Discuss the clinical features, investigations, and management of a 40-year-old man presenting with acute Occlusion of Rt femoral artery
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
acute limb ischemia management revascularization
Reading File
Reading File
I now have comprehensive information from multiple authoritative surgical textbooks. Let me compile the full detailed answer:
Acute Occlusion of the Right Femoral Artery in a 40-Year-Old Man
Definition & Overview
Acute limb ischemia (ALI) is defined as a sudden loss of limb perfusion, applicable up to 2 weeks after an initiating event. It is a surgical emergency - irreversible muscle and nerve injury occurs after 6 hours of severe arterial insufficiency. Perioperative mortality rates of 20-40% and limb loss rates of 12-50% have been reported in lower extremity ALI.
In a 40-year-old man, the most likely cause is arterial embolism (from a cardiac source) or in-situ thrombosis on atherosclerotic plaque, though trauma and other causes must also be considered.
Etiology
The most common causes, in order of frequency:
| Cause | Notes |
|---|---|
| Arterial embolism | Heart is the source in >90% of peripheral emboli. Atrial fibrillation is the most common source; also mural thrombus over MI or LV aneurysm |
| In-situ thrombosis | Thrombosis on pre-existing atherosclerotic plaque or bypass graft occlusion |
| Trauma | Direct arterial injury, compartment syndrome |
| Aortic dissection | Extending into the femoral system |
| Popliteal aneurysm thrombosis | With distal embolization |
| Hypercoagulable state | Factor V Leiden, antiphospholipid syndrome, protein C/S deficiency |
Key distinction: Embolism vs. Thrombosis - Management differs significantly:
| Feature | Embolism | Thrombosis |
|---|---|---|
| Onset | Sudden, dramatic | More gradual |
| Prior claudication | Absent | Usually present |
| Contralateral pulses | Normal | Often reduced/absent |
| Atrial fibrillation/cardiac disease | Often present | Less common |
| Angiographic appearance | Sharp cutoff, meniscus sign | Irregular, collaterals present |
| Treatment of choice | Embolectomy (Fogarty) | Thrombolysis or bypass |
Clinical Features - The "Six Ps"
The classic presentation of ALI is summarized by the "Six Ps":
- Pain - Sudden, severe pain in the limb (earliest symptom); at rest, worsened by movement
- Pallor - The limb appears pale or mottled due to lack of perfusion; later becomes cyanotic/mottled
- Pulselessness - Absent femoral, popliteal, dorsalis pedis, and posterior tibial pulses distal to the occlusion; a palpable femoral pulse that disappears at the bifurcation localizes the embolus
- Paresthesia - Tingling and numbness; reflects ischemia of sensory nerve fibers (early ischemia sign)
- Paralysis - Motor weakness or complete loss of movement; indicates advanced ischemia of motor nerves and muscle
- Poikilothermia (Perishingly cold) - The limb is cold to touch, with a distinct temperature border indicating the level of occlusion
The presence of paresthesia and paralysis indicates threatened limb requiring immediate intervention.
