Oral antidiabetic drugs
Oral Antidiabetic Drugs
Overview of Classes
| Class | Mechanism | Key Agents | Hypoglycemia Risk |
|---|---|---|---|
| Biguanides | ↓ Hepatic gluconeogenesis | Metformin | Low |
| Sulfonylureas | ↑ Insulin secretion (K⁺-ATP channel closure) | Glipizide, Glimepiride, Glyburide | High |
| Meglitinides | ↑ Insulin secretion (rapid onset) | Repaglinide, Nateglinide | Low-moderate |
| Thiazolidinediones | Insulin sensitizers (PPARγ agonists) | Pioglitazone, Rosiglitazone | Low |
| Alpha-glucosidase inhibitors | ↓ Carbohydrate absorption | Acarbose, Miglitol | Very low |
| DPP-4 Inhibitors | ↑ Incretin (GLP-1/GIP) levels | Sitagliptin, Saxagliptin, Linagliptin | Very low |
| SGLT-2 Inhibitors | ↑ Urinary glucose excretion | Empagliflozin, Dapagliflozin, Canagliflozin | Very low |
| GLP-1 RAs (oral) | Incretin mimetic | Semaglutide (oral only) | Low |
| Bile acid sequestrant | Unclear | Colesevelam | Very low |
1. Biguanides - Metformin
- Primarily reduces hepatic gluconeogenesis (targets excess fasting glucose)
- Slows intestinal glucose absorption
- Improves peripheral glucose uptake and insulin sensitivity
- Does not stimulate insulin secretion → minimal hypoglycemia risk
- Well absorbed orally, not bound to plasma proteins, not metabolized
- Excreted unchanged by the kidneys
- GI: diarrhea, nausea, vomiting (most common; alleviated by slow titration and taking with meals)
- Lactic acidosis - rare but serious; risk increases with renal impairment
- Vitamin B12 malabsorption with chronic use
- Weight loss (decreases appetite)
- eGFR < 30 mL/min (hold if eGFR 30-45)
- IV contrast procedures (hold for 48 hours)
- Hepatic impairment, alcoholism, heart failure
2. Sulfonylureas
- Bind SUR1 subunit of ATP-sensitive K⁺ channels on β cells → channel closure → membrane depolarization → Ca²⁺ influx → insulin release
- Action is glucose-independent (hence hypoglycemia risk)
- 1st generation (older, more side effects): Tolbutamide, Chlorpropamide
- 2nd generation (preferred): Glipizide, Glyburide (Glibenclamide), Glimepiride
- All well absorbed orally; extensively protein-bound
- Metabolized by liver; renal excretion of metabolites
- Hypoglycemia (most important - especially glyburide, which has active metabolites and is long-acting; avoid in elderly and renal impairment)
- Weight gain
- Disulfiram-like reaction with alcohol (especially chlorpropamide)
- Drug interactions: NSAIDs, sulfonamides, warfarin can potentiate hypoglycemia
3. Meglitinides
- Same target as sulfonylureas (K⁺-ATP channels) but faster onset and shorter duration
- Particularly effective for postprandial glucose control
- Taken before each meal
- Repaglinide: metabolized by CYP2C8/CYP3A4, excreted in feces
- Nateglinide: metabolized by CYP2C9/CYP3A4, excreted in urine
- Gemfibrozil (a CYP2C8 inhibitor) markedly increases repaglinide levels - combination is contraindicated
- Hypoglycemia and weight gain, but less than sulfonylureas
- Do NOT combine with sulfonylureas (overlapping mechanism, high hypoglycemia risk)
- Use with caution in hepatic impairment
4. Thiazolidinediones (TZDs) - "Glitazones"
- Agonists at PPARγ (peroxisome proliferator-activated receptor-γ), a nuclear receptor
- PPARγ activation regulates transcription of insulin-responsive genes
- Increases insulin sensitivity in adipose tissue, liver, and skeletal muscle
- Do NOT cause hyperinsulinemia (no direct insulin secretion)
- Well absorbed; extensively bound to serum albumin
- Metabolized primarily by CYP2C8
- Pioglitazone: excreted in bile/feces; no dose adjustment in renal impairment
- Rosiglitazone: urinary excretion of metabolites
- Weight gain (increased subcutaneous fat)
- Fluid retention → worsen or precipitate heart failure (avoid in symptomatic HF)
- Osteopenia and fracture risk (especially in women)
- Pioglitazone: possible association with bladder cancer (avoid in bladder cancer history)
- Rosiglitazone: cardiovascular concerns limit its use
5. Alpha-Glucosidase Inhibitors
- Inhibit alpha-glucosidase enzymes in the brush border of the small intestine
- Delay digestion and absorption of complex carbohydrates
- Reduce postprandial glucose spikes
- Taken with the first bite of each meal
- GI: flatulence, bloating, diarrhea, abdominal cramps (most common; limits use)
- Very low hypoglycemia risk as monotherapy
- If hypoglycemia occurs while on alpha-glucosidase inhibitors (in combination), treat with glucose (dextrose), not sucrose - sucrose digestion is blocked
6. DPP-4 Inhibitors ("Gliptins")
- Inhibit dipeptidyl peptidase-4 (DPP-4), the enzyme that inactivates incretin hormones (GLP-1 and GIP)
- Result: prolonged action of endogenous GLP-1 and GIP
- Effect is glucose-dependent → stimulates insulin secretion only when glucose is elevated; also suppresses glucagon
- Generally well tolerated; weight neutral
- Nasopharyngitis, upper respiratory tract infections
- Rare: pancreatitis; urticaria/angioedema
- Saxagliptin and alogliptin: possible association with increased heart failure hospitalization
- Linagliptin: non-renal elimination (safest in CKD)
7. SGLT-2 Inhibitors ("Gliflozins")
- Inhibit sodium-glucose cotransporter 2 (SGLT-2) in the proximal renal tubule
- Block renal glucose reabsorption → glycosuria → lower blood glucose
- Mechanism is entirely insulin-independent
- Also reduce blood pressure, weight, and have direct cardiac and renal protective effects
- Empagliflozin (EMPA-REG OUTCOME) and canagliflozin (CANVAS): reduced MACE, CV death, HF hospitalization
- Preferred as add-on to metformin in patients with established ASCVD, heart failure, or diabetic nephropathy
- Genital mycotic infections (most common - due to glycosuria)
- UTIs
