Fibrous dysplasia of maxilla, mandible
Reading File
Finding Sources
Finding Sources
Searching PubMed
"fibrous dysplasia" AND "jaw" AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
I now have all the material needed for a thorough, well-illustrated answer. Let me compile the complete response.
Fibrous Dysplasia of the Maxilla and Mandible
Definition and Pathogenesis
Fibrous dysplasia (FD) is a benign, chronic, slowly progressive bone disorder in which normal cancellous bone is replaced by abnormal fibrous tissue and poorly calcified woven bone trabeculae. It is not a true neoplasm but a hamartomatous lesion arising from a mutation in the GNAS1 gene (chromosome 20q13), which codes for the alpha subunit of the stimulatory G-protein. This activating mutation leads to elevated cyclic AMP levels, driving abnormal proliferation of immature mesenchymal osteoblastic precursor cells. The result is failure of normal bone maturation - medullary cavity fills with fibrous tissue containing disorganized woven bone spicules.
- Cummings Otolaryngology, p. 2917 | Scott-Brown's ORL, p. 1148
Classification
| Type | Frequency | Features |
|---|---|---|
| Monostotic | ~75% | Single bone; craniofacial bones, ribs, proximal femur most common |
| Polyostotic | ~20% | Multiple bones; craniofacial region + femur most often |
| McCune-Albright Syndrome (MAS) | ~5% | Polyostotic FD + café-au-lait spots + endocrinopathies |
| Craniofacial FD | Subset | Multiple craniofacial bones involved; still classified as monostotic |
| Juvenile aggressive | Rare | Rapidly growing, markedly deforming lesion of the maxilla; destroys tooth buds; refractory to treatment |
The maxilla is the most commonly involved craniofacial bone in the polyostotic form. Multiple craniofacial localizations together are classified under "craniofacial fibrous dysplasia" and should still be considered monostotic. The mandibular condyles are characteristically spared in Cherubism (a hereditary variant limited to the mandible and maxilla).
- KJ Lee's Essential Otolaryngology, p. 1232 | Harrison's Principles, p. 3361
Clinical Features
Onset and Demographics:
- Most commonly diagnosed in the first two decades of life
- Equal sex frequency overall; MAS with precocious puberty is 10:1 female predominance
- Monostotic form may become quiescent at puberty; polyostotic form can continue progressing
- Lesions may reactivate during pregnancy or with estrogen therapy
Local symptoms (maxilla/mandible):