Additional Findings
- Mottling (blue-red discoloration that blanches on pressure) - early; progresses to fixed staining (irreversible)
- Absent Doppler signals distally
- Signs of underlying cause: irregular pulse (AF), cardiac murmur, recent MI, or known peripheral vascular disease
Rutherford Classification (Severity Grading)
This is used to stratify urgency of intervention:
| Category | Description | Sensory Loss | Muscle Weakness | Arterial Doppler | Venous Doppler |
|---|---|---|---|---|---|
| I - Viable | Not immediately threatened | None | None | Audible | Audible |
| IIa - Marginally threatened | Salvageable if promptly treated | Minimal (toes) / none | None | Absent | Audible |
| IIb - Immediately threatened | Salvageable with immediate revascularization | More than toes, rest pain | Mild-moderate | Absent | Audible |
| III - Irreversible | Major tissue loss / permanent neurologic damage | Profound, anesthetic | Profound paralysis (rigor) | Absent | Absent |
Investigations
Immediate (Bedside)
- Continuous-wave Doppler of peripheral signals - assess level and severity; compare multiphasic vs. monophasic vs. absent signals with the contralateral limb
- Ankle-Brachial Index (ABI) - typically <0.3 in acute occlusion (normal >0.9)
- 12-lead ECG - detect atrial fibrillation, recent MI
- Pulse oximetry on the affected digit
Laboratory Tests
- Full blood count (CBC) - baseline, detect polycythemia
- Coagulation profile (PT, aPTT, INR, fibrinogen) - before thrombolysis
- Urea, creatinine, electrolytes - baseline renal function; critical for contrast use and monitoring reperfusion injury
- Serum lactate, CK (creatine kinase) - assess severity of muscle ischemia/necrosis
- Serum potassium - hyperkalemia from ischemic muscle
- Blood glucose, lipid profile - risk factor assessment
- Cardiac enzymes (Troponin) - if MI suspected as cause
- Hypercoagulable screen (antiphospholipid antibodies, protein C, protein S, factor V Leiden, antithrombin III) - especially important in a young patient; must be done before starting heparin if time permits
Imaging
- Duplex ultrasound (Doppler) - First-line non-invasive imaging; identifies site of occlusion, differentiates embolism from thrombosis, assesses collaterals. Rapid and bedside-available.
- CT Angiography (CTA) - Most widely used; rapid, non-invasive; excellent for defining anatomy, level of occlusion, inflow/outflow, and planning intervention. Preferred if arteriography is not immediately available.
- Conventional Catheter Arteriography - Gold standard; allows simultaneous diagnosis and therapeutic intervention (thrombolysis, angioplasty). Shows the meniscus sign (sharp cutoff) in embolism or irregular occlusion with collaterals in thrombosis. Arteriography is not mandatory if the clinical picture is clear, but all patients should be positioned for fluoroscopic access.
- MR Angiography - Alternative if contrast is contraindicated; less practical in emergency setting
- Echocardiography - To identify cardiac source (intracardiac thrombus, valvular disease, LV aneurysm); transoesophageal echo (TOE) is more sensitive
Management
Immediate (Emergency) Measures - "Do These Now"
- IV access + resuscitation - IV fluids, Foley catheter for urine output monitoring
- IV Heparin anticoagulation - Start immediately upon diagnosis; prevents thrombus propagation; unfractionated heparin bolus (80 U/kg) then infusion (18 U/kg/hr). If hypercoagulable workup needed, draw samples before heparin.
- Analgesia - IV opioids for pain
- Position - Keep the limb dependent (slightly below heart level) to improve perfusion; avoid pressure on the limb
- Protect the limb - Pad bony prominences; do not apply heat (increases metabolic demand in ischemic tissue)
- Oxygen supplementation
- Emergency vascular surgery referral
Definitive Treatment - Based on Rutherford Class
Class I (Viable) and IIa (Marginally Threatened)
- Catheter-directed thrombolysis (CDT) is preferred as first-line
- tPA (alteplase) or urokinase infused directly into the thrombus via catheter
- Advantages over surgery: reduced endothelial trauma, more gradual complete lysis including branch vessels too small for embolectomy catheters, potentially lower reperfusion injury
- Contraindications: recent stroke (<3 months), intracranial malignancy, brain surgery; relative contraindications include renal insufficiency, recent arterial puncture, coagulopathy, diabetic retinopathy, cardiac thrombus
- Percutaneous mechanical thrombectomy / thromboaspiration - Can be used as standalone or adjunct when thrombolysis is contraindicated; FDA-approved devices for acute lower extremity arterial thrombosis
