Submandibular gland excision
Reading File
Finding Sources
Finding Sources
Searching PubMed
"submandibular gland" AND "excision" AND "complications"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
I have sufficient material for a complete answer. Here it is:
Submandibular Gland Excision
Anatomy Review (Surgical Relevance)
The submandibular gland has a larger superficial lobe and a smaller deep lobe connected around the posterior border of the mylohyoid muscle. The superficial lobe sits in the digastric triangle; the deep lobe lies on the hyoglossus muscle. Key anatomical relationships:
- Marginal mandibular branch of the facial nerve - runs in the superficial fascia, crosses over the facial vessels; injury causes drooping of the ipsilateral corner of the mouth
- Lingual nerve - lies on the hyoglossus muscle, crossing Wharton's duct laterally; at risk during duct ligation
- Hypoglossal nerve (CN XII) - lies deep to the lingual nerve on the hyoglossus; injury causes ipsilateral tongue deviation
- Facial artery - passes through or superficial to the gland, must be ligated twice (at entry and exit)
- Facial vein - superficial to the gland; used as a landmark for nerve protection
- Wharton's duct (submandibular duct) - ~5 cm long, emerges from the deep lobe, opens at the sublingual papilla in the floor of the mouth
- Submandibular ganglion - suspended from the lingual nerve on the hyoglossus; carries parasympathetic secretomotor fibres; must be divided to free the gland without injuring the lingual nerve
Indications
- Benign disease: chronic sialadenitis (most common), sialolithiasis not amenable to sialendoscopy, recurrent obstruction, ranula, benign tumors (pleomorphic adenoma, Warthin's)
- Malignant tumors: adenoid cystic carcinoma, mucoepidermoid carcinoma, etc. - requires excision of gland + Level Ib lymph node clearance ± neck dissection
Pre-operative Assessment
- Fine needle aspiration cytology (FNAC) or core biopsy for suspected tumors
- Ultrasound +/- CT/MRI to assess gland, duct stones, and locoregional spread in malignancy
- Rule out reactive lymphadenopathy (often mimics submandibular gland pathology)
- For malignancy: assess nerve involvement (hypoglossal > trigeminal > marginal mandibular)
Anaesthesia
General anaesthesia is standard. Nerve monitoring is recommended (oral commissure should be included in the operative field).
Surgical Technique (Transcervical Approach)
This is the standard and most widely used approach.
1. Incision
A curvilinear incision is placed in a natural skin crease, at least 2-3 finger-breadths (3-4 cm) below the inferior border of the mandible, directly over the gland. This keeps the incision well below the marginal mandibular nerve and provides a cosmetically acceptable scar along Langer's lines.
2. Flap Elevation
- Incise through skin, subcutaneous fat, and platysma
- Elevate a subplatysmal flap superiorly to the level of the mandible attachment of the platysma - this is an avascular plane; veins should remain in the investing fascia
- Retract with skin hooks
3. Marginal Mandibular Nerve Identification and Protection
- Identify the nerve in the fascia overlying the facial vessels at the midpoint of the mandibular body; it exits the parotid, curves anteriorly and caudally, runs over the posterior facial vein, then curves cranially toward the oral commissure
- Hayes-Martin maneuver: doubly ligate the anterior facial vein below the nerve and retract the superior ligature (and the fascia it holds) upward - this physically displaces the nerve superiorly and out of the operative field
- The proximal stump of the facial vein can be retracted superiorly to keep the nerve away from active dissection
4. Gland Mobilization
- Ligate the submental vessels (branches to mylohyoid)
- Ligate and divide the facial artery superiorly, freeing the upper attachment of the gland
- Retract the gland downward and outward to expose the mylohyoid muscle and its lateral free edge
5. Deep Lobe Exposure
- Retract the free (posterior) edge of the mylohyoid anteriorly while maintaining gentle posterior traction on the gland
- This unmasks the deep portion of the gland, Wharton's duct, the submandibular ganglion, and the lingual and hypoglossal nerves - all lying superficial to the hyoglossus muscle
- Retract the gland superiorly and posteriorly to expose the hypoglossal nerve above the ranine veins
6. Nerve and Duct Management
- Divide the submandibular ganglion (the nerve branches from the lingual nerve to the ganglion) - this releases the lingual nerve from the gland
- Identify and protect the hypoglossal nerve deep to the anterior belly of the digastric
- Doubly ligate and divide Wharton's duct as close to the floor of the mouth as possible (reduces risk of retained debris or stones and subsequent infection)
7. Final Ligation and Removal
- Divide the facial artery a second time (at its inferior entry to the gland near the common tendon of the digastric)
- Separate the specimen from the digastric muscle
- The gland is removed en bloc
8. Closure
- Achieve hemostasis; consider a drain if a large dead space exists
- Close platysma and skin in layers
For Malignancy (Modified Technique)
- Excise the gland en continuity with Level Ib lymph node-bearing fibrofatty tissue (perivascular lymph nodes)
- The fatty tissue between the inferior aspect of the mandible and the gland is kept together with the specimen
- For low-grade tumors <4 cm without extraparenchymal spread: gland excision + Level Ib clearance is sufficient
- For high-grade or more advanced disease: supra-omohyoid neck dissection (Levels I-III) or modified radical neck dissection
- The hypoglossal nerve is preserved unless grossly involved by tumor
Alternative Approaches
Transoral Approach
Gaining popularity, particularly where sialendoscopy has already been attempted or in pediatric cases.