- Euglycemic DKA (rare but serious; drug must be held before surgery/prolonged fasting)
- Fournier's gangrene (necrotizing fasciitis of perineum) - rare
- Canagliflozin: increased risk of lower limb amputation and bone fractures
- Polyuria, dehydration, hypotension
- Avoid if eGFR < 30 (reduced efficacy; though some agents allowed down to eGFR 20 for HF/renal protection)
8. Bile Acid Sequestrant
- Approved as add-on for type 2 diabetes; mechanism of glucose lowering is unclear
- Reduces A1c by ~0.5% when added to metformin, sulfonylurea, or insulin
- Also lowers LDL cholesterol
9. Oral Semaglutide (GLP-1 Receptor Agonist)
- Only oral GLP-1 receptor agonist currently available
- Same mechanism as injectable GLP-1 RAs: stimulates GLP-1 receptor in a glucose-dependent manner
- Slows gastric emptying, reduces appetite, promotes weight loss
- Requires specific administration: taken fasting with a small amount of water, no food for 30 minutes after
Treatment Algorithm for Type 2 Diabetes
- Start: Metformin + lifestyle modification at diagnosis
- If A1c target not achieved in 2-3 months: add a second agent
- Established ASCVD/high CV risk: add GLP-1 RA or SGLT-2 inhibitor
- Heart failure or CKD: prefer SGLT-2 inhibitor
- Need for weight loss: prefer GLP-1 RA or SGLT-2 inhibitor
- Cost is a concern: add sulfonylurea
- Further escalation: Triple therapy (metformin + two agents) or add basal insulin
- Reinforce lifestyle at every visit; check A1c every 3 months
Key Comparison Points for Exams
| Property | Metformin | SU | TZD | DPP-4i | SGLT-2i | GLP-1 RA |
|---|---|---|---|---|---|---|
| Hypoglycemia | No | Yes | No | No | No | No |
| Weight | Neutral/↓ | ↑ | ↑ | Neutral | ↓ | ↓ |
| CV benefit | Neutral | Neutral | Rosig: ↑ risk | Neutral/↑HF | ↓MACE, HF | ↓MACE |
| Renal protection | - | - | - | - | Yes | Some |
| GI side effects | Yes | - | - | - | - | Yes |
| Use in CKD | Caution/avoid | Avoid (glyburide) | Ok | Linagliptin ok | Limit | Use with caution |
Mechanism of action,uses and adverse effects of metformin and glibenclamide
Metformin and Glibenclamide - Mechanism, Uses & Adverse Effects
METFORMIN (Biguanide)
Mechanism of Action
- Metformin inhibits mitochondrial Complex I in hepatocytes, raising the AMP:ATP ratio
- This activates AMP-activated protein kinase (AMPK), which suppresses expression of gluconeogenic enzymes (PEPCK, G6Pase)
- Excess hepatic glucose output is the main driver of fasting hyperglycemia in type 2 diabetes - metformin directly tackles this
- Delays carbohydrate absorption from the gut, blunting postprandial glucose spikes
- Increases glucose uptake and utilization in skeletal muscle
- Does NOT stimulate insulin secretion from β cells → no hyperinsulinemia, minimal hypoglycemia risk as monotherapy
Uses
| Indication | Notes |
|---|---|
| Type 2 diabetes mellitus | First-line drug; started at diagnosis per ADA/all major guidelines |
| Prevention of type 2 diabetes | Beneficial in patients with prediabetes (reduces progression) |
| Polycystic ovary syndrome (PCOS) | Reduces insulin resistance; improves menstrual regularity and ovulation |
| Metabolic syndrome | Off-label use for insulin resistance management |
| Pediatric type 2 diabetes | Only oral agent FDA-approved for children ≥10 years |
| Combination therapy | Used with sulfonylureas, DPP-4i, SGLT-2i, GLP-1 RAs, or insulin |
Pharmacokinetics
- Absorption: Well absorbed orally; bioavailability ~50-60%
- Protein binding: None (not bound to plasma proteins)
- Metabolism: Not metabolized - excreted unchanged
- Excretion: Renal (unchanged drug) - explains why renal impairment is dangerous
Adverse Effects
- Diarrhea, nausea, vomiting, metallic taste, abdominal cramps
- Minimized by: slow dose titration + taking with meals
- Usually transient; often resolve within weeks
- Occurs because metformin inhibits hepatic lactate clearance (lactate → gluconeogenesis pathway is blocked)
- Risk factors: renal impairment, hepatic failure, sepsis, dehydration, excessive alcohol
- Mortality ~50% when it occurs
- Contraindicated in eGFR < 30 mL/min/1.73 m²; use with caution at eGFR 30-45
- Long-term use reduces B12 absorption (interferes with ileal B12-intrinsic factor complex uptake)
- Periodic monitoring recommended, especially in patients with anemia or peripheral neuropathy
- Weight neutral to slight weight loss (reduces appetite)
Contraindications
| Contraindication | Reason |
|---|---|
| eGFR < 30 mL/min | Accumulation → lactic acidosis |
| IV contrast media procedures | Hold 48 hours pre/post (contrast can cause acute kidney injury) |
| Acute myocardial infarction, sepsis, severe dehydration | Risk of acute renal failure → lactic acidosis |
| Hepatic impairment, alcohol abuse | Impaired lactate clearance |
| Age > 80 years (caution) | Reduced renal reserve |
| Symptomatic heart failure (caution) | Reduced perfusion to kidneys |
GLIBENCLAMIDE (Glyburide) - 2nd Generation Sulfonylurea
Note: Glibenclamide is the international non-proprietary name (INN); glyburide is the name used in the USA. It is 100-200 times more potent than 1st generation sulfonylureas.
Mechanism of Action
- Glibenclamide binds to the SUR1 subunit (140-kDa high-affinity sulfonylurea receptor) on the β-cell membrane
- SUR1 is associated with an inward rectifier ATP-sensitive K⁺ channel (K_ATP channel)
- Binding inhibits K⁺ efflux through the channel → membrane depolarization
- Depolarization opens voltage-gated L-type Ca²⁺ channels
- Ca²⁺ influx triggers exocytosis of preformed insulin granules
- Net result: increased insulin release
This mechanism mirrors the normal glucose-stimulated insulin secretion pathway, but glibenclamide acts regardless of blood glucose level - this is the basis for its hypoglycemia risk.