Class IIb (Immediately Threatened)
- Emergency surgical revascularization (insufficient time for thrombolysis)
- Open embolectomy (if embolic etiology):
- Vertical groin incision exposing the common femoral artery (CFA) and its bifurcation
- The location of the embolus at the femoral bifurcation is often apparent by a palpable proximal femoral pulse disappearing distally
- A transverse arteriotomy over the bifurcation; Fogarty balloon catheter is passed to extract the thrombus
- 5Fr or 6Fr catheter proximally into the infrarenal aorta; 3-4Fr distally into SFA and profunda
- Good back-bleeding and antegrade bleeding confirm complete clot removal
- Embolic material sent for culture and histology
- Completion angiography to confirm adequate clot removal
- The femoral approach is preferred due to the larger artery diameter reducing risk of arterial compromise at arteriotomy closure
- Bypass surgery - For in-situ thrombosis on atherosclerotic disease or failed bypass graft (embolectomy catheters cannot traverse calcified occlusions); if there are good distal vessels and suitable saphenous vein, surgical bypass is fast and durable
Class III (Irreversible)
- Primary amputation - When limb is non-viable (profound paralysis with rigor, fixed staining)
- Attempting revascularization risks reperfusion syndrome - massive release of myoglobin, potassium, and toxic metabolites causing cardiac arrhythmia, acute renal failure, and death
Post-Revascularization Care
Reperfusion Injury & Compartment Syndrome
- After revascularization, ischemia-reperfusion releases oxygen free radicals, potassium, myoglobin, and lactate into circulation
- Monitor for compartment syndrome - pain on passive stretch, tense swollen compartments
- Fasciotomy of the 4 compartments of the leg should be performed prophylactically when ischemia time is >4-6 hours or there are signs of reperfusion injury
Systemic complications to monitor:
- Myoglobinuria / acute tubular necrosis - forced alkaline diuresis; monitor urine output >1 mL/kg/hr
- Hyperkalemia - cardiac monitoring, treat if K⁺ >6 mmol/L
- Metabolic acidosis - bicarbonate infusion
- Cardiac arrhythmias - especially if underlying AF
Long-term:
- Anticoagulation - Long-term warfarin (target INR 2-3) if embolic cause; direct oral anticoagulants if AF confirmed
- Treat underlying cause - Rate/rhythm control for AF, antiplatelet therapy for atherosclerosis
- Risk factor modification - Stop smoking, statin therapy, control hypertension/diabetes
- Surveillance imaging - Duplex ultrasound follow-up of revascularized segment
Summary Algorithm
Suspected Acute Femoral Artery Occlusion
↓
IV Heparin + Analgesia + Resuscitation
↓
Clinical Assessment (6 Ps) + Doppler
↓
Rutherford Classification
↓
┌────────────────────────────────┐
│ Class I / IIa │ → Imaging (CTA/arteriography) → Thrombolysis or Endovascular
│ Class IIb │ → Emergency Surgery (Embolectomy/Bypass)
│ Class III (Irreversible) │ → Amputation
└────────────────────────────────┘
↓
Post-op: Monitor for Compartment Syndrome, Reperfusion Injury
↓
Long-term anticoagulation + Treat underlying cause
Recent Evidence
Three recent systematic reviews (2025-2026) are relevant:
- Abuajamieh et al., J Vasc Surg 2026 (PMID: 41232816) - Compared endovascular vs. open surgery in ALI; meta-analysis of current data
- Cosarca et al., Medicina 2025 (PMID: 40428785) - Compared thrombolytic therapy vs. open surgical intervention; no clear superiority of either for 30-day limb salvage or mortality, consistent with prior RCT data
- Abouzid et al., Prog Cardiovasc Dis 2025 (PMID: 38981532) - Endovascular therapy vs. surgical revascularization for critical limb-threatening ischemia
These confirm the established textbook guidance that no single modality is universally superior - treatment choice must be individualized based on ischemia severity, anatomical factors, and patient fitness.
Sources: Sabiston Textbook of Surgery (20th ed.); Schwartz's Principles of Surgery (11th ed.); Current Surgical Therapy (14th ed.); Goldman-Cecil Medicine; Harrison's Principles of Internal Medicine (22nd ed.)
Dissecting aneurysm of aorta
Reading File
Finding Sources
Finding Sources
Searching PubMed
aortic dissection management guidelines
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive, authoritative content from Harrison's (22nd ed.), Braunwald's, Robbins, Sabiston, Schwartz, Grainger & Allison's Radiology, and Rosen's Emergency Medicine. Let me now compose the full detailed answer.