- Wharton's duct is cannulated; an incision encircles the duct orifice and extends along the floor of the mouth
- Sublingual gland is removed first by blunt dissection, exposing the duct-lingual nerve relationship
- The duct is tunneled under the lingual nerve and followed to the hilum
- Digital pressure from below the submandibular triangle delivers the gland into the field
- Endoscopic assistance improves visualization
- Must be prepared to convert to open if facial artery bleeding occurs
- Advantage: no external scar, no marginal mandibular nerve risk from external approach
Endoscopic / Robotic-Assisted
Emerging techniques via retroauricular or submental approaches; can reduce complication rates and improve cosmesis.
Complications
| Complication | Nerve / Structure | Consequence |
|---|---|---|
| Marginal mandibular nerve injury | CN VII (marginal branch) | Drooping of ipsilateral lower lip/oral commissure |
| Lingual nerve injury | CN V3 branch | Ipsilateral tongue numbness/dysgeusia |
| Hypoglossal nerve injury | CN XII | Ipsilateral tongue deviation, dysphagia |
| Hematoma | Facial vessels | Requires evacuation |
| Infection / Abscess | - | Wound infection, cellulitis |
| Scar / keloid | - | Cosmetic |
| Salivary fistula | Residual duct | Rare |
| Xerostomia | Loss of ~65% submandibular contribution | Usually subclinical |
The marginal mandibular nerve is the most commonly injured nerve. Rates of temporary palsy up to 10-20% and permanent palsy ~1-5% have been reported; meticulous identification and the Hayes-Martin retraction maneuver are the primary preventive measures.
Key Points Summary
- Incision: skin crease, 3-4 cm below mandible
- The Hayes-Martin maneuver (superior retraction of the facial vein ligature) is the core technique for protecting the marginal mandibular nerve
- Dividing the submandibular ganglion is what separates the lingual nerve from the gland
- Wharton's duct is ligated close to the floor of the mouth
- The hypoglossal nerve is deep and at risk only during the deepest part of the dissection
- For malignancy: include Level Ib en bloc; consider neck dissection based on grade and stage
Sources:
- Cummings Otolaryngology Head and Neck Surgery (Chapters 84 & 205)
- Bailey and Love's Short Practice of Surgery, 28th Ed. (Chapter 54)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Chapters 41 & 10)
Recent evidence note: A 2026 systematic review and meta-analysis (PMID 42001628) compared gland-preserving surgery vs. total gland excision for benign submandibular tumors - suggesting a possible role for partial gland-sparing approaches in selected benign lesions.
Submandibular gland anatomy
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I have comprehensive information from multiple authoritative sources. Here is the complete anatomy review:
Submandibular Gland Anatomy
Overview
The submandibular gland is the second largest major salivary gland, irregular in shape and roughly the size of a walnut. It weighs 7-16 g and is a mixed gland, predominantly serous (serous acini predominate, with some mucous acini capped by serous demilunes). It contributes approximately 60-70% of resting salivary volume.
Location - The Submandibular (Digastric) Triangle
The gland occupies the submandibular triangle, which is bounded by:
- Anteriorly: anterior belly of the digastric muscle
- Inferolaterally: posterior belly of the digastric + stylohyoid muscle