- Diffuse, painless bony swelling with facial deformity - the hallmark presentation
- Does not cross the midline
- Facial asymmetry and malocclusion
- Dental displacement; involves and incorporates the lamina dura and cortical bone
- Nasal obstruction and sinusitis (maxillary sinus encroachment)
- Orbital displacement causing proptosis or diplopia
- Optic nerve compression from orbital roof or sphenoid involvement - a serious complication
- In advanced cases: pain, pathological fracture, cranial nerve palsies
- Leontiasis ossea (lion-face deformity) in severe craniofacial involvement
Systemic features (MAS):
- Café-au-lait spots with rough "coast of Maine" borders (vs. smooth "coast of California" borders in neurofibromatosis)
- Precocious puberty (most common endocrinopathy)
- Less common: thyrotoxicosis, Cushing's syndrome, acromegaly, hyperparathyroidism
Radiological Findings
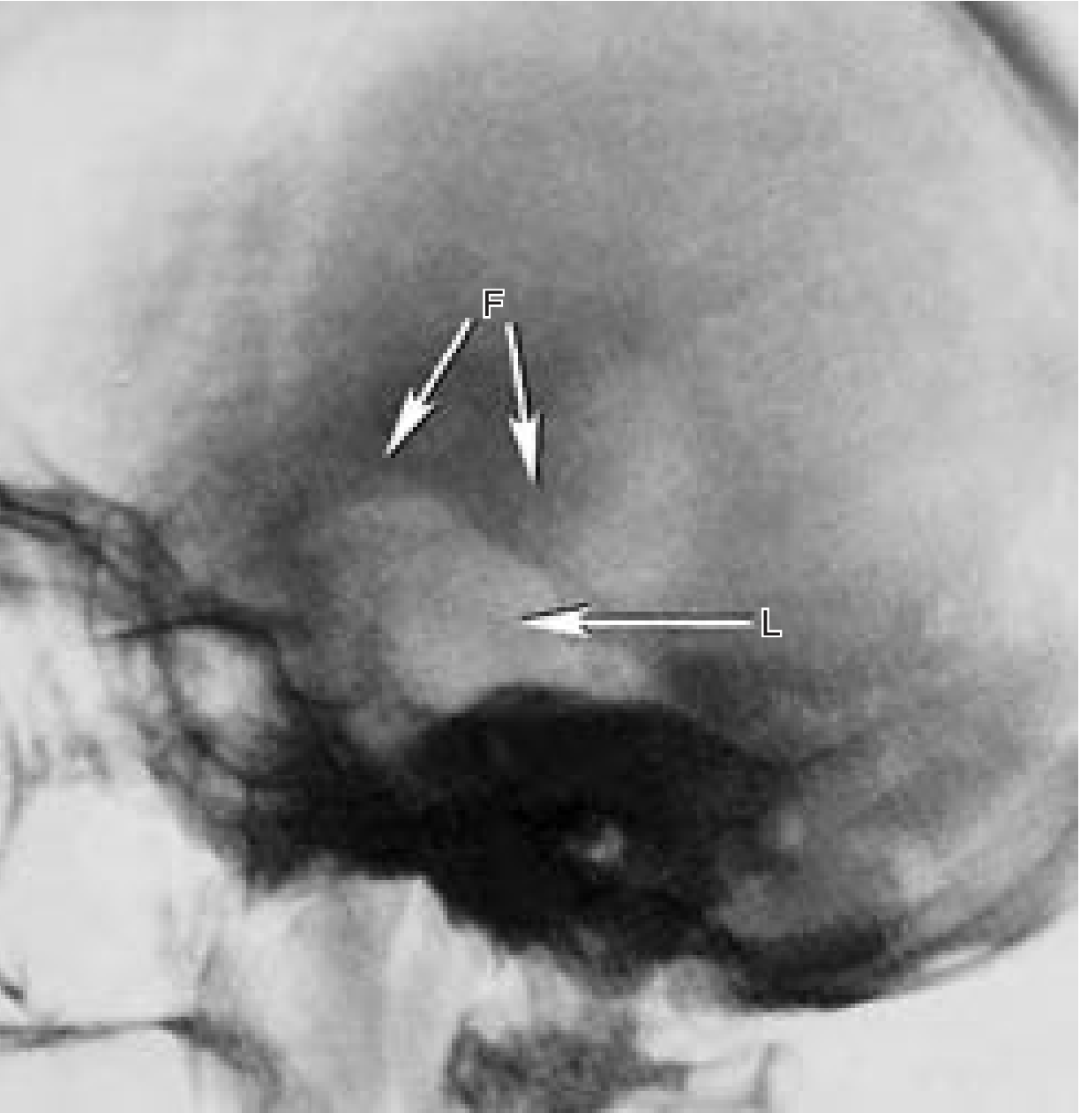
Plain radiograph / OPG:
- Classic: ground-glass appearance with fusiform, tapered expansion and diffuse margins
- May also appear as: multilocular radiolucency, radiolucent/lytic, or irregularly mottled (mixed opaque and lucent)
- Involves and incorporates the lamina dura and cortical bone (unlike ossifying fibroma)