Dissecting Aneurysm of the Aorta (Aortic Dissection)
Definition
Aortic dissection occurs when the laminar planes of the media split apart, allowing blood under systemic pressure to track through the aortic wall and form a blood-filled false lumen - a channel within the aortic wall itself. This is the most common clinical emergency involving the aorta, with an estimated incidence of 3.5-16.3 cases per 100,000 patient-years.
Note: The term "dissecting aneurysm" is somewhat a misnomer since the aorta need not be aneurysmal for dissection to occur, but the term persists clinically.
Pathology
The intimal tear typically occurs in the ascending aorta within 10 cm of the aortic valve. Tears are usually transverse or oblique, 1-5 cm long, with sharp jagged edges. Once the tear occurs, blood dissects through the media along laminar planes, usually between the middle and outer thirds of the media.
The dissecting hematoma can:
- Extend distally - as far as the iliac and femoral arteries
- Extend retrogradely - toward the heart, causing AR, hemopericardium, tamponade
- Rupture externally through the adventitia - causing massive hemorrhage or cardiac tamponade
- Re-enter the true lumen distally through a second tear - creating a "double-barrelled" aorta
Pathology image (Robbins, Fig. 8.18) showing the dissection with intramural hematoma:
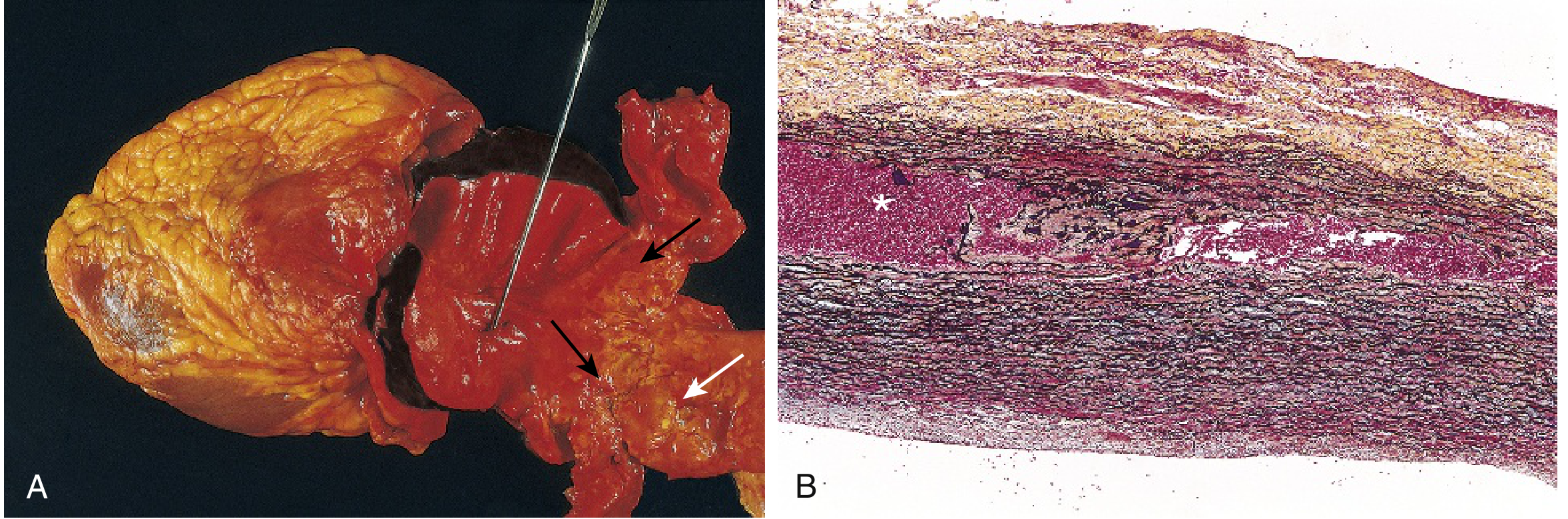
Panel A: Opened aorta showing proximal dissection with oblique intimal tear (probe). Black arrows mark the distal edge of intramural hematoma; the white arrow shows the adjacent atherosclerosis that arrested dissection. Panel B: Histologic Movat stain showing the dissection plane and intramural hematoma (asterisk).