- May reduce hepatic glucose output
- May increase peripheral insulin sensitivity (secondary to improved glycemic control)
- Unique property: Glibenclamide also becomes sequestered within the β cell after binding, contributing to its prolonged biologic effect (24 hours) despite a short plasma half-life of 1-2 hours
Uses
| Indication | Notes |
|---|---|
| Type 2 diabetes mellitus | Monotherapy or combination (commonly with metformin) |
| Gestational diabetes | Used where insulin is not available; crosses placenta (caution) |
| Neonatal diabetes (due to KATP channel mutations) | Off-label; highly effective in KCNJ11/ABCC8 mutations |
| Combination with metformin | Additive glucose-lowering; complementary mechanisms |
Pharmacokinetics
| Parameter | Detail |
|---|---|
| Absorption | Well absorbed orally |
| Protein binding | Extensively bound to serum albumin |
| Metabolism | Hepatic - metabolites have hypoglycemic activity |
| Half-life | 1-2 hours (plasma), but biologic effect persists 24 hours |
| Excretion | Bile/feces and urine |
| Dosing | Starting dose: 2.5 mg/day; usual: 5-10 mg/day; max: 20 mg/day |
Adverse Effects
- Most serious adverse effect
- Occurs because insulin release is glucose-independent
- Particularly dangerous in: elderly patients, renal impairment (active metabolites accumulate), liver failure, missed meals, excessive exercise, alcohol
- Can be prolonged and severe (lasts 24-36 hours due to active metabolites)
- Glibenclamide has the highest hypoglycemia risk among 2nd generation sulfonylureas
- Due to hyperinsulinemia → increased lipogenesis and appetite
- Average gain: 2-4 kg
- SUR2A receptors on cardiac muscle are also blocked by glibenclamide → may impair ischemic preconditioning of the myocardium (a protective response to ischemia)
- Not recommended in patients with significant cardiovascular disease
- Flushing after ethanol ingestion (more common with chlorpropamide; occurs occasionally with glibenclamide)
- Nausea, vomiting, cholestatic jaundice (rare)
- Leukopenia, thrombocytopenia, hemolytic anemia
- NSAIDs, sulfonamides, warfarin, fluconazole, salicylates (displace from protein binding or inhibit metabolism)
- Beta-blockers (mask tachycardia warning of hypoglycemia; also inhibit glycogenolysis)
Contraindications
| Contraindication | Reason |
|---|---|
| Renal impairment (CrCl < 30 mL/min) | Active metabolites accumulate → prolonged hypoglycemia |
| Hepatic failure | Impaired metabolism → drug accumulation |
