Can you give me easy explanation on ABG why it's important how to treatment acidosis alkalosis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Now I have everything I need to give a thorough, easy explanation. Let me compile it all.
Arterial Blood Gas (ABG) - Easy Guide
What is an ABG and Why Does it Matter?
An ABG is a blood test taken from an artery (usually the radial artery at the wrist). It measures how well your lungs and kidneys are keeping your blood's chemistry in balance. Specifically, it tells you:
| Parameter | Normal Value | What it measures |
|---|---|---|
| pH | 7.35 - 7.45 | How acidic or alkaline the blood is |
| PaCO₂ | 35 - 45 mmHg | Carbon dioxide - controlled by the lungs |
| HCO₃⁻ | 22 - 26 mEq/L | Bicarbonate - controlled by the kidneys |
| PaO₂ | 80 - 100 mmHg | Oxygen in the blood |
Why does it matter? The body can only function normally within a very narrow pH range. When pH falls too low (acidosis) or rises too high (alkalosis), serious consequences follow. Severe acidemia (pH < 7.2) can cause:
- Heart: impaired pumping, dangerous arrhythmias, reduced response to adrenaline
- Lungs: exhausted respiratory muscles
- Metabolism: insulin resistance, high potassium, reduced energy production (ATP)
- Brain: confusion, coma
Severe alkalemia (pH > 7.6) causes:
- Heart: arterial constriction, reduced coronary blood flow, arrhythmias
- Electrolytes: low potassium, low calcium and magnesium (causing muscle cramps, tingling, spasms)
The 4 Disorders - Simple Summary
Think of it this way: two organs control pH - the lungs (via CO₂) and the kidneys (via HCO₃⁻). When either fails, you get an acid-base disorder.
pH < 7.35 = ACIDOSIS (too acid)
pH > 7.45 = ALKALOSIS (too alkaline)
1. Respiratory Acidosis
- What: Lungs can't blow off enough CO₂ → CO₂ builds up → acid rises
- ABG: pH ↓, PaCO₂ ↑
- Common causes: COPD, pneumonia, asthma, drug overdose (opioids/sedatives), Guillain-Barré, obesity hypoventilation
- The body compensates: Kidneys retain HCO₃⁻ (takes 48-96 hours)
2. Respiratory Alkalosis
- What: Lungs blow off too much CO₂ (hyperventilation) → acid drops
- ABG: pH ↑, PaCO₂ ↓
- Common causes: Anxiety/panic, pain, fever, sepsis, pregnancy, salicylate toxicity, pulmonary embolism
- Watch out: Causes low ionized calcium → tingling lips, hand spasms (carpal spasm), syncope
- The body compensates: Kidneys excrete HCO₃⁻ (takes 48-96 hours)
3. Metabolic Acidosis
- What: Too much acid produced OR too much bicarbonate lost → pH falls
- ABG: pH ↓, HCO₃⁻ ↓
- Common causes (use the mnemonic MUDPILES for high anion gap):
| MUDPILES (high anion gap) | HARDUP (normal anion gap) |
|---|---|
| Methanol | Hyperalimentation / Hospital saline |
| Uremia | Acid infusion / Addison's / CA inhibitors |
| DKA (diabetic ketoacidosis) | Renal tubular acidosis |
| Propylene glycol / Paraldehyde | Diarrhea |
| Isoniazid / Iron | Ureterosigmoidostomy |
| Lactic acidosis (most common!) | Pancreatic fistula |
| Ethylene glycol | |
| Salicylates |
- The body compensates: Lungs hyperventilate to blow off CO₂ (within 12-24 hours). Use Winter's formula to check: PaCO₂ = (1.5 × HCO₃⁻) + 8 ± 2
4. Metabolic Alkalosis
- What: Too much bicarbonate gained OR too much acid lost → pH rises
- ABG: pH ↑, HCO₃⁻ ↑
- Common causes:
- Chloride-responsive (urine Cl⁻ < 25): vomiting, nasogastric suction, diuretics, diarrhea (chloride-wasting)
- Chloride-unresponsive (urine Cl⁻ > 40): hyperaldosteronism, Cushing's, severe hypomagnesemia, steroids
- The body compensates: Lungs hypoventilate to retain CO₂ (PaCO₂ = 0.7 × HCO₃⁻ + 20 ± 5)
How to Interpret an ABG - 4 Simple Steps
Step 1: Look at the pH
- pH < 7.35 = Acidosis
- pH > 7.45 = Alkalosis
Step 2: Find the cause (respiratory or metabolic?)