- Superiorly: inferior border of the body of the mandible
- Floor: mylohyoid muscle anteriorly, hyoglossus muscle posteriorly
The triangle also contains the facial artery and vein, marginal mandibular branch of the facial nerve, and Level Ib lymph nodes.
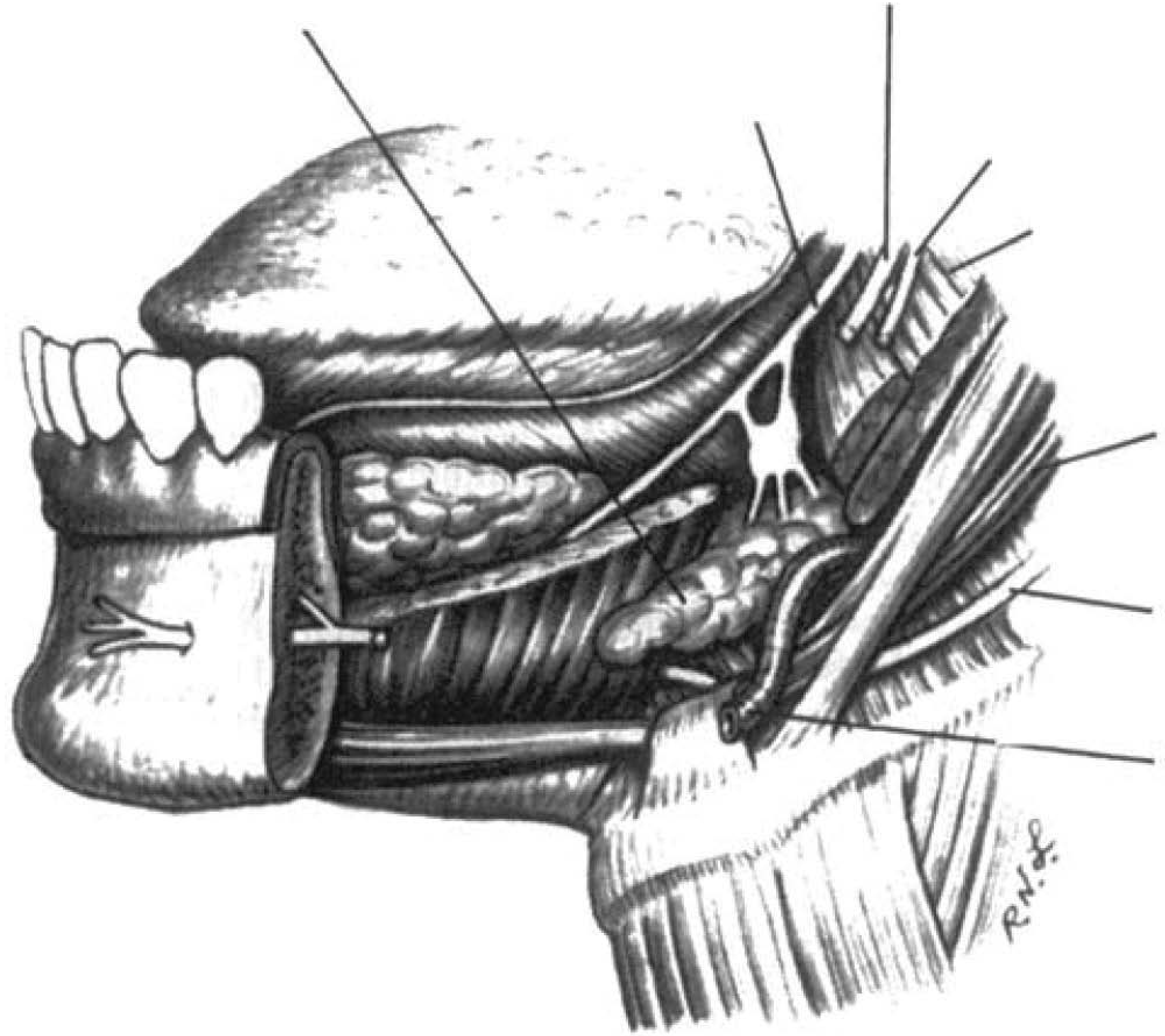
Submandibular gland anatomy: the gland wraps around the posterior border of mylohyoid, with its deep part lying between mylohyoid and hyoglossus, flanked by the lingual nerve above and hypoglossal nerve below.
Structure - Superficial and Deep Parts
The gland has two parts connected around the posterior free border of the mylohyoid muscle:
Superficial Part (larger)
- Lies in the digastric triangle
- Above, it extends medially to the body of the mandible (submandibular fossa)
- Below, it overlaps the intermediate tendon of the digastric and insertion of stylohyoid
- Covered by: skin, platysma, and the split layer of deep cervical fascia (derived from greater cornu of hyoid)
- The fascia blends with the periosteum of the mandible along the mylohyoid line medially and the lower mandibular border laterally
Deep Part (smaller)
- Lies between mylohyoid inferolaterally and hyoglossus and styloglossus medially
- Sits between the lingual nerve above and the hypoglossal nerve below
- Extends anteriorly to reach the posterior end of the sublingual gland
Surface Relations
| Surface | Relations |
|---|---|
| Lateral (outer) | Submandibular fossa of mandible, origin of medial pterygoid muscle |
| Inferior | Skin, platysma, deep cervical fascia; crossed by facial vein and cervical branch of facial nerve |
| Medial (deep) - anterior part | Mylohyoid muscle and its nerve + submental vessels |
| Medial (deep) - posterior part | Hyoglossus muscle, lingual nerve, submandibular ganglion, hypoglossal nerve, styloglossus, posterior belly of digastric |
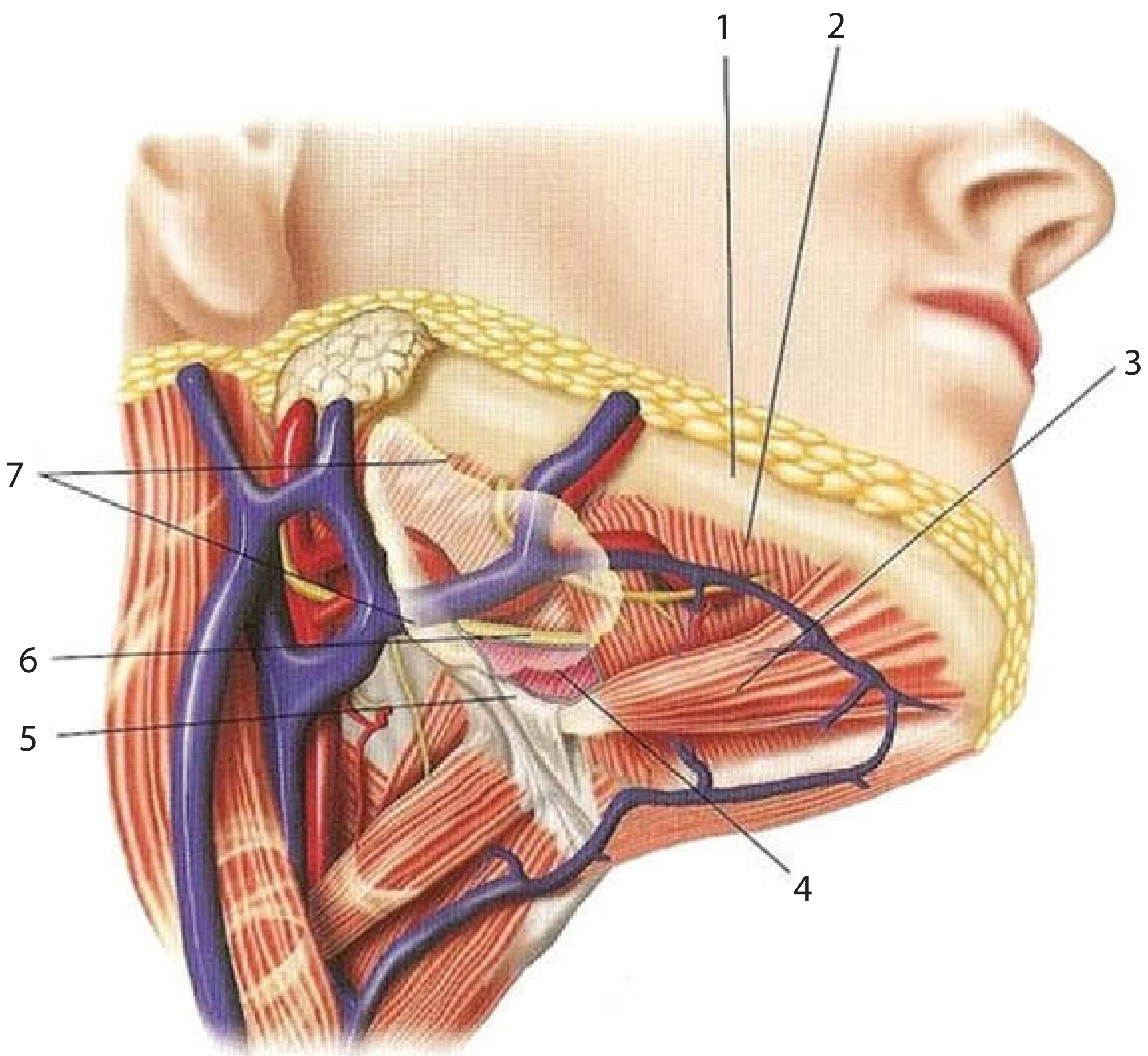
Cross-sectional anatomy of the submandibular gland region. Key: 1. Mandible, 2. Mylohyoid, 3. Anterior belly of digastric, 4. Submandibular gland, 5. Hyoid, 6. Hypoglossal nerve, 7. Facial artery
Wharton's Duct (Submandibular Duct)
- Length: ~5 cm
- Origin: formed by coalescence of ducts within the superficial part, emerges from the medial surface of the superficial lobe behind the posterior border of mylohyoid
- Course: passes through the deep part of the gland, then runs anteriorly along the floor of the mouth between:
- Laterally: sublingual gland
- Medially: genioglossus muscle
- Key crossing: on the hyoglossus muscle, the lingual nerve crosses the duct laterally (wraps around it in a double loop - crossing superior to it anteriorly, then inferior to it posteriorly)
- Opening: opens at the sublingual papilla (caruncle) at the side of the lingual frenulum on the floor of the mouth
- Narrowest point: at the ostium (mean ~0.5 mm); this is where stones most commonly obstruct
- The duct lies between the hypoglossal and lingual nerves as it courses forward on the hyoglossus
Blood Supply
- Arterial: submental branch of the facial artery (branch of the external carotid artery)
- The facial artery passes deep to the posterior belly of digastric and stylohyoid, then enters or deeply grooves the posterior aspect of the gland, loops through or superficially over it, and exits between the gland and the lower border of the mandible to reach the face
- Glandular branches are ligated during excision; the main facial artery trunk can be preserved (important as a recipient vessel for microvascular free flap anastomosis)