| Type 1 diabetes / DKA | No β cell function to stimulate |
| Elderly patients (relative) | High hypoglycemia risk; use shorter-acting alternatives |
| Pregnancy | Sulfonylureas cross placenta → neonatal hypoglycemia |
Side-by-Side Comparison
| Feature | Metformin | Glibenclamide |
|---|---|---|
| Class | Biguanide | 2nd-generation sulfonylurea |
| Primary mechanism | ↓ Hepatic gluconeogenesis (AMPK) | Closes β-cell K_ATP channels → ↑ insulin secretion |
| Requires insulin secretion? | No | Yes (needs functioning β cells) |
| Hypoglycemia risk | Minimal (monotherapy) | High |
| Weight | Neutral / slight ↓ | ↑ Weight gain |
| A1c reduction | 1-2% | 1-2% |
| Serious ADR | Lactic acidosis (rare) | Severe/prolonged hypoglycemia |
| Renal impairment | Avoid (eGFR <30) | Avoid (active metabolites) |
| Cardiovascular | Neutral/beneficial | Caution (ischemic preconditioning) |
| First-line? | YES - always first line | Second-line / adjunct |
Explain how levels of calcium is regulated with help of diagram
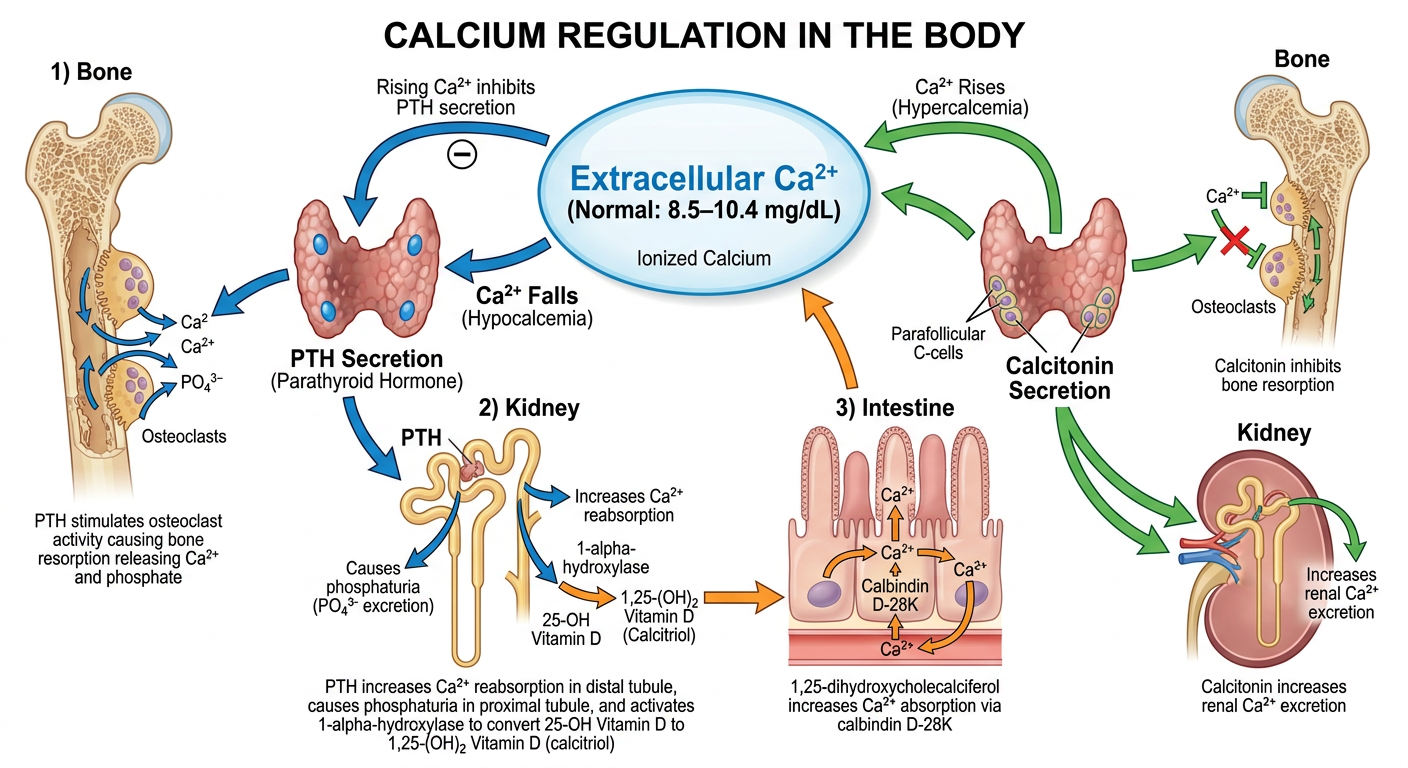
A detailed medical physiology diagram showing calcium regulation in the body. Central oval labeled "Extracellular Ca2+ (Normal: 8.5–10.4 mg/dL)". When Ca2+ falls, arrows show PTH secretion from parathyroid glands, with three downstream pathways: 1) Bone - PTH stimulates osteoclast activity causing bone resorption releasing Ca2+ and phosphate; 2) Kidney - PTH increases Ca2+ reabsorption in distal tubule, causes phosphaturia in proximal tubule, and activates 1-alpha-hydroxylase to convert 25-OH Vitamin D to 1,25-(OH)2 Vitamin D (calcitriol); 3) Intestine - 1,25-dihydroxycholecalciferol increases Ca2+ absorption via calbindin D-28K. When Ca2+ rises, calcitonin from parafollicular C-cells of thyroid inhibits bone resorption and increases renal Ca2+ excretion. Feedback arrow shows rising Ca2+ inhibits PTH secretion. The diagram uses a clean, color-coded layout with blue for PTH pathway, orange for Vitamin D pathway, and green for calcitonin pathway.
Regulation of Calcium Levels
1. Forms of Calcium in Blood
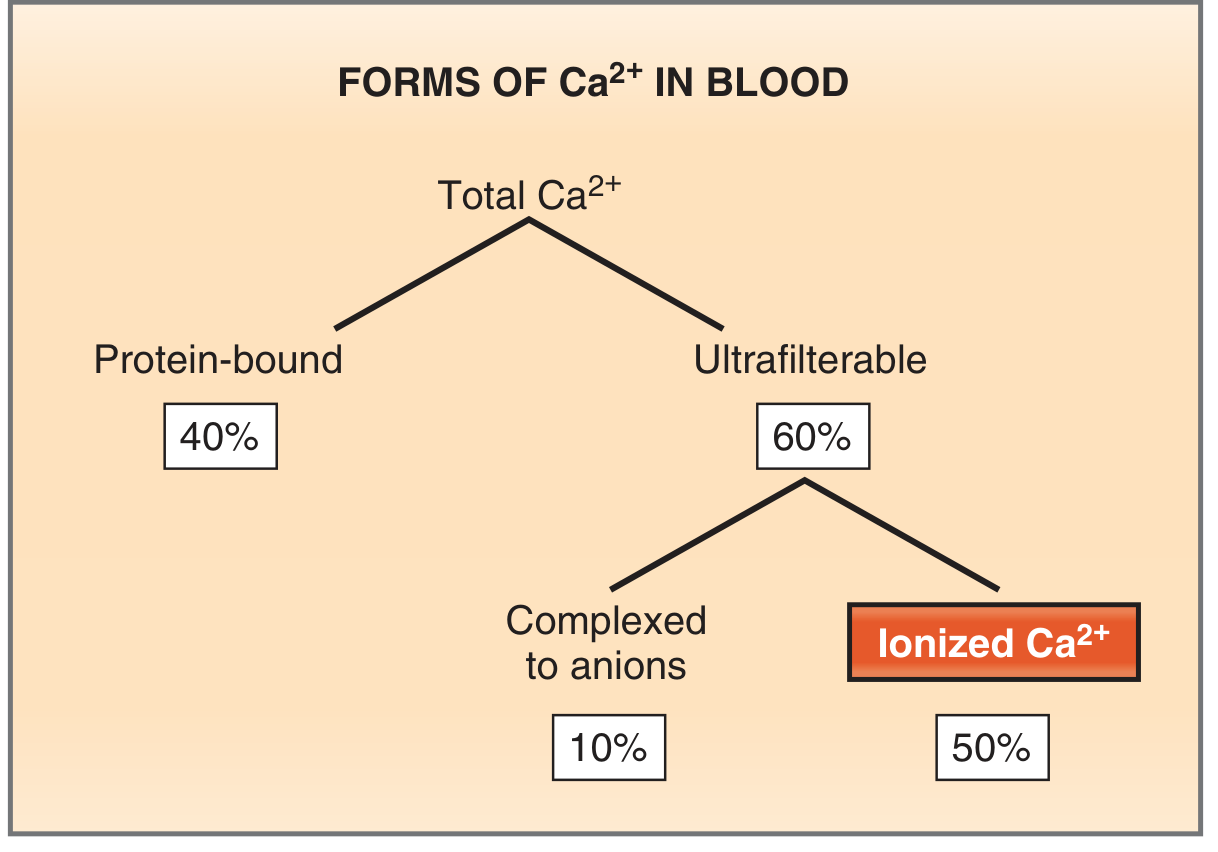
| Form | Percentage | Notes |
|---|---|---|
| Protein-bound | 40% | Mainly albumin; not biologically active |
| Complexed to anions | 10% | Bound to phosphate, sulfate, citrate |
| Free ionized Ca²⁺ | 50% | Only biologically active form |
The body contains ~1000-1300 g of calcium total; >99% is stored in bone and teeth. The extracellular Ca²⁺ pool (in ECF/blood) is the tightly regulated compartment.