- The lesion blends with surrounding bone without a discrete capsule
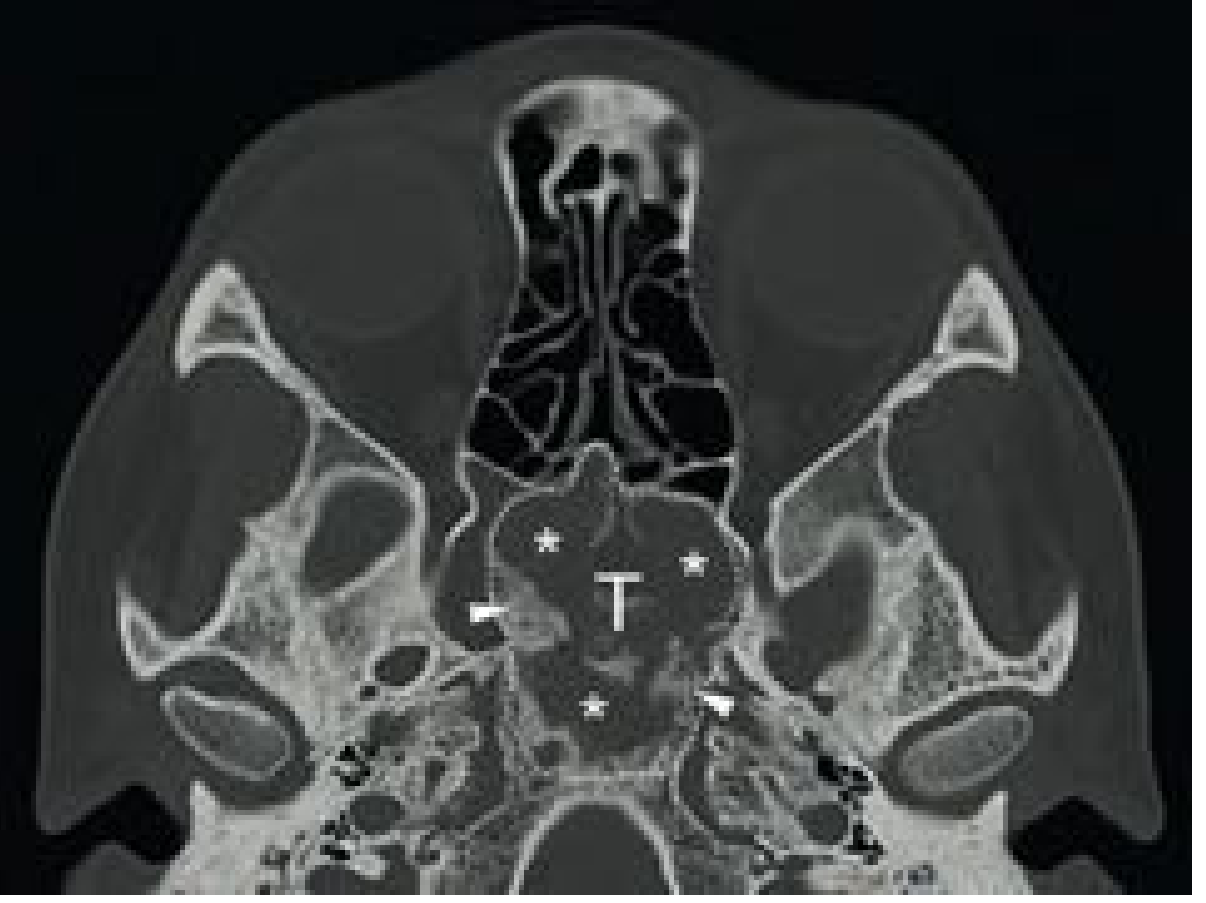
CT scan (modality of choice):
- Appearance depends on degree of mineralization:
- Early/high fibrous content: radiolucent/lytic appearance
- As mineralization increases: ground-glass (most characteristic)
- Advanced: sclerotic/dense
- Expansile lesion with mixed density; no sharp peripheral cortical rim (unlike ossifying fibroma)
- Involvement of the maxillary sinus walls, orbital floor, and skull base can be assessed
MRI:
- Variable T2 signal (reflects varying degrees of mineralization)
- T1: commonly hypointense
- Non-homogeneous enhancement with gadolinium
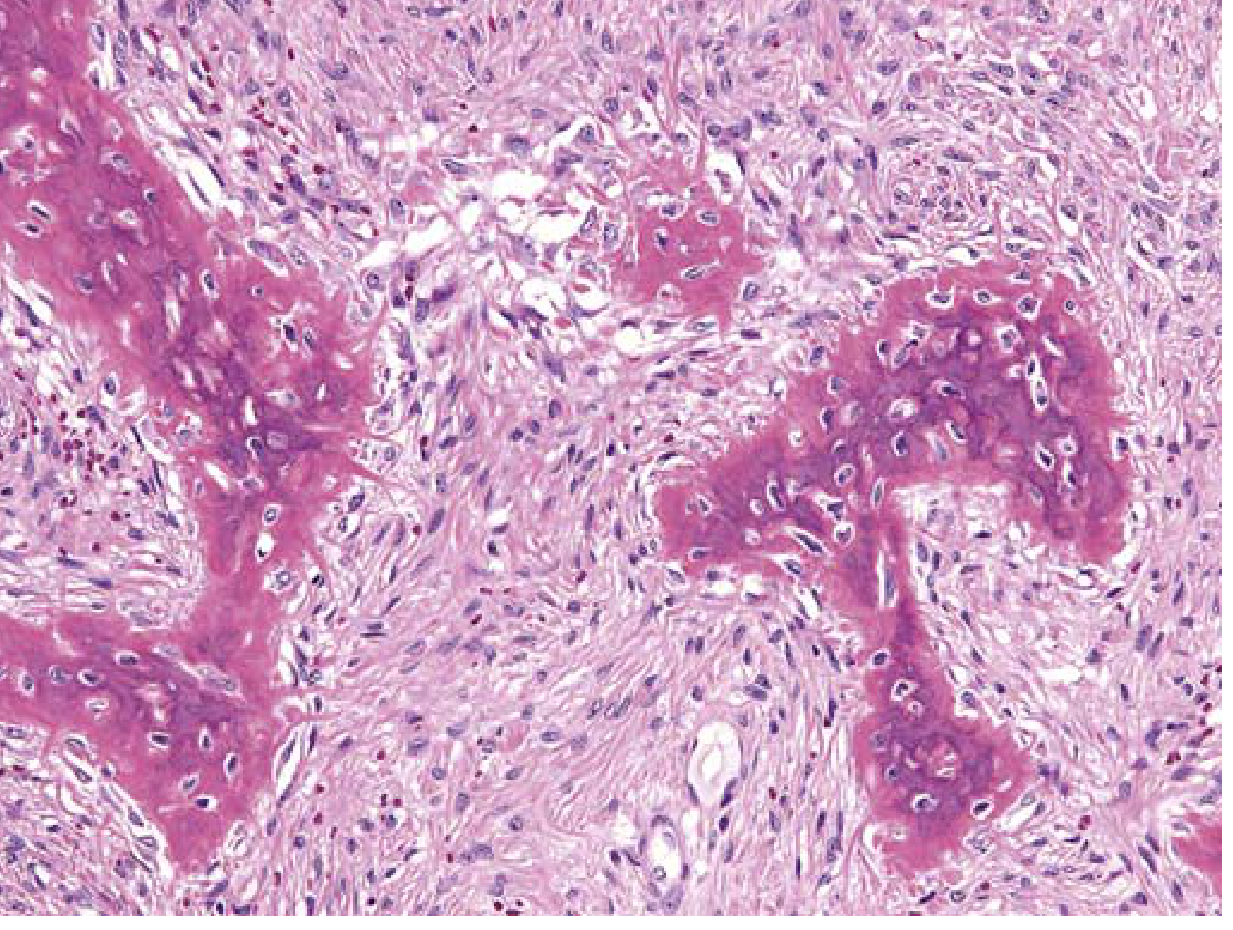
Histopathology
Normal cancellous bone is replaced by a fibrous stroma arranged in a whorled pattern, containing irregularly arranged spicules of woven bone (the "Chinese letters" pattern). The woven bone spicules lack osteoblastic rimming - a key distinguishing feature from ossifying fibroma and other fibro-osseous lesions.
Key features:
- Stroma: cellular, spindle-cell fibrous tissue
- Trabeculae: curvilinear, disconnected woven bone (like "Chinese letters" or alphabet soup)
- No osteoblastic rimming of bone trabeculae (important!)