Predisposing Conditions / Etiology
Primary Risk Factors
| Category | Conditions |
|---|---|
| Hypertension | Present in ~70% of cases; most common risk factor; narrowing of vasa vasorum with medial degeneration |
| Connective tissue disorders | Marfan syndrome (fibrillin-1 mutation - cystic medial necrosis), Ehlers-Danlos syndrome type IV, Loeys-Dietz syndrome |
| Congenital | Bicuspid aortic valve, coarctation of the aorta, Turner syndrome |
| Inflammatory | Takayasu arteritis, giant cell arteritis, syphilitic aortitis |
| Iatrogenic | Arterial cannulation, cardiopulmonary bypass, cardiac catheterization |
| Trauma | Deceleration injury, weightlifting |
| Drugs | Cocaine use (abrupt pressure surge); implicated in 0.5-37% of cases |
| Pregnancy | Third trimester; hormone-induced vascular remodeling + hemodynamic stress |
| Age/Sex | Peak incidence 6th-7th decade; men > women (2:1 overall) |
Dissection is unusual in the presence of heavy atherosclerosis because medial fibrosis inhibits propagation of the dissecting hematoma.
Classification
Stanford Classification (Clinically Most Useful)
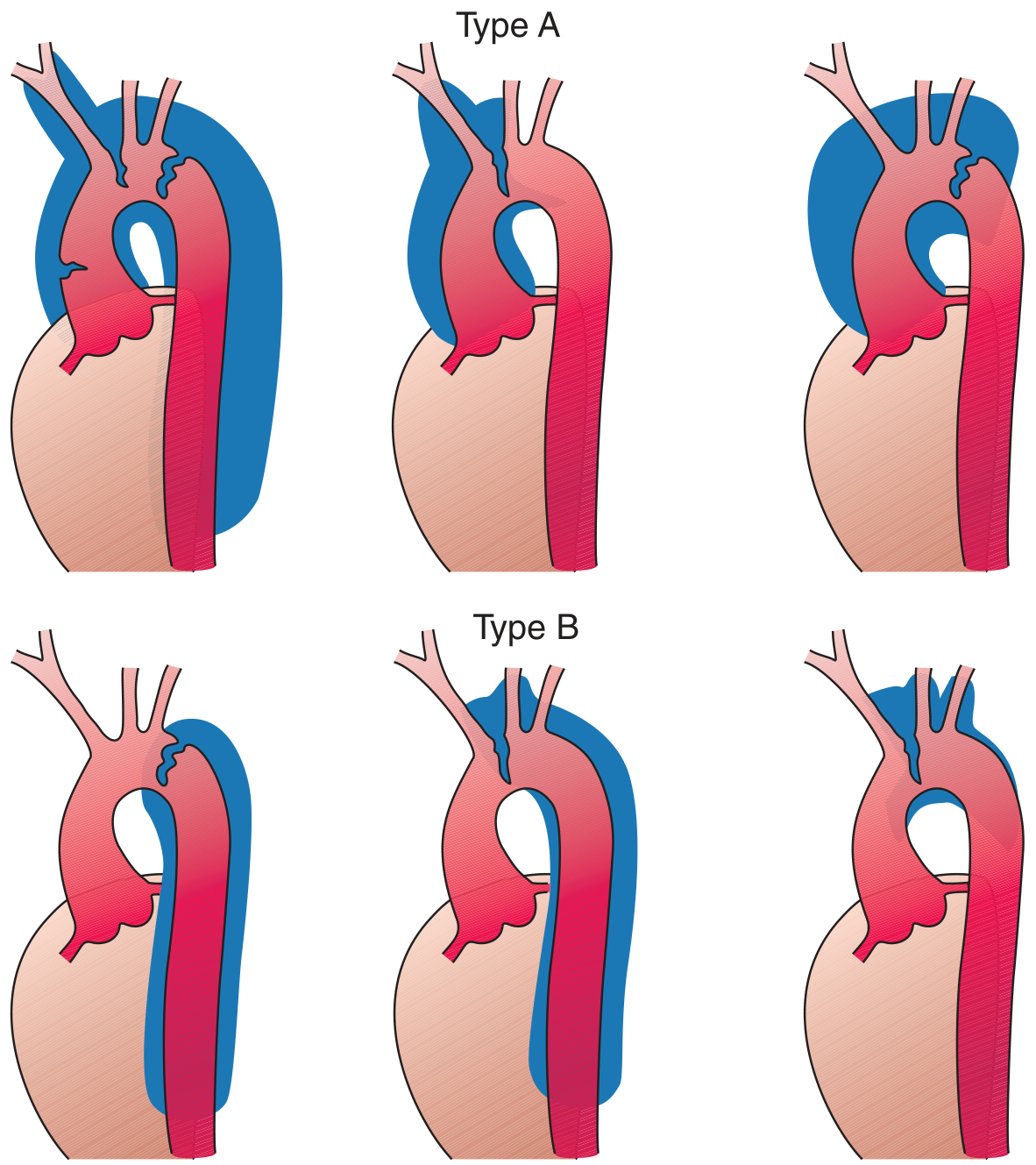
Top row: Stanford Type A (ascending aorta involvement - various extents). Bottom row: Stanford Type B (descending only, sparing the ascending aorta).
| Type | Definition | Frequency | Management |
|---|---|---|---|
| Type A | Any involvement of the ascending aorta (regardless of where the intimal tear is) | ~65-75% | Emergency surgery |
| Type B | Confined to the descending aorta distal to the left subclavian artery; no ascending involvement | ~25-35% | Medical therapy (surgery/TEVAR if complicated) |
DeBakey Classification
| Type | Description |
|---|---|
| Type I | Originates in ascending aorta, extends to arch and typically to descending (and beyond) |
| Type II | Confined to the ascending aorta only |
| Type III | Originates in the descending aorta (just distal to left subclavian); IIIa = thoracic only; IIIb = extends below diaphragm |
Types I and II = Stanford A; Type III = Stanford B.
Temporal Classification
| Phase | Time Frame |
|---|---|
| Hyperacute | <24 hours |
| Acute | 2-7 days |
| Subacute | 8-30 days |
| Chronic | >30 days |
Clinical Features
The presentation results from four mechanisms: the intimal tear itself, dissecting hematoma, occlusion of branch arteries, and compression of adjacent structures.
Cardinal Symptom: Pain
- Sudden onset, severe, tearing or ripping quality (described as the worst pain of their life)