2. Overall Calcium Homeostasis - The Big Picture
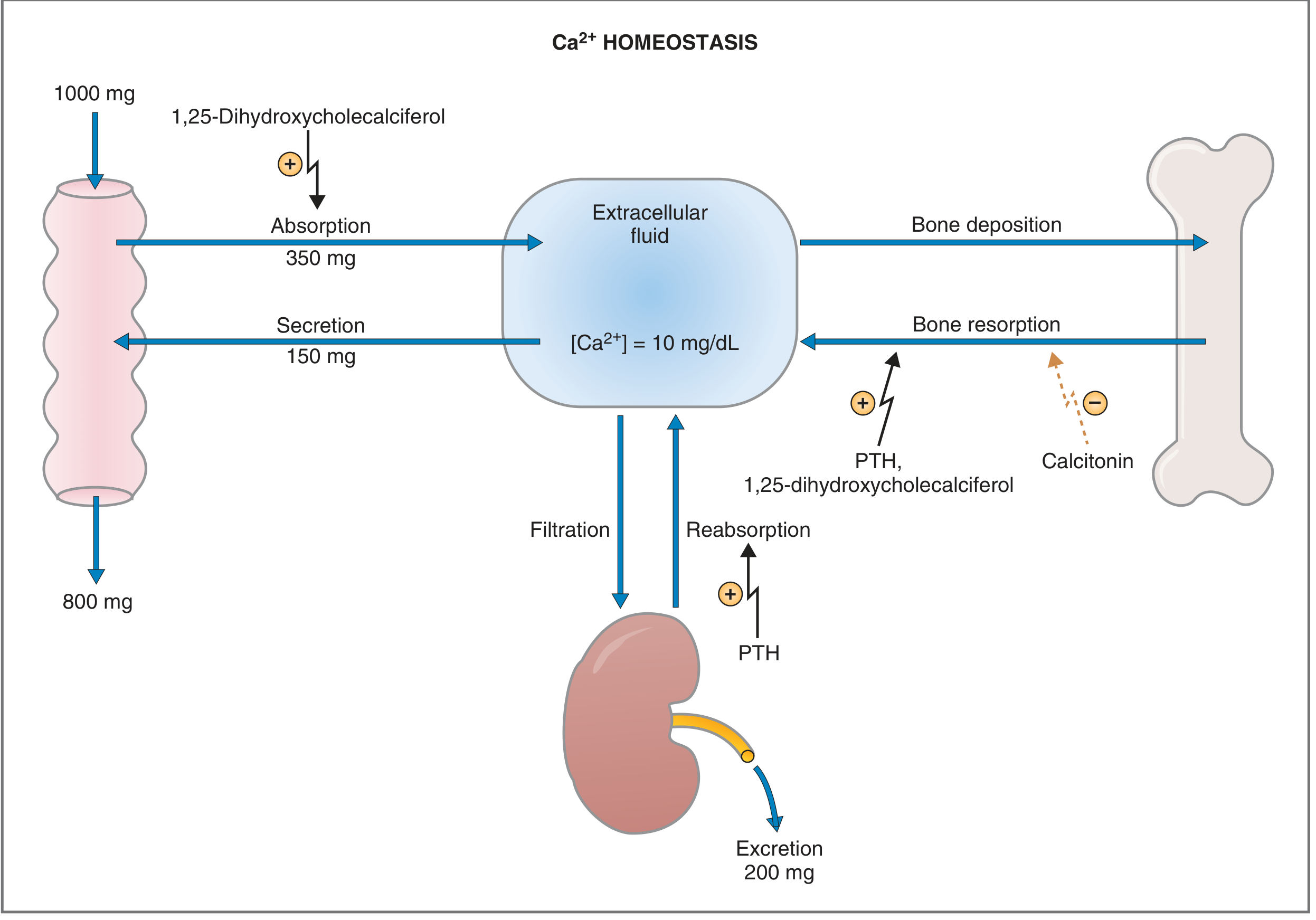
- 350 mg absorbed from the gut (stimulated by 1,25-(OH)₂ Vitamin D)
- 150 mg secreted back into the gut = net absorption 200 mg/day
- 800 mg excreted in feces
- Kidneys filter ~10,000 mg/day and reabsorb ~9,800 mg → excrete 200 mg/day (matching absorption to maintain balance)
3. The Three Regulatory Hormones
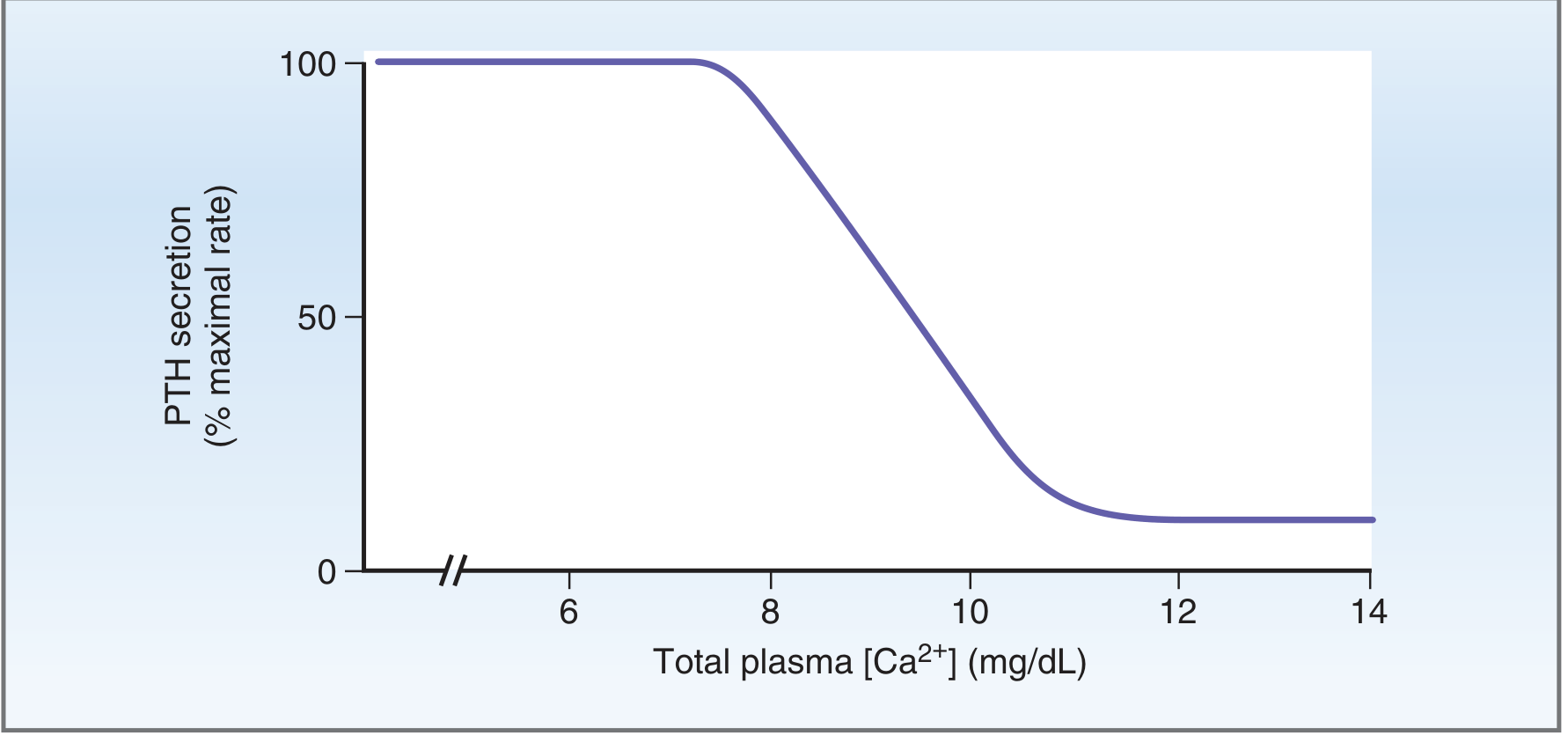
A. Parathyroid Hormone (PTH)
- Secreted by chief cells of the 4 parathyroid glands
- Parathyroid cells express a Calcium-Sensing Receptor (CaSR) linked via Gq to phospholipase C
- When Ca²⁺ falls → less CaSR activation → less IP₃/Ca²⁺ signaling → PTH secretion increases (within seconds)
- When Ca²⁺ rises → CaSR activated → inhibits PTH
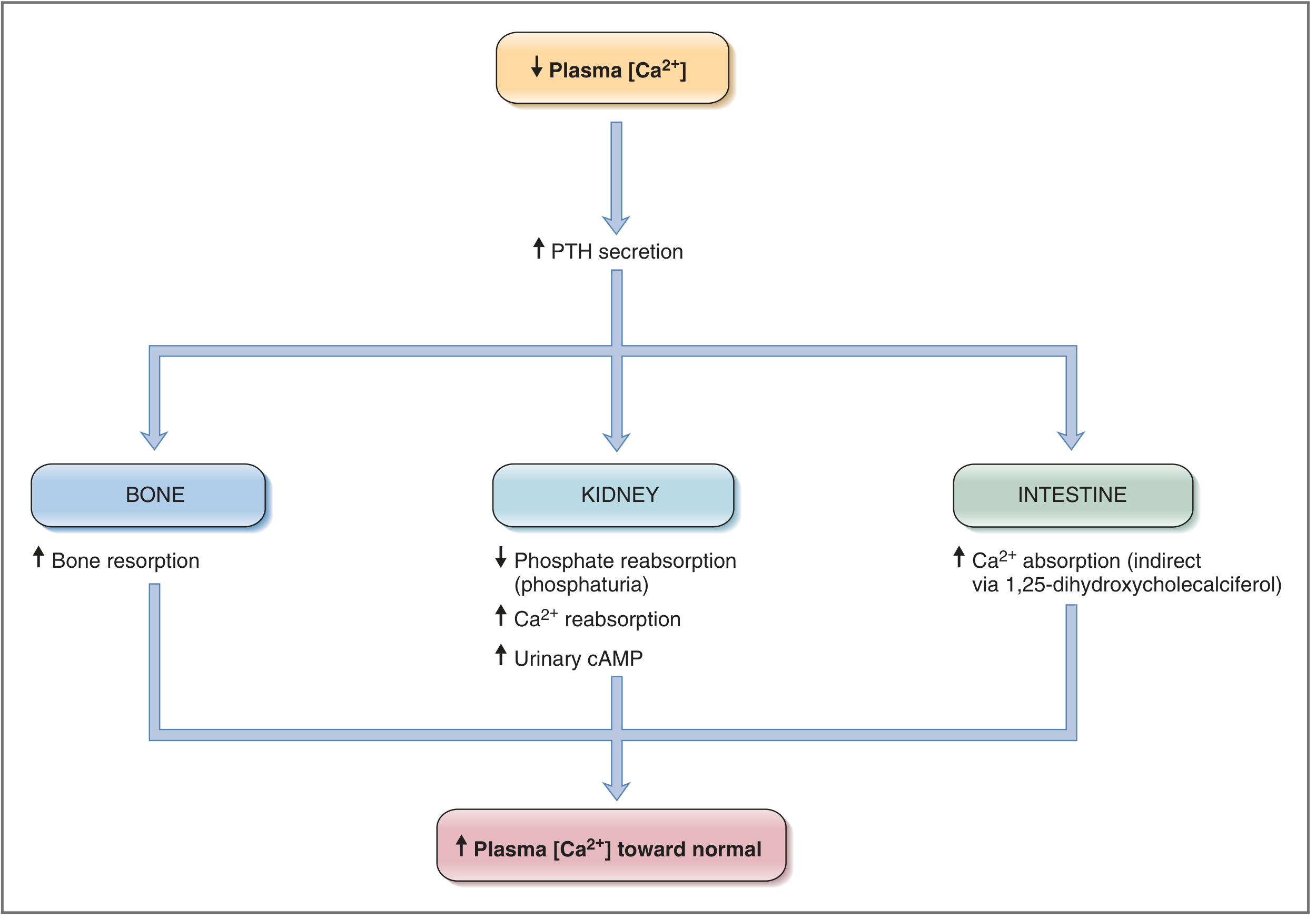
| Target | PTH Action | Net Effect |
|---|---|---|
| Bone | Initially stimulates osteoblasts (brief); then activates osteoclasts indirectly (via cytokines from osteoblasts) | ↑ Bone resorption → Ca²⁺ and PO₄³⁻ released into ECF |