- No lamellar bone
- Diagnosis cannot be made by microscopy alone - requires correlation with clinical and radiographic findings
Differential Diagnosis
| Feature | Fibrous Dysplasia | Ossifying Fibroma | Cherubism |
|---|---|---|---|
| Age | 1st-2nd decade | Adults (mandible most common) | Children |
| Borders | Diffuse, blend with bone | Well-demarcated, capsule | Bilateral |
| CT rim | No peripheral rim | Eggshell-like dense rim | - |
| Bone trabeculae | Curvilinear, no osteoblast rimming | Lamellar bone + osteoblast rimming | - |
| Root effects | Incorporates lamina dura | Diverges tooth roots | - |
| Treatment | Conservative; recontouring | Wide resection (high recurrence) | Often resolves at puberty |
| Heredity | No (sporadic GNAS1 mutation) | No | Yes (autosomal dominant) |
| Midline crossing | No | Yes (can) | Bilateral, symmetric |
Laboratory Findings
- Serum alkaline phosphatase (ALP) elevated in ~30% of polyostotic cases
- Serum calcium, phosphorus, PTH, 25-OH vitamin D: usually normal
- Extensive polyostotic lesions: may cause hypophosphatemia + hyperphosphaturia + osteomalacia (due to FGF23 overproduction by dysplastic tissue)
- Biochemical markers of bone turnover may be elevated
Treatment
Conservative (observation):
- Asymptomatic patients should be followed with periodic clinical and radiological examinations
- Monostotic FD can often be observed; lesions tend to stabilize after skeletal maturation
- Surgery should be postponed as long as possible in younger, asymptomatic patients
Medical:
- Bisphosphonates (IV): Reduce bone pain and may partially resolve radiographic lesions; reduce fracture risk
- Denosumab: Monthly or every 3 months; effective in reducing bone turnover markers; note - discontinuation can occasionally result in rebound hypercalcemia (per Harrison's 22nd ed., 2025)
- No role for radiotherapy - it is ineffective and increases risk of malignant transformation
Surgical indications:
- Visual impairment (optic nerve compression)
- Cosmetic/aesthetic deformity
- Sinus obstruction causing sinusitis
- Pathologic fracture risk or destruction of joint space
- Cranial nerve compression
Surgical approach:
- Endoscopic sinus surgery for paranasal sinus lesions - improves drainage, relieves sinusitis; ideally with computer-assisted navigation
- Local controlled resection and bone recontouring (not radical excision) for cosmetic deformity
- In contrast to ossifying fibroma, wide radical resection is NOT required for FD
Complications and Prognosis
- Sarcomatous transformation: Rare; estimated at 0.4-0.5% (osteosarcoma most common)
- Any rapidly growing, painful lesion should raise suspicion
- Risk is increased by radiation (never irradiate FD)
- Lesions typically stabilize after skeletal maturity
- Polyostotic form can continue progressing into adulthood
- Renal phosphate wasting with rickets/osteomalacia in widespread disease
Key Distinguishing Points for the Maxilla vs. Mandible
- Maxilla is the most commonly involved jaw bone in craniofacial FD, particularly in polyostotic disease
- Maxillary FD can obliterate the maxillary sinus, encroach on the orbit, and involve the pterygoid plates
- Mandibular FD is less common; when the mandible is the sole site in children, consider cherubism (which bilaterally involves mandible and maxilla but spares the condyles)
- The juvenile aggressive variant almost exclusively involves the maxilla - rapidly growing, destroys tooth buds, and is refractory to treatment
Sources: Cummings Otolaryngology Head and Neck Surgery | Scott-Brown's Otorhinolaryngology H&N Surgery Vol. 1 | KJ Lee's Essential Otolaryngology | Harrison's Principles of Internal Medicine 22E (2025)
Recent evidence note (2026): A systematic review (PMID 41955566, J Clin Endocrinol Metab, June 2026) from the ECTS Rare Bone Disease Action Group reviewed denosumab use in rare bone diseases including fibrous dysplasia. Its findings support denosumab as an option when bisphosphonates are insufficient, consistent with Harrison's 22E guidance above.
Fibrous dysplasia of maxilla, mandible
Reading File
Finding Sources
Finding Sources
Searching PubMed
"fibrous dysplasia" AND "craniofacial" AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
All key content and images are now in hand. Here is the comprehensive answer.
Fibrous Dysplasia of the Maxilla and Mandible
Definition and Pathogenesis
Fibrous dysplasia (FD) is a benign, slowly progressive developmental bone disorder in which normal cancellous bone is replaced by abnormal fibrous tissue and poorly calcified woven bone trabeculae. It is not a true neoplasm but rather a genetic developmental anomaly of the bone-forming mesenchyme, with a defect in osteoblastic differentiation and maturation.
Molecular basis: All forms of FD result from a somatic gain-of-function mutation in GNAS1 (also written GNASI), located on chromosome 20q13. This gene encodes the alpha subunit of the stimulatory G-protein (Gs-alpha). The activating mutation constitutively elevates cellular cAMP levels, which:
- Promotes cellular proliferation
- Disrupts osteoblast differentiation
- Prevents maturation of bone to lamellar structure
The phenotype depends on the timing of the mutation during embryogenesis and the proportion/location of mesenchymal cells harboring it. The result is a lesion composed of immature mesenchymal osteoblastic precursor cells unable to produce mature bone.