- Venous: corresponding facial vein, which is lateral (superficial) to the gland draining toward the anterior mandibular border
Nerve Supply
Parasympathetic (Secretomotor)
The pathway is the most clinically important:
- Superior salivatory nucleus (pons, nervus intermedius)
- → Facial nerve (CN VII) within temporal bone
- → Chorda tympani - branches off the vertical segment of the facial nerve, crosses the middle ear medial to the handle of the malleus, exits via the petrotympanic fissure, enters the infratemporal fossa
- → Joins the lingual nerve (V3 branch) in the infratemporal fossa
- → Preganglionic fibres travel with the lingual nerve to reach the submandibular ganglion
- → Synapse in the submandibular ganglion - postganglionic fibres then either:
- Re-enter the lingual nerve and travel to the gland with its terminal branches, OR
- Pass directly from the ganglion to the gland
The Submandibular Ganglion
- A small, fusiform parasympathetic ganglion
- Hangs from (suspended by) the lingual nerve on the upper surface of the hyoglossus muscle
- Secretomotor to both the submandibular and sublingual glands
- Surgically significant: dividing the ganglion fibres from the lingual nerve is what separates the lingual nerve from the gland during excision
Sympathetic
- From the superior cervical ganglion via the sympathetic plexus on the facial artery (and lingual artery)
- Sympathetic fibres pass through the submandibular ganglion without synapsing
- Distributed to blood vessels of the gland (vasoconstrictor)
Marginal Mandibular Branch of the Facial Nerve
- Not innervating the gland but runs in close proximity
- Lies in the superficial fascia, traversing over (lateral to) the facial vein
- Exits the parotid, curves anteriorly and caudally paralleling the mandible, passes over the posterior facial vein, then curves cranially toward the oral commissure
- Dissecting deep to the facial vein can be used to preserve or identify this nerve
Lymphatics
- Submandibular lymph nodes lie at the medial aspect and anterior end of the superficial part - some may be embedded within the gland itself
- These are Level Ib nodes
- Perivascular lymph nodes around the facial artery are frequently involved in submandibular gland cancer and must be removed with the gland
- Efferent lymphatics drain to the deep cervical chain, particularly the jugulo-omohyoid nodes
Key Nerves at Risk - Summary Table
| Nerve | Location Relative to Gland | Injury Consequence |
|---|---|---|
| Marginal mandibular (CN VII) | Superficial fascia, crossing over facial vein; superior to gland | Drooping lower lip / oral commissure |
| Lingual nerve (V3) | Medial surface of deep lobe, on hyoglossus; crosses Wharton's duct | Ipsilateral tongue numbness, loss of taste (anterior 2/3), dry mouth |
| Hypoglossal nerve (CN XII) | Deep to lingual nerve, below Wharton's duct on hyoglossus | Ipsilateral tongue deviation, dysarthria, dysphagia |
| Chorda tympani | Joins lingual nerve proximal to submandibular ganglion | (Same as lingual nerve if proximal; loss of taste + salivation if distal) |
Histology
The submandibular gland is a mixed tubuloalveolar gland. Serous acini predominate (like the parotid), but mucous acini are also present, typically capped by serous demilunes. This mixed composition distinguishes it histologically from the purely serous parotid and the predominantly mucous sublingual gland.