- pH ↓ + PaCO₂ ↑ = Respiratory Acidosis
- pH ↓ + HCO₃⁻ ↓ = Metabolic Acidosis
- pH ↑ + PaCO₂ ↓ = Respiratory Alkalosis
- pH ↑ + HCO₃⁻ ↑ = Metabolic Alkalosis
Step 3: Check compensation (is the other organ trying to fix it?)
Step 4: Calculate the anion gap if metabolic acidosis is present (AG = Na⁺ - Cl⁻ - HCO₃⁻, normal < 13)
Treatment
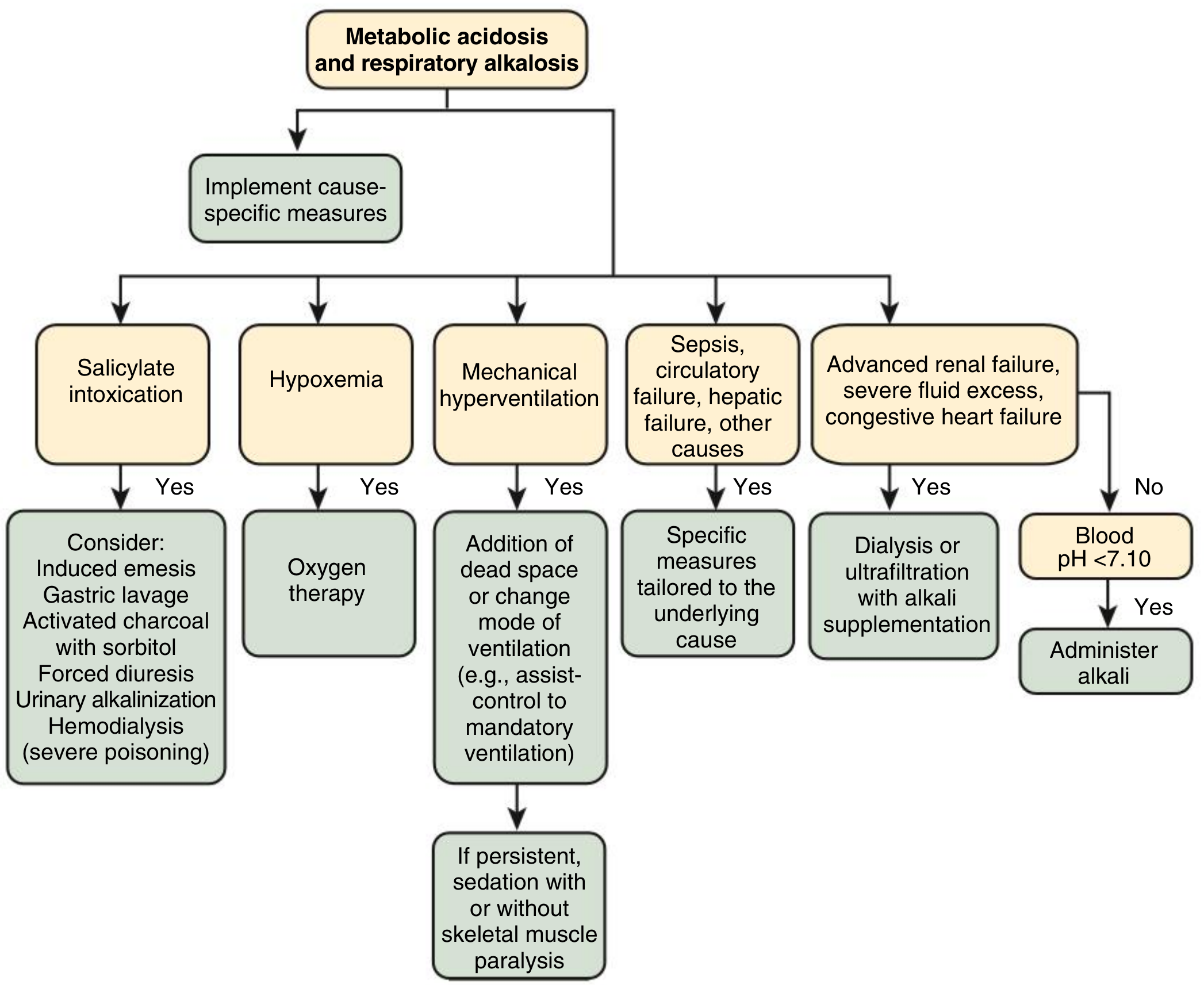
Metabolic Acidosis Treatment
The most important rule: treat the underlying cause first.
- DKA → insulin + fluids
- Lactic acidosis → fix the cause of poor perfusion
- Salicylate toxicity → gastric lavage, activated charcoal, urinary alkalinization, hemodialysis in severe cases
- If pH < 7.10 and cause not quickly correctable → consider sodium bicarbonate (NaHCO₃)
- Renal failure → dialysis or ultrafiltration with alkali supplementation
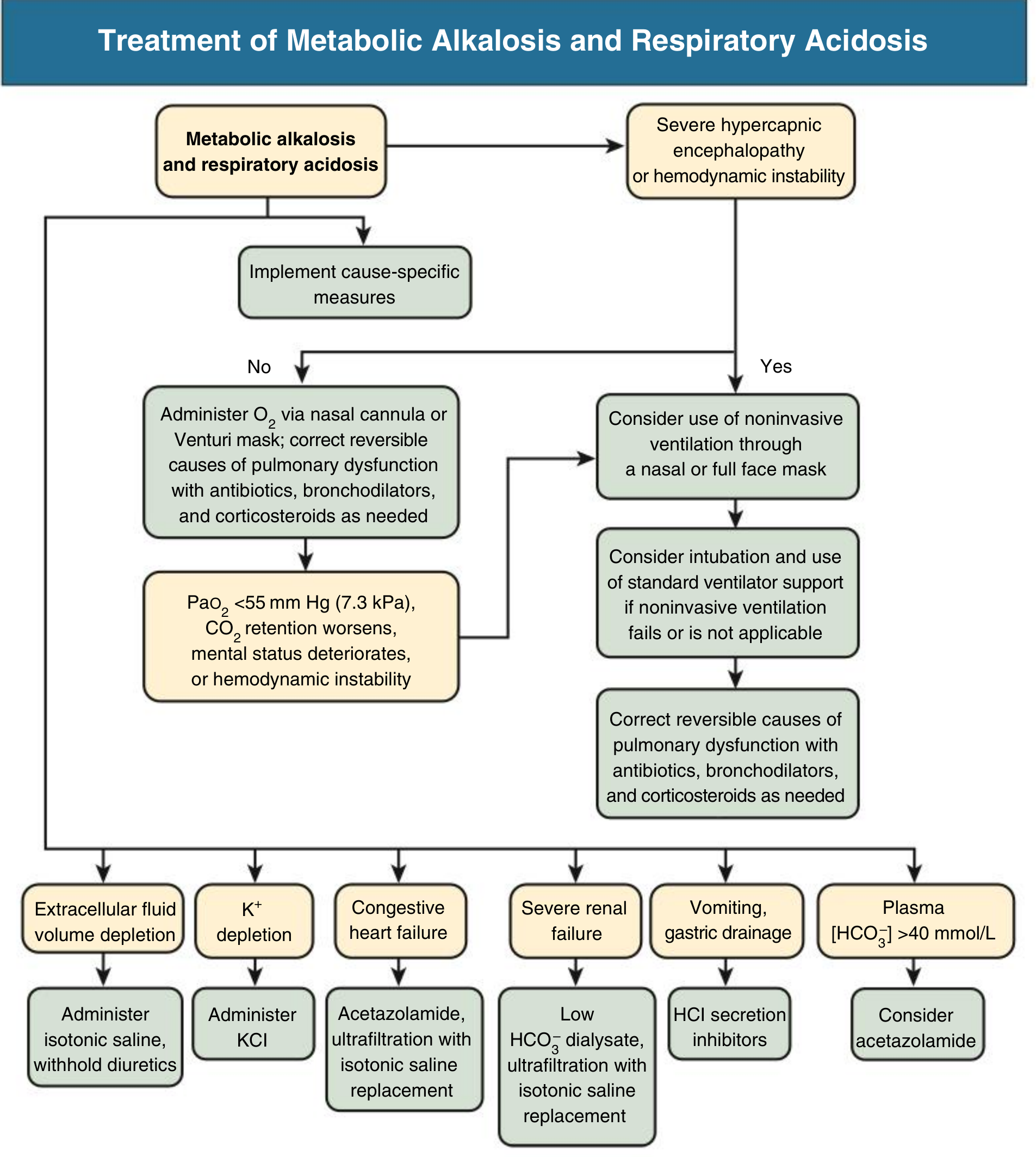
Respiratory Acidosis Treatment