- Robbins & Kumar Basic Pathology, p. 789 | Scott-Brown's ORL Vol. 1, p. 1148
Classification
| Type | Frequency | Key Features |
|---|---|---|
| Monostotic | ~75% | Single bone affected; skull, ribs, proximal femur, tibia most common |
| Polyostotic | ~20% | Multiple bones; craniofacial region + femur most frequently involved |
| McCune-Albright Syndrome (MAS) | ~5% | Polyostotic FD + café-au-lait skin pigmentation + endocrinopathies |
| Mazabraud Syndrome | Rare | FD + soft tissue myxoma |
| Craniofacial FD | Subset | Multiple craniofacial bones; still classified as monostotic |
| Juvenile aggressive | Rare | Rapidly growing, markedly deforming lesion of maxilla; destroys tooth buds; refractory to treatment |
Ossifying fibroma and FD were historically grouped together due to histologic overlap, but Reed (1963) separated them. FD is a genetic developmental anomaly; ossifying fibroma is a true benign neoplasm. The key histologic difference is the absence of a capsule and lack of osteoblastic rimming in FD.
- Cummings Otolaryngology, p. 996
Clinical Features
Age / Sex:
- Presents in the first to second decade of life
- Equal sex frequency overall; MAS with precocious puberty is 10:1 female predominance
- Monostotic form often becomes quiescent at skeletal maturity (puberty); polyostotic can progress into adulthood
- Early-onset disease is generally more severe
- Lesions may reactivate during pregnancy or with estrogen therapy
Local jaw symptoms:
- Diffuse, painless bony swelling causing facial deformity - the cardinal presentation
- Does not cross the midline
- Facial asymmetry and malocclusion
- Loose dentition; incorporates and displaces the lamina dura
- Mass of the body of the mandible or alveolar ridge of maxilla
- Paresthesias, pain (if nerve involved)
- Maxillary: nasal obstruction, sinusitis, sinus drainage obstruction
- Maxillary/orbital: proptosis, diplopia, epiphora
- Optic nerve compression from orbital roof or sphenoid extension - a sight-threatening complication
- Headache, facial pressure
Systemic (MAS) features:
- Café-au-lait spots with rough "coast of Maine" borders (vs. smooth "coast of California" in neurofibromatosis)
- Isosexual pseudoprecocious puberty (most common endocrinopathy - girls >> boys)
- Less common: thyrotoxicosis, Cushing's syndrome, acromegaly, hyperparathyroidism, hyperprolactinemia
- Leontiasis ossea (lion-face appearance) in severe craniofacial involvement
- Skull base foraminal narrowing causing hearing loss, visual loss, or other cranial nerve deficits
Radiological Features
Plain radiograph / OPG:
- Classic: ground-glass appearance with fusiform, tapered expansion and diffuse margins (no discrete capsule)
- Also: multilocular radiolucency, lytic, or irregularly mottled (mixed opaque and lucent)
- Involves and incorporates the lamina dura and cortical bone (key point - does not displace or thin the cortex as a separate rim)
- Lesion blends imperceptibly with surrounding bone
CT scan (modality of choice for extent and surgical planning):
- Appearance tracks degree of mineralization:
- Early/high fibrous content → radiolucent/lytic (mimics simple bone cyst)
- Intermediate mineralization → ground-glass (most characteristic and diagnostic)
- Advanced mineralization → cotton-wool / sclerotic
- Expansile lesion; no sharp peripheral eggshell cortical rim (ossifying fibroma has this)
- Useful for: sinus obliteration, orbital involvement, skull base foraminal compromise, optic canal narrowing
MRI:
- T1: intermediate signal (hypointense in many cases)
- T2: hypointense (helpful to distinguish from meningioma and bone cysts, which are T2 bright)
- Non-homogeneous gadolinium enhancement
- Useful to evaluate soft tissue component and nerve compression
Histopathology
The hallmark is replacement of normal cancellous bone by a moderately cellular fibroblastic (spindle cell) stroma containing curvilinear trabeculae of woven bone without osteoblastic rimming - the so-called "Chinese letters" or "alphabet soup" pattern.