| Kidney (proximal tubule) | Inhibits Na⁺-phosphate cotransporter → phosphaturia | ↓ Serum phosphate (prevents Ca²⁺-PO₄ complexing → allows ionized Ca²⁺ to rise) |
| Kidney (distal tubule) | Stimulates Ca²⁺ reabsorption | ↑ Serum Ca²⁺, ↑ urinary cAMP (nephrogenous cAMP) |
| Kidney (proximal tubule) | Activates 1α-hydroxylase | 25-OH Vitamin D → 1,25-(OH)₂ Vitamin D (calcitriol) |
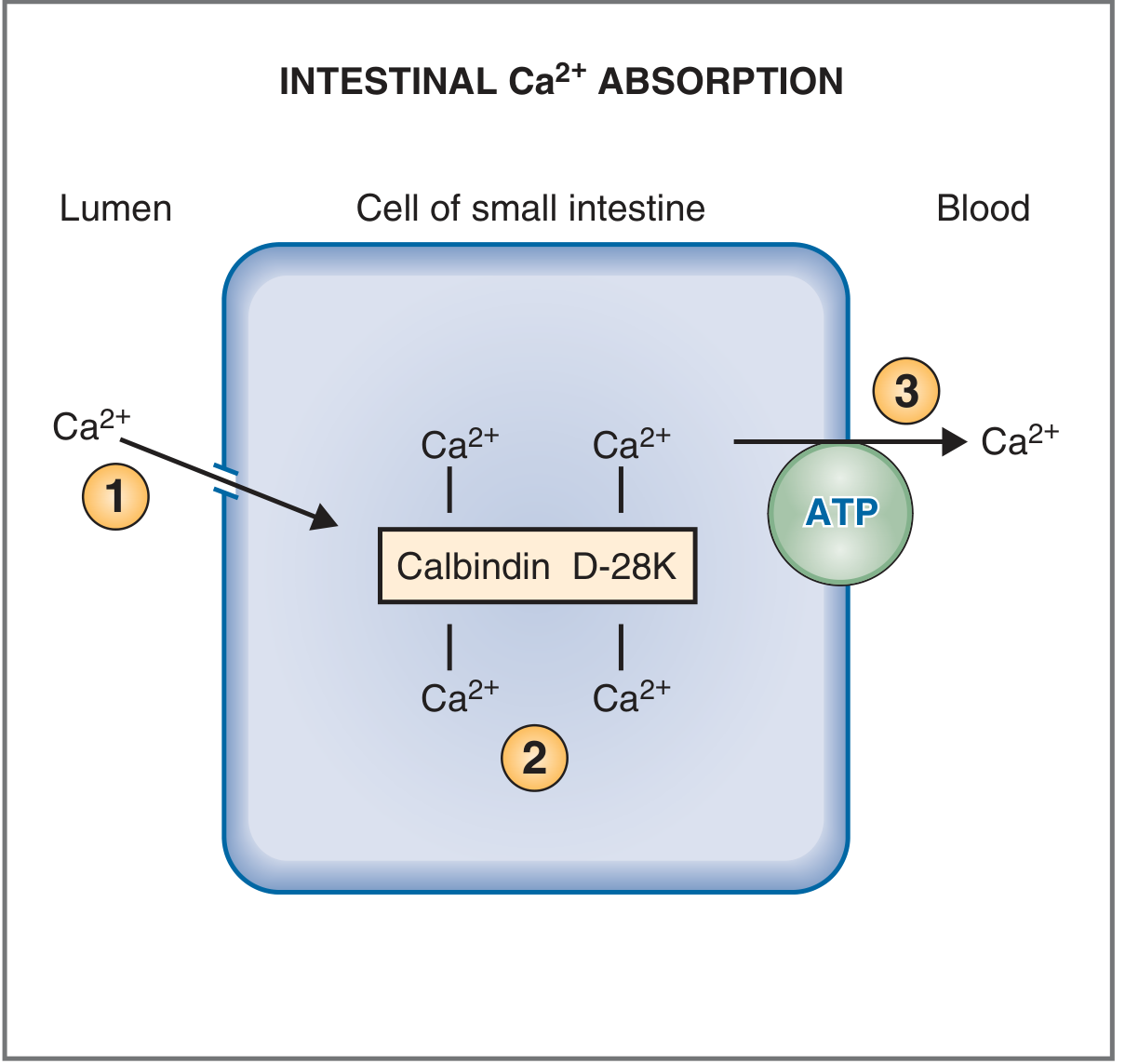
| Intestine | Indirect - via activation of Vitamin D | ↑ Intestinal Ca²⁺ absorption |
Note: The phosphaturic action of PTH is critical - without it, the phosphate released from bone would complex with ionized Ca²⁺ in ECF and blunt the rise in calcium.
B. Vitamin D (1,25-Dihydroxycholecalciferol / Calcitriol)
Skin (UV light)
Cholesterol → 7-dehydrocholesterol → Cholecalciferol (Vitamin D₃)
↓ (Liver)
25-Hydroxycholecalciferol
↓ (Kidney - 1α-hydroxylase)
↑ stimulated by PTH, low Ca²⁺, low PO₄
1,25-Dihydroxycholecalciferol (Calcitriol) ← ACTIVE FORM
| Target | Action |
|---|---|
| Intestine (main target) | Induces synthesis of calbindin D-28K → ↑ Ca²⁺ AND phosphate absorption |
| Kidney | Stimulates reabsorption of both Ca²⁺ and phosphate |
| Bone | Synergizes with PTH to stimulate osteoclast activity and bone resorption (to provide Ca²⁺/PO₄ for new bone mineralization) |
| Parathyroid glands | Directly inhibits PTH synthesis and secretion (negative feedback) |
C. Calcitonin
- Secreted by parafollicular C cells of the thyroid gland
- Stimulus: hypercalcemia (high plasma Ca²⁺)
- Mechanism: binds Gs-coupled receptor on osteoclasts → ↑ cAMP → inhibits osteoclast activity
| Action | Effect |
|---|---|
| Bone | Inhibits osteoclast activity → ↓ bone resorption → ↓ Ca²⁺ and PO₄ release |
| Kidney | ↓ Ca²⁺ reabsorption → ↑ urinary Ca²⁺ excretion |
Calcitonin is physiologically less important in adults than PTH/Vitamin D, but it plays a significant role in calcium regulation in children during active bone growth.