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Chapters 35, 41, 43)
- Bailey and Love's Short Practice of Surgery, 28th Ed. (Chapter 54)
- Gray's Anatomy for Students
- Color Atlas of Human Anatomy Vol. 2, Internal Organs
- Scott-Brown's Otorhinolaryngology Vol. 2 (Chapter on facial nerve/ganglion)
Physiology of salivation
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
I have all the material needed for a comprehensive answer. Here it is:
Physiology of Salivation
Overview
Saliva is the combined exocrine secretion of the three pairs of major salivary glands (parotid, submandibular, sublingual) and hundreds of minor salivary glands distributed throughout the oral mucosa. The total daily salivary volume is approximately 1,000-1,500 mL/day, making salivary glands some of the most productive secretory organs per gram of tissue - producing up to 40 times more fluid per unit weight than other digestive secretions.
Contributions by Gland
| Gland | Resting/Unstimulated | Stimulated | Secretion type |
|---|---|---|---|
| Submandibular | 71% | ~35% | Mixed serous/mucous; most viscous |
| Parotid | 25% | ~60% (dominant) | Purely serous; amylase-rich |
| Sublingual | 3-4% | Small fraction | Predominantly mucous |
| Minor glands | Trace | Trace | Mostly mucous |
- At rest: the submandibular gland is the dominant contributor (71%)
- When stimulated: the parotid reverses this and supplies ~two-thirds of flow
- Stimulated saliva accounts for 80-90% of average daily production
Flow Rates
| State | Normal range | Average |
|---|---|---|
| Unstimulated (resting) | ≥0.1 mL/min | ~0.3 mL/min |
| Stimulated | ≥0.2 mL/min | up to 7 mL/min (maximum) |
| Hypofunction threshold | <0.12-0.16 mL/min (unstimulated) | or 50% reduction from individual baseline |
Flow varies with circadian rhythm - lowest during sleep (nocturnal), peak in the afternoon.
Neural Control - The Salivary Reflex
Central Control
Salivary secretion is controlled by the salivary centre in the medulla oblongata, which integrates peripheral afferent stimuli and modulates autonomic output to the glands.
Afferent Stimuli (in order of potency)
- Gustatory - the most potent stimulus; elicits up to a 10-fold increase in flow. Acidic tastes produce the greatest response; sweet tastes are least stimulating
- Mechanoreceptor - stimulation by chewing (receptors in oral mucosa, muscles of mastication, TMJ); salivary flow is directly proportional to applied chewing force
- Olfactory - the weakest physiological stimulus; smell of food triggers anticipatory salivation
- Psychic/conditioned reflexes - anticipation of food, sight
- Nausea - profuse salivation (protective, prior to vomiting)
Habituation occurs with repeated presentation of the same food cue (decreased salivation). Dishabituation follows presentation of novel cues.
Autonomic Innervation - Parasympathetic vs Sympathetic
Parasympathetic (dominant; produces watery, copious secretion)
| Gland | Preganglionic nerve | Ganglion | Postganglionic |
|---|---|---|---|
| Parotid | CN IX (glossopharyngeal) → tympanic branch → lesser petrosal nerve | Otic ganglion | Via auriculotemporal nerve |
| Submandibular & Sublingual | CN VII → chorda tympani → lingual nerve | Submandibular ganglion | Directly to glands |
- Receptor: M3 muscarinic receptors on acinar cells
- Signal: Gq → phospholipase C → IP3 → intracellular Ca²⁺ release → exocytosis of secretory granules + activation of Cl⁻ channels
- Effect: Copious, watery secretion with relatively little organic content (low protein concentration); vasodilation of gland vasculature (via VIP co-release), increasing blood flow and fluid substrate
Sympathetic (produces thick, protein-rich secretion)
- Origin: Superior cervical ganglion → sympathetic plexus on vessels supplying each gland
- Receptor: β-adrenergic on acinar cells (predominant for exocytosis); α-adrenergic (vasoconstriction)
- Effect: Stimulates exocytosis of protein-rich secretory granules (high organic content), but vasoconstriction reduces overall fluid substrate → the net result is reduced volume with viscous, sticky saliva
- This is why anxiety causes dry mouth - sympathetic dominance reduces watery flow while producing thick secretory product
Clinical note: Many drugs with anticholinergic effects (antihistamines, antidepressants, antipsychotics, antimuscarinics) and sympathomimetics reduce salivary flow, causing xerostomia.
Two-Stage Secretion Model
Saliva is produced in two sequential steps:
Stage 1 - Primary Secretion (Acinar Cells)
- Acinar cells secrete a plasma-like isotonic primary fluid (similar electrolyte composition to plasma)
- Na⁺, Cl⁻, K⁺, HCO₃⁻ are secreted in concentrations similar to plasma
- Organic components (enzymes, mucins, proteins) are co-secreted by exocytosis of secretory granules
Stage 2 - Ductal Modification
- As the primary fluid flows through the striated ducts (and then excretory ducts), it is modified:
- Na⁺ is reabsorbed (more than water)
- K⁺ is secreted into the lumen
- HCO₃⁻ is secreted (increasing at higher flow rates - key for buffering)
- Cl⁻ is reabsorbed
- The duct epithelium is relatively impermeable to water, so water does not follow the ions
- Net result: the final saliva is hypotonic relative to plasma, with lower Na⁺, higher K⁺, and variable HCO₃⁻
Effect of Flow Rate on Composition
- At high flow rates (stimulated): less contact time in ducts → less ductal reabsorption → saliva is closer to isotonic, with higher Na⁺ and HCO₃⁻ concentrations → better buffering capacity
- At low flow rates (resting): more ductal contact time → more Na⁺ reabsorption → more hypotonic saliva with lower bicarbonate → reduced buffering
Composition of Saliva
Saliva is 99% water. The remaining 1% is:
Inorganic (electrolytes)
| Ion | Relative to plasma |
|---|---|
| Na⁺ | Lower (10-20 mEq/L vs 140 mEq/L) |
| K⁺ | Higher (~20 mEq/L vs 5 mEq/L) |
| Cl⁻ | Lower |
| HCO₃⁻ | Variable (increases with flow rate) |
| Ca²⁺ | Present (~2-3.6 mEq/L) - important for remineralization |
| HPO₄²⁻ | Present - also for remineralization |
Organic components
| Component | Source gland / function |
|---|---|
| α-Amylase (ptyalin) | Parotid (mainly), submandibular; initiates starch digestion |
| Mucins (MUC1, MUC2) | Sublingual > submandibular > parotid; lubrication, antibacterial |
| sIgA | Plasma cells in gland stroma; aggregates bacteria, prevents mucosal adhesion |
| Lysozyme (muramidase) | Submandibular; cleaves muramic acid in bacterial cell walls |
| Lactoferrin | Scavenges free iron; bacteriostatic, anti-inflammatory |
| Peroxidase | Bactericidal oxidation system |
| Proline-rich proteins | Parotid; lubrication, bind calcium, tooth protection |
| Statherin | Stabilizes Ca²⁺ and PO₄³⁻ in solution; remineralization |
| Histatins | Antifungal (anti-Candida) |
| Cystatins | Cysteine protease inhibitors |
| EGF (epidermal growth factor) | Mucosal healing |
| Urea, ammonia | Nitrogen end-products |
pH of saliva: normally slightly alkaline (~6.8-7.4); drops at very low flow rates
Five Functions of Saliva
1. Lubrication and Protection
- Mucins coat oral mucosa and oropharynx, enabling speech, mastication, and swallowing
- Forms a protective barrier against chemical irritants, proteolytic enzymes (from plaque), and desiccation
- Highest mucin concentrations in minor salivary gland and sublingual saliva
2. Buffering and Clearance
- Bicarbonate is the primary buffer (most important; increases with flow rate)
- Phosphate and histidine-rich proteins are secondary buffers (dominant at low flow rates)
- Urea contributes alkalinity
- Clearance of acids by dilution + swallowing - regional variation ("salivary highways" in the mandibular lingual area vs "byways" near maxillary incisors)
3. Maintenance of Tooth Integrity
- Remineralization: saliva supersaturated with Ca²⁺ and PO₄³⁻ replaces minerals lost from enamel
- Demineralization inhibition: bicarbonate buffering neutralizes acid (pH 5-5.5 threshold for dissolution)
- Protective salivary pellicle formation (statherin, mucins, proline-rich proteins bind hydroxyapatite)
- Fluoride incorporation into enamel crystals
4. Antibacterial Activity
- Immunological: sIgA (aggregation, blocks adhesion), IgG (complement fixation, lysis)
- Non-immunological: lysozyme (cell wall lysis), lactoferrin (iron chelation), peroxidase system, histatins (anti-Candida), mucins (modulate bacterial adhesion)
5. Taste and Digestion
- Solubilises food particles for taste receptor stimulation
- α-Amylase hydrolyses α-1,4 glycosidic bonds (active at neutral pH; inactivated by gastric acid but may continue ~30 min in stomach inside a food bolus)
- Lingual lipase (minor contribution) initiates fat digestion
- Protects taste receptors from desiccation; neutralises bitter/sour stimuli
Factors That Reduce Salivary Flow (Xerostomia)
- Drugs (most common): anticholinergics, antihistamines, tricyclic antidepressants, antipsychotics, diuretics, opioids
- Sjögren's syndrome: autoimmune destruction of acinar cells
- Radiation therapy to head/neck: irreversible fibrosis of gland parenchyma
- Dehydration
- Aging: compounded by polypharmacy, systemic disease
- Anxiety/stress: sympathetic dominance
About 30% of the general population reports some degree of dry mouth. Salivary hypofunction is defined as unstimulated flow <0.12-0.16 mL/min, or a 50% reduction from an individual's baseline.
Sources:
- Cummings Otolaryngology Head and Neck Surgery, Chapter 81 (Saliva - Flow Rate, Composition, Functions)
- Junqueira's Basic Histology, 17e (Chapter 16)
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Chapter 16)
Tests for Salivary flow
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Searching the Web
tests for salivary flow measurement sialometry methods clinical
Reading Web Page
https://iowaprotocols.medicine.uiowa.edu/protocols/sialometr…
Finding Sources
Finding Sources
Searching the Web
Saxon test oral Schirmer test salivary flow clinical methods sialometry techniques
Reading File
Reading File
I now have all the material needed for a thorough answer. Here it is:
Tests for Salivary Flow
Measurement of salivary flow (sialometry) is the objective method for diagnosing salivary gland hypofunction and xerostomia. Tests range from simple chair-side methods to nuclear imaging studies.
Pre-test Conditions (Standardisation)
For reliable, reproducible sialometry, the following conditions should be controlled:
- Perform test in the morning (salivary flow follows a circadian rhythm - highest in the afternoon, lowest at night/early morning; standardising time reduces variability)
- Patient should be fasting for at least 1-2 hours beforehand
- No smoking, toothbrushing, or oral hygiene procedures for at least 1 hour prior
- No medications known to affect flow for at least 12-24 hours (if clinically feasible)
- Patient should be seated upright in a quiet, neutral environment
- Avoid testing during acute oral infection or active sialadenitis
1. Whole Saliva Sialometry
This is the gold standard clinical test and the most widely used. It measures total output from all glands combined.
A. Unstimulated Whole Saliva (UWS)
- What it measures: Baseline (resting) secretion; predominantly submandibular gland (65-71%)
- Method - Drip/Drool method (most common):
- Patient sits quietly for 5 minutes without talking, chewing, or swallowing
- Patient allows saliva to drip passively from the lower lip into a pre-weighed, graduated tube or container
- Volume (or weight) is measured at the end of 5 minutes
- Result expressed as mL/min
- Method - Spitting method: Patient periodically spits accumulated saliva into a tube every 60 seconds for 5-15 minutes
- Normal: ≥0.1 mL/min (average ~0.3 mL/min)
- Hypofunction: <0.1-0.12 mL/min (some sources use <0.16 mL/min as the cut-off)
- More reliable hypofunction definition: a 50% reduction from the individual's own baseline
B. Stimulated Whole Saliva (SWS)
- What it measures: Functional reserve of all glands combined; parotid becomes dominant (50-60%)
- Method - Paraffin chewing (most standard):
- Patient chews a pre-weighed piece of paraffin wax (or tasteless gum) at a regular pace for 5 minutes
- Patient spits accumulated saliva into a pre-weighed graduated tube every 60 seconds (or all at once at 5 minutes)
- Volume or weight measured; result in mL/min
- Method - Citric acid/lemon stimulation: A few drops of citric acid (or lemon juice) applied to the tongue every 30-60 seconds as a gustatory stimulus; saliva collected by spitting
- Citric acid is the most potent gustatory sialagogue; acidic taste produces the greatest salivary response
- Used specifically to stimulate parotid flow (Lashley cup technique)
- Normal: ≥0.7 mL/min (some sources ≥1.0 mL/min)
- Hypofunction: <0.7 mL/min (paraffin-stimulated); some criteria use <0.6 mL/min
2. Individual Gland Collection Methods
These isolate the output of specific glands, useful when asymmetric disease or gland-specific assessment is needed.
Lashley Cup / Carlson-Crittenden Device (Parotid)
- A small suction cup device (Lashley cup) is placed over Stensen's duct orifice at the parotid papilla (opposite upper second molar)
- Dual-chamber design: one chamber collects parotid saliva, the other applies gentle suction to secure the device to the mucosa
- Saliva collected over a timed period with or without gustatory stimulation
- Allows pure parotid saliva collection without contamination from other glands
- Normal stimulated parotid flow: ~0.7 mL/min per gland
Micropipettes / Cannulation (Submandibular/Sublingual)
- Fine-bore micropipettes or cannulae are placed over Wharton's duct orifices at the sublingual caruncles (floor of mouth)
- More technically demanding than parotid collection
- Allows separate collection from each submandibular/sublingual gland
Clinical Duct Expression (Bedside)
- Dry the area around the duct orifice with gauze
- Externally compress and milk the gland toward the duct
- Parotid: compress posterior-to-anterior over the cheek toward Stensen's duct
- Submandibular: bimanual compression (one finger intraoral, one extraoral below mandible) toward Wharton's duct
- Observe character of secretion: clear watery = normal; cloudy/turbid/purulent = infection or ductal obstruction; no flow = hypofunction or obstruction
3. The Saxon Test
- A simple, validated chair-side test for whole saliva output
- Patient chews a pre-weighed sterile gauze swab (4 × 4 cm folded) for 2 minutes
- Swab is re-weighed; the difference = weight of saliva absorbed (in grams; 1 g ≈ 1 mL)
- Normal: ≥2.75 g/2 min (some sources use >2.0 g/2 min)