Key features:
- Fibrous stroma arranged in a whorled pattern
- Woven bone spicules are irregular, disconnected, curvilinear
- No rim of osteoblasts around bone trabeculae (critical distinction from ossifying fibroma)
- No lamellar bone maturation
- Cystic degeneration, hemorrhage, and foamy macrophages may be present
- No capsule (contrast: ossifying fibroma is capsulated)
- Periosteal reaction: usually absent
"Diagnosis is often impossible by microscopy alone and requires clinical and radiographic information." - KJ Lee's Essential Otolaryngology
Laboratory Findings
- Serum alkaline phosphatase (ALP) elevated in ~30% of polyostotic FD cases
- Serum calcium, phosphorus, PTH, 25-OH vitamin D: usually normal
- Extensive polyostotic lesions: hypophosphatemia + hyperphosphaturia (due to FGF-23 overproduction by dysplastic tissue) causing rickets or osteomalacia
- Biochemical markers of bone turnover may be elevated
Differential Diagnosis
| Feature | Fibrous Dysplasia | Ossifying Fibroma | Cherubism |
|---|---|---|---|
| Age | 1st-2nd decade | Adults | Children |
| Genetics | Sporadic GNAS1 | Sporadic | Autosomal dominant |
| Borders | Diffuse, blend with bone | Well-demarcated, capsulated | Bilateral symmetric |
| CT rim | No peripheral eggshell rim | Eggshell-like dense rim | - |
| Histology | Woven bone, no osteoblast rimming | Lamellar bone + osteoblast rimming | - |
| Root effect | Incorporates lamina dura | Diverges tooth roots | - |
| Midline crossing | No | Can cross | Bilateral |
| Condyles | May involve | - | Characteristically spared |
| Treatment | Conservative, recontouring | Wide resection (high recurrence) | Often resolves at puberty |
Treatment
Conservative (observation):
- Asymptomatic monostotic FD can be observed with periodic clinical and radiological follow-up
- Lesions tend to stabilize after skeletal maturation; surgery should be deferred as long as possible in asymptomatic children
Medical:
- IV bisphosphonates - reduce bone pain, reduce fracture incidence, may partially resolve radiographic lesions
- Denosumab (monthly or every 3 months) - reduces bone turnover markers; note that discontinuation can trigger rebound hypercalcemia
Surgical indications:
- Visual impairment / optic nerve compression
- Cosmetic/aesthetic deformity
- Sinus obstruction causing chronic sinusitis
- Pathologic fracture risk or joint destruction
- Cranial nerve compression (hearing loss, etc.)
Surgical approach:
- Endoscopic sinus surgery for paranasal sinus involvement - improves drainage; computer-assisted navigation is preferred
- Local controlled resection + bone recontouring for cosmetic deformity - not radical resection (unlike ossifying fibroma)
- Wide radical excision is NOT indicated; FD does not have sharp margins and recontouring is the goal
No role for radiotherapy - it is ineffective and significantly increases the risk of malignant transformation. Never irradiate FD.
Complications and Prognosis
- Sarcomatous transformation: ~0.4-0.5%; osteosarcoma most common
- Risk significantly increased by prior radiation therapy
- Suspect in any rapidly growing or painful lesion
- Monostotic FD: generally stabilizes at skeletal maturity; favorable prognosis
- Polyostotic FD: may progress into adulthood; more complications
- Renal phosphate wasting (FGF-23 mediated) in widespread disease
Maxilla vs. Mandible: Specific Points
Maxilla:
- Most commonly involved jaw bone in craniofacial FD, especially in polyostotic disease
- Can obliterate the maxillary sinus entirely, erode the orbital floor, and extend to the pterygoid plates and skull base
- The juvenile aggressive variant almost exclusively affects the maxilla - rapidly growing, destroys tooth buds, and is refractory to treatment
- Orbital/optic nerve complications are more likely with maxillary involvement
Mandible:
- Less commonly involved than maxilla in FD
- Presents as painless swelling of the body of the mandible
- When bilateral mandibular FD occurs in children, always consider Cherubism (inheritable, autosomal dominant, spares condyles - unlike conventional FD)
- Monostotic mandibular FD: relatively better prognosis; often stabilizes at puberty
Sources: Cummings Otolaryngology Head and Neck Surgery | Scott-Brown's Otorhinolaryngology H&N Surgery Vol. 1 | KJ Lee's Essential Otolaryngology | Robbins & Kumar Basic Pathology | Harrison's Principles of Internal Medicine 22E
Recent literature (2025): A systematic review on craniofacial FD (Tuompo et al., Bone, Mar 2025; PMID 39681203) provides an updated synthesis of diagnosis and management of craniofacial FD - the most relevant recent evidence for this topic.
This is a shared conversation. Sign in to Orris to start your own chat.