- Fix the lungs - treat the underlying cause (antibiotics for pneumonia, bronchodilators for COPD/asthma, corticosteroids)
- Oxygen via nasal cannula or Venturi mask
- If severe (hypercapnic encephalopathy or hemodynamic instability) → non-invasive ventilation (BiPAP/CPAP) first, then intubation and mechanical ventilation if that fails
Metabolic Alkalosis Treatment
- Chloride-responsive: Give isotonic saline (IV fluids) + withhold diuretics; replace potassium (KCl) if low
- Chloride-unresponsive: Treat the cause (e.g., remove aldosterone source); consider acetazolamide, HCl secretion inhibitors (omeprazole if due to gastric drainage), or ultrafiltration
- Congestive heart failure with alkalosis → acetazolamide or ultrafiltration with isotonic saline replacement
Respiratory Alkalosis Treatment
- Treat the underlying cause (reassure anxious patient, treat pain/fever/sepsis)
- Hyperventilation on a ventilator → reduce respiratory rate or add dead space
- The alkalosis itself resolves as cause is fixed; do NOT use CO₂ rebreathing (paper bag) routinely - it can be dangerous
Treatment Flowcharts (from Comprehensive Clinical Nephrology)
Metabolic Alkalosis + Respiratory Acidosis:
Metabolic Acidosis + Respiratory Alkalosis:
Quick Reference Cheat Sheet
| Disorder | pH | Primary Change | Compensation | Key Causes |
|---|---|---|---|---|
| Respiratory Acidosis | ↓ | PaCO₂ ↑ | HCO₃⁻ ↑ | COPD, OD, pneumonia |
| Respiratory Alkalosis | ↑ | PaCO₂ ↓ | HCO₃⁻ ↓ | Anxiety, PE, sepsis |
| Metabolic Acidosis | ↓ | HCO₃⁻ ↓ | PaCO₂ ↓ | DKA, lactic acidosis, diarrhea |
| Metabolic Alkalosis | ↑ | HCO₃⁻ ↑ | PaCO₂ ↑ | Vomiting, diuretics |
Sources: Barash et al., Clinical Anesthesia, 9e | Rosen's Emergency Medicine | Comprehensive Clinical Nephrology, 7e
This is a shared conversation. Sign in to Orris to start your own chat.