- Hypofunction: <2.75 g/2 min
- Advantages: simple, no equipment, well-tolerated
- Limitation: primarily reflects stimulated flow; less useful for unstimulated resting assessment
- Scores influenced by age and sex (older patients and women tend to score lower)
4. Oral Schirmer's Test
- Adapted from the ophthalmic Schirmer's test for tear production
- A pre-weighed filter paper strip (Schirmer's strip) is placed in the floor of the mouth or against the buccal mucosa at the duct orifice for 1-5 minutes
- Strip is re-weighed; result expressed as µL/cm²/min or net weight gain
- Useful for assessing minor salivary gland secretion from labial/palatal mucosa
- Can detect hypofunction even when whole saliva sialometry is normal (useful when patient complains of localised oral dryness)
- Validated for Sjögren's syndrome assessment
5. Swab Method
- A pre-weighed cotton swab or absorbent pad is placed in the mouth for a set duration
- Similar principle to the Saxon test; re-weighed after collection
- Reported to be fast, reliable, and capable of distinguishing healthy from hypo-functioning glands
- Well tolerated in outpatient and geriatric settings
6. Radioisotope Salivary Gland Scintigraphy
- Agent: Technetium-99m (⁹⁹ᵐTc) pertechnetate, given as a single IV injection
- Mechanism: ⁹⁹ᵐTc-pertechnetate is actively concentrated by salivary acinar cells (and thyroid), then excreted into the saliva
- Imaging: serial gamma camera images obtained over 30-60 minutes, capturing:
- Uptake phase: active concentration by parenchyma (reflects acinar cell mass/function)
- Excretion phase: secretion into the oral cavity after sialagogue stimulus (lemon juice given at ~20 min)
- Stimulated excretion fraction calculated as:
1 - [(net minimal post-sialagogue counts) / (net maximum pre-sialagogue counts)] × 100 - Uses:
- Assess all four major glands simultaneously
- Evaluate residual function after duct ligation, duct relocation surgery
- Assessment in Sjögren's syndrome, radioiodine-induced damage, post-radiation damage
- Sensitivity: good; Specificity: fairly low; lacks standardised interpretation criteria
- No duct cannulation required; well tolerated
7. Magnetic Resonance Sialography (MR Sialography)
- Non-invasive imaging of the ductal system using heavily T2-weighted sequences (RARE, HASTE, CISS)
- No contrast agent, no radiation, no duct cannulation
- Visualises ductal morphology up to second and third-order branches
- Can be performed even during acute inflammation (conventional sialography is contraindicated during acute infection)
- Replaces conventional sialography in many centres for assessing ductal strictures, sialectasia, stones
8. Conventional Sialography
- Duct cannulation + injection of water-soluble or oil-based contrast agent
- Fluoroscopic or plain radiographic images
- Shows ductal anatomy: strictures, sialectasia, stones, fistulae
- Contraindicated during acute infection
- Being largely replaced by MR sialography and sialendoscopy
- Requires patient cooperation for duct cannulation
9. Minor Salivary Gland Biopsy (Labial Gland Biopsy)
- Not a flow test per se, but the gold standard tissue test for diagnosing salivary gland dysfunction due to Sjögren's syndrome
- Technique: shallow horizontal incision of the lower lip mucosa (halfway between vestibule and vermillion border), 6-7 minor glands excised from lamina propria, fixed in formalin, embedded whole in paraffin
- Focus score calculated: number of lymphocytic foci (clusters ≥50 lymphocytes) per 4 mm² of glandular area
- Abnormal: focus score ≥1 focus/4 mm² (correlates strongly with Sjögren's syndrome)
- Complication: persistent lip numbness in ~2% of patients
Summary: Normal Values and Hypofunction Cut-offs
| Test | Normal | Hypofunction |
|---|---|---|
| Unstimulated whole saliva | ≥0.1 mL/min (avg 0.3) | <0.1-0.16 mL/min |
| Stimulated whole saliva (paraffin) | ≥0.7 mL/min | <0.7 mL/min |
| Saxon test (chewing gauze 2 min) | ≥2.75 g | <2.75 g |
| Stimulated parotid (Lashley cup) | ~0.7 mL/min/gland | reduced |
| Daily output | 1,000-1,500 mL/day | <500 mL/day |
Clinical Approach
- History: xerostomia symptoms, medications, systemic disease (Sjögren's, diabetes, sarcoidosis, HIV), radiation history
- Clinical exam: lip dryness, buccal mucosal dryness, salivary pool in floor of mouth, gland palpation + duct expression
- Sialometry: unstimulated whole saliva first; then stimulated if borderline
- If hypofunction confirmed: serology (anti-Ro/SSA, anti-La/SSB, ANA, RF); imaging (ultrasound, MRI); minor salivary gland biopsy if Sjögren's suspected
- If obstruction suspected (unilateral swelling, mealtime pain): ultrasound, sialography/MR sialography, sialendoscopy
Sources:
- Cummings Otolaryngology Head and Neck Surgery (Chapter 81 - Saliva; Chapter 205 - Sialendoscopy/Imaging)
- Rheumatology 2-Volume Set, Elsevier 2022 (Chapter 146 - Sjögren's Syndrome)
- Iowa Head and Neck Protocols - Sialometry
- University of Southern California, Ostrow School of Dentistry - Salivary Gland and Flow Exam
- Johns Hopkins Sjögren's Center - Sialometry Protocol
This is a shared conversation. Sign in to Orris to start your own chat.