- Associated with diaphoresis
- Location varies by type:
- Type A: Anterior chest, substernal
- Type B: Interscapular back pain, between the shoulder blades
- Pain characteristically migrates as the dissection propagates distally
Signs from Branch Vessel Occlusion
| Artery Involved | Clinical Manifestation |
|---|---|
| Coronary artery (usually right) | Acute MI (inferior STEMI pattern); occurs in <1-2% |
| Carotid arteries | Hemiplegia, hemianesthesia, stroke, syncope |
| Spinal arteries | Paraplegia (anterior spinal artery syndrome) |
| Renal arteries | Hematuria, oliguria, acute renal failure |
| Mesenteric arteries | Bowel ischemia, abdominal pain |
| Iliac/femoral arteries | Acute limb ischemia (absent pulses, cold limb) |
| Aortic root | Acute aortic regurgitation (>50% of Type A cases) |
Signs from Retrograde Dissection (Type A)
- Aortic regurgitation (AR) - present in >50% of Type A; bounding pulses, wide pulse pressure, diastolic murmur along right sternal border
- Hemopericardium / cardiac tamponade - pulsus paradoxus, hypotension, JVP elevation, muffled heart sounds (Beck's triad)
- Acute MI - if coronary ostium involved
Signs from Compression of Adjacent Structures
| Structure Compressed | Effect |
|---|---|
| Superior cervical ganglia | Horner's syndrome (ptosis, miosis, anhidrosis) |
| Superior vena cava | SVC syndrome |
| Left recurrent laryngeal nerve | Hoarseness |
| Esophagus | Dysphagia |
| Trachea/bronchus | Airway compromise, cough |
Blood Pressure Findings
- Hypertension is most common
- Hypotension - suggests tamponade, AR, or rupture; ominous sign
- Pulse deficit - absent or diminished pulse in one arm or leg (due to occlusion of the artery of origin)
- Blood pressure differential between arms (>20 mmHg) - highly suggestive
Investigations
Immediate Bedside
- Blood pressure in both arms - differential BP >20 mmHg is significant
- 12-lead ECG - critical to exclude acute MI; usually normal or shows LVH; inferior ST elevation if right coronary ostium involved
- Pulse oximetry, both limbs
- Chest auscultation - diastolic murmur of AR
Blood Tests
- FBC, urea, creatinine, electrolytes - baseline; renal involvement
- Cardiac troponin - may be elevated if coronary involvement; helps differentiate from MI (but does NOT exclude dissection)
- D-dimer - typically very elevated (>500 ng/mL) in acute dissection; a normal D-dimer has high negative predictive value to exclude dissection in low-risk patients
- Cross-match and group-and-save - for surgery preparation
- LFTs, amylase - if mesenteric involvement suspected
- Coagulation screen - disseminated intravascular coagulation possible
Chest X-Ray Findings
- Widened superior mediastinum (>8 cm or >25% of chest width) - most important sign; seen in ascending aortic dissections
- Abnormal aortic contour - loss of the aortic knuckle
- Pleural effusion (usually left-sided) - typically serosanguineous; not indicative of rupture unless accompanied by hypotension and falling Hct
- Tracheal/oesophageal deviation
- Normal in 10-20% of cases - cannot exclude dissection
Definitive Imaging
| Modality | Sensitivity | Specificity | Comments |
|---|---|---|---|
| CT Angiography | >90% | >90% | First-line investigation - rapid, widely available, excellent for whole aorta, extent, branch involvement; gold standard in emergency |
| Transesophageal Echocardiography (TOE/TEE) | 98% | ~90% | Excellent for ascending and descending thoracic aorta; does NOT visualize the arch well; also assesses AR, tamponade, LV function; can be bedside/ICU |
| MRI / MR Angiography | >90% | >90% | Most comprehensive; impractical in emergency (long scan time, unstable patients); best for chronic follow-up |
| Transthoracic Echocardiography (TTE) | 60-85% | Moderate | Quick and non-invasive; sensitivity for ascending aorta >80%; poor for descending aorta; cannot exclude dissection |
| Catheter Aortography | High | High | Was once gold standard; now rarely used as invasive when CT/MRI are available |
CT Angiography findings:
- Double-barrelled aortic lumen with intimal flap
- True lumen (smaller, high density) vs false lumen (larger, lower attenuation)
- Extent of dissection, involvement of branch vessels
- Pleural/pericardial effusion, mediastinal hematoma
Echo findings (diagnostic criteria):
- Dilated aortic lumen
- Linear, mobile echogenic structure (intimal flap) with motion different from aortic wall
- Different color Doppler flow patterns in true vs false lumen
- AR severity, pericardial effusion
Management
Immediate Resuscitation (All Types)
- Admit to ICU for continuous hemodynamic monitoring (arterial line, central line, Foley catheter)
- IV access - large bore, two sites
- Analgesia - IV morphine/opioids (reduces sympathetic drive)
- Blood pressure control - the cornerstone of initial medical therapy
- Oxygen supplementation
- Cross-match blood, alert cardiothoracic surgery immediately
- NPO (nothing by mouth) - anticipate surