x: b.x, y: b.y, w: b.w, h: b.h,
fill: { color: b.col }, line: { type: "none" },
shadow: { type: "outer", color: "000000", blur: 4, offset: 2, angle: 135, opacity: 0.15 }
});
s.addText(b.text, {
x: b.x + 0.1, y: b.y, w: b.w - 0.2, h: b.h,
fontSize: 11.5, bold: true, color: C.white, fontFace: "Calibri",
align: "center", valign: "middle"
});
});
// Arrows between boxes
[1.7, 2.5, 3.3].forEach(y => {
s.addShape(pres.shapes.RECTANGLE, { x: 6.5, y, w: 0.3, h: 0.2, fill: { color: C.gold }, line: { type: "none" } });
});
// YES / NO branches from systemic
s.addText("YES → DMARDs + Biologics\nहो → रोगप्रतिकारक औषधे", {
x: 0.4, y: 3.38, w: 3.7, h: 0.6,
fontSize: 11, color: C.white, fontFace: "Calibri", align: "center", valign: "middle",
fill: { color: C.red }
});
s.addShape(pres.shapes.RECTANGLE, {
x: 0.4, y: 3.38, w: 3.7, h: 0.6, fill: { color: C.red }, line: { type: "none" }
});
s.addText("YES → DMARDs + Biologics\nहो → रोगप्रतिकारक औषधे", {
x: 0.5, y: 3.38, w: 3.5, h: 0.6,
fontSize: 11, color: C.white, fontFace: "Calibri", align: "center", valign: "middle"
});
// Conservative box
s.addShape(pres.shapes.RECTANGLE, {
x: 4.3, y: 3.5, w: 4.7, h: 0.65, fill: { color: C.green }, line: { type: "none" }
});
s.addText("Conservative (3-6 months)\nपुराणमतवादी उपचार ३-६ महिने", {
x: 4.4, y: 3.5, w: 4.5, h: 0.65,
fontSize: 11.5, bold: true, color: C.white, fontFace: "Calibri", align: "center", valign: "middle"
});
s.addText("Heel lift • NSAIDs • Eccentric exercise • Night splint • ESWT | टाच उशी • दाहविरोधी • व्यायाम • रात्री स्प्लिंट", {
x: 4.4, y: 4.22, w: 4.5, h: 0.35,
fontSize: 10, italic: true, color: C.teal, fontFace: "Calibri", align: "center"
});
// Failed conservative
s.addShape(pres.shapes.RECTANGLE, {
x: 4.3, y: 4.65, w: 4.7, h: 0.55, fill: { color: C.mgray }, line: { type: "none" }
});
s.addText("Failed Conservative? → MRI\nअपयश? → MRI करा", {
x: 4.4, y: 4.65, w: 4.5, h: 0.55,
fontSize: 11.5, bold: true, color: C.white, fontFace: "Calibri", align: "center", valign: "middle"
});
// Two surgical branches
s.addShape(pres.shapes.RECTANGLE, {
x: 0.4, y: 5.4, w: 5.8, h: 1.6, fill: { color: C.teal }, line: { type: "none" }
});
s.addText("<50% Tendinosis\n५०%पेक्षा कमी टेंडिनोसिस\n\nEndoscopic Calcaneoplasty\nor Zadek Osteotomy\n(दुर्बीण शस्त्रक्रिया / झाडेक ऑस्टिओटॉमी)", {
x: 0.5, y: 5.42, w: 5.6, h: 1.55,
fontSize: 12, bold: true, color: C.white, fontFace: "Calibri", align: "center", valign: "middle"
});
s.addShape(pres.shapes.RECTANGLE, {
x: 7.1, y: 5.4, w: 5.8, h: 1.6, fill: { color: C.red }, line: { type: "none" }
});
s.addText(">50% Tendinosis\n५०%पेक्षा जास्त टेंडिनोसिस\n\nDebridement + Exostectomy\n+ FHL Tendon Transfer\n(कंडरा दुरुस्ती + FHL बदली)", {
x: 7.2, y: 5.42, w: 5.6, h: 1.55,
fontSize: 12, bold: true, color: C.white, fontFace: "Calibri", align: "center", valign: "middle"
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 15 — QUICK REFERENCE SUMMARY
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addLightBg(s);
slideTitle(s, "Quick Reference Summary", "जलद संदर्भ सारांश");
const rows = [
["Topic", "Key Fact", "Marathi Note"],
["Bursa Location", "Deep to Achilles, between tendon & posterosuperior calcaneus", "अकिलीस कंडराच्या खाली"],
["Haglund Deformity", "Posterosuperior calcaneal exostosis (anterior to tendon)", "पोस्टेरोसुपेरियर हाडाची वाढ"],
["Key Exam Sign", "Mediolateral squeeze → fluid fluctuation", "मध्य-पार्श्व पिळणे चाचणी"],
["First Imaging", "Standing lateral heel X-ray", "उभे राहून पार्श्व टाच क्ष-किरण"],
["AVOID", "Corticosteroid injection near Achilles", "अकिलीसजवळ इंजेक्शन टाळा"],
["ESWT", "Chronic cases >6 weeks", "जुनाट रुग्णांसाठी शॉक वेव्ह"],
["Surgery threshold", "After 3-6 months failed conservative", "३-६ महिने अपयशानंतर"],
["Preferred Surgery", "Endoscopic calcaneoplasty (90.7 AOFAS, 4.1% complications)", "दुर्बीण शस्त्रक्रिया — प्रथम पसंती"],
[">50% Tendinosis", "Debridement + FHL transfer", "FHL बदली आवश्यक"],
["Zadek Osteotomy", "<50% tendinosis, high calcaneal pitch", "कमी टेंडिनोसिससाठी"],
["Fluoroquinolones", "Stop immediately if tendinopathy develops", "फ्लुरोक्विनोलोन त्वरित बंद करा"],
["Systemic Causes", "SpA, RA, Gout, CPPD, Ochronosis", "प्रणालीगत कारणे"],
];
const cw = [2.4, 5.5, 4.4];
const cx = [0.4, 2.85, 8.4];
const rh = 0.49;
rows.forEach((row, ri) => {
row.forEach((cell, ci) => {
const isHeader = ri === 0;
s.addShape(pres.shapes.RECTANGLE, {
x: cx[ci], y: 1.1 + ri * rh, w: cw[ci], h: rh,
fill: { color: isHeader ? C.navy : ri % 2 === 0 ? C.white : "EDF3F8" },
line: { color: C.lgray, width: 0.5 }
});
s.addText(cell, {
x: cx[ci] + 0.07, y: 1.13 + ri * rh, w: cw[ci] - 0.14, h: rh - 0.08,
fontSize: isHeader ? 11 : 10.5, bold: isHeader || ci === 0,
color: isHeader ? C.white : ci === 0 ? C.navy : C.mgray,
fontFace: "Calibri", valign: "middle"
});
});
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 16 — REFERENCES & THANK YOU
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
addDarkBg(s, C.navy);
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.55, h: 7.5, fill: { color: C.gold }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 5.6, w: 13.3, h: 1.9, fill: { color: C.teal }, line: { type: "none" } });
s.addText("References & Sources", {
x: 0.75, y: 0.25, w: 12.1, h: 0.55,
fontSize: 26, bold: true, color: C.white, fontFace: "Calibri"
});
s.addText("संदर्भ व स्रोत", {
x: 0.75, y: 0.78, w: 12.1, h: 0.38,
fontSize: 15, italic: true, color: C.gold, fontFace: "Calibri"
});
const refs = [
"1. Campbell's Operative Orthopaedics 15th Ed 2026 — Chapters 55 (Tendoscopy) & 88 (Insertional Achilles Tendinopathy)",
"2. Miller's Review of Orthopaedics 9th Edition — Chapter 6 (Foot & Ankle)",
"3. Goldman-Cecil Medicine (International Ed) — Chapter 40 (Disorders of the Ankle and Foot)",
"4. Grainger & Allison's Diagnostic Radiology — Musculoskeletal Imaging (Tendons, p.1000)",
"5. Roberts & Hedges' Clinical Procedures in Emergency Medicine — Chapter 51 (Heel Pain)",
"6. Alessio-Mazzola M et al. Endoscopic calcaneoplasty for Haglund's deformity. KSSTA 2021 — PMID: 33216187",
"7. Yuen WLP et al. Surgical Treatment of Haglund's Deformity: Systematic Review. Cureus 2022 — PMID: 36060327",
"8. Poutoglidou F et al. Zadek calcaneal osteotomy in insertional Achilles tendinopathy: Meta-analysis. Foot Ankle Surg 2023 — PMID: 37088671",
];
s.addText(refs.join("\n\n"), {
x: 0.75, y: 1.3, w: 12.2, h: 4.1,
fontSize: 10.5, color: C.lgray, fontFace: "Calibri", valign: "top"
});
s.addText("रेट्रोकॅल्केनियल बर्सायटिस — शरीररचनेपासून उपचारापर्यंत", {
x: 0.75, y: 5.72, w: 12.1, h: 0.45,
fontSize: 16, bold: true, color: C.white, fontFace: "Calibri", align: "center"
});
s.addText("Retrocalcaneal Bursitis — From Anatomy to Management | Orris Medical Reference 2026", {
x: 0.75, y: 6.18, w: 12.1, h: 0.35,
fontSize: 11, color: C.white, fontFace: "Calibri", align: "center"
});
}
// ══════════════════════════════════════════════════════════════════════════════
// WRITE FILE
// ══════════════════════════════════════════════════════════════════════════════
pres.writeFile({ fileName: "/home/daytona/workspace/retrocalcaneal-ppt/Retrocalcaneal_Bursitis_Complete.pptx" })
.then(() => console.log("SUCCESS: PPTX written."))
.catch(e => { console.error("ERROR:", e); process.exit(1); });
cd /home/daytona/workspace/retrocalcaneal-ppt && node make_ppt.js 2>&1
cd /home/daytona/workspace/retrocalcaneal-ppt && \ node /home/daytona/skills/shared/scripts/fetch_images.js \ "https://cdn.orris.care/cdss_images/2552b51a06c8a672790c07de779e7740ecda895a9121397a5dbe9030ffd1be7b.png" \ "https://cdn.orris.care/cdss_images/9b682c75f07ccfac7ba9b8d23ff7c9904f583b6b7c2192404d29d8fc94b2e094.png" \ "https://cdn.orris.care/cdss_images/719c92d190cc775d327fad8c132f988df02c80348f8743f56d24d142ed9b3d16.png" \ "https://cdn.orris.care/cdss_images/c77cd37ed2dea1c94a909acb623717a5af67bc5cdfce3b60828ec6eef9b15dd8.png" \ > /home/daytona/workspace/retrocalcaneal-ppt/images_b64.json && echo "Done, size=$(wc -c < images_b64.json)"
~/retrocalcaneal-ppt/make_ppt.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/retrocalcaneal-ppt/make_ppt.js'
cd /home/daytona/workspace/retrocalcaneal-ppt && node make_ppt.js 2>&1
ls -lh /home/daytona/workspace/retrocalcaneal-ppt/Retrocalcaneal_Bursitis_Complete.pptx
Retrocalcaneal Bursitis Complete
Presentation · PPTX
| Slide | Content |
|---|---|
| 1 | Title slide - Bilingual (English + मराठी), dark navy theme |
| 2 | Table of Contents - 11 topics with Marathi translations |
| 3 | Section divider — Anatomy |
| 4 | Anatomy - Bursal architecture, entheseal organ, two bursae comparison, systemic associations |
| 5 | Section divider — Pathophysiology |
| 6 | Pathophysiology + Haglund X-ray - Cascade of events diagram, lateral heel X-ray image embedded |
| 7 | Section divider — Clinical Presentation |
| 8 | Clinical Presentation - Symptoms, signs, Haglund triad, fluoroquinolone warning |
| 9 | Section divider — Imaging |
| 10 | X-ray + Radiological Measurements - Fowler-Philip angle, PPL, calcaneal pitch, X-ray image |
| 11 | MRI & Ultrasound - MRI Haglund syndrome triad image + US Achilles image, indication comparison boxes |
| 12 | Differential Diagnosis Table - 8 conditions with distinguishing features |
| 13 | Section divider — Non-operative Management |
| 14 | Non-operative Management - 6 category boxes (mechanical, pharmacological, PT, ESWT, immobilisation, AVOID corticosteroid in red) |
| 15 | Physical Therapy - 3 Phases - Phase 1/2/3 columns with Marathi labels |
| 16 | Section divider — Operative |
| 17 | Operative Options + Intraop X-ray - All 4 surgical procedures, MRI decision criterion |
| 18 | Endoscopic vs Open Evidence Table - Full data from 2021 systematic review (1,260 ankles) |
| 19 | Special Populations - Athletes, SpA/RA, Children (Sever's), Gout, Fluoroquinolone warning banner |
| 20 | Management Algorithm - Visual flowchart from presentation to surgery |
| 21 | Quick Reference Summary Table - 13 key topics at a glance |
| 22 | References + Thank You - All 8 sources cited with PMIDs |