4. Effect of Acid-Base Disturbances on Ionized Ca²⁺
| Condition | Effect on Ionized Ca²⁺ | Clinical Result |
|---|---|---|
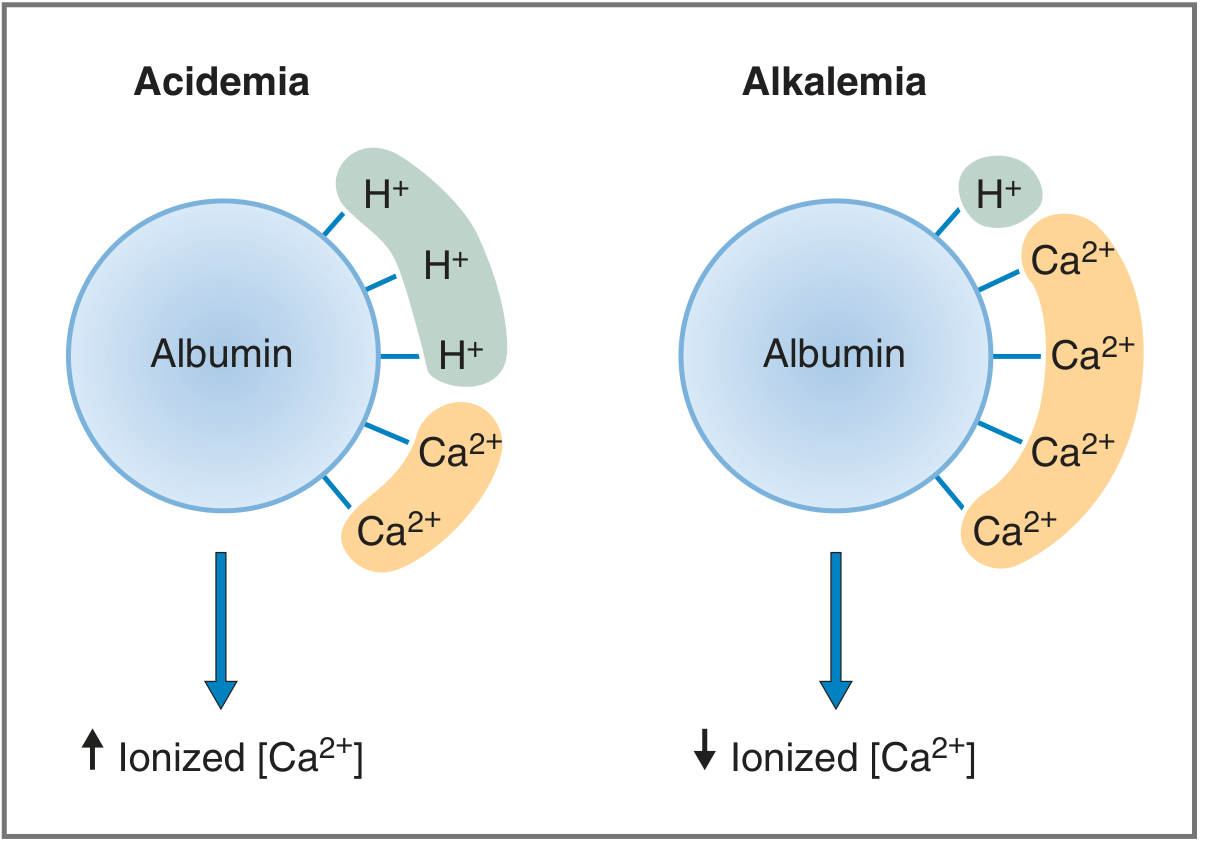
| Acidemia | H⁺ competes with Ca²⁺ for albumin → ↑ free ionized Ca²⁺ | Hypercalcemia symptoms |
| Alkalemia | Less H⁺ → Ca²⁺ binds albumin more → ↓ free ionized Ca²⁺ | Hypocalcemia symptoms (tetany, tingling) |
Clinically: Hyperventilation (acute respiratory alkalosis) causes tetany due to this mechanism even though total Ca²⁺ is normal.
5. Integrated Regulatory Summary
| Scenario | What Happens |
|---|---|
| Hypocalcemia | ↑ PTH secretion (within seconds) → ↑ bone resorption + ↑ renal Ca²⁺ reabsorption + ↑ 1,25-Vit D → ↑ gut absorption → Ca²⁺ restored |
| Hypercalcemia | ↓ PTH secretion + ↑ Calcitonin → ↓ bone resorption + ↓ renal Ca²⁺ reabsorption → Ca²⁺ lowered |
| Vitamin D deficiency | ↓ gut Ca²⁺ absorption → hypocalcemia → secondary ↑ PTH → rickets (children), osteomalacia (adults) |
| Primary hyperparathyroidism | PTH adenoma → excess PTH → hypercalcemia + hypophosphatemia + hypercalciuria → "stones, bones, groans" |
| Chronic renal failure | ↓ 1α-hydroxylase → ↓ active Vitamin D → hypocalcemia → secondary hyperparathyroidism |
6. Summary Table of the Three Hormones
| Property | PTH | Vitamin D (1,25-(OH)₂) | Calcitonin |
|---|---|---|---|
| Source | Parathyroid chief cells | Skin → Liver → Kidney | Thyroid C cells |
| Stimulus | ↓ Ca²⁺, ↓ Mg²⁺ | ↑ PTH, ↓ Ca²⁺, ↓ PO₄ | ↑ Ca²⁺ |
| Effect on serum Ca²⁺ | ↑↑ | ↑ | ↓ |
| Effect on serum PO₄ | ↓ | ↑ | ↓ |
| Effect on bone | ↑ Resorption | ↑ Resorption (synergy) | ↓ Resorption |
| Effect on kidney | ↑ Ca²⁺ reabsorption, ↓ PO₄ reabsorption | ↑ Ca²⁺ + PO₄ reabsorption | ↓ Ca²⁺ reabsorption |
| Effect on gut | Indirect (via Vit D) | ↑ Ca²⁺ + PO₄ absorption | None significant |
| Mechanism | cAMP (Gs protein) | Nuclear receptor (gene transcription) | cAMP (Gs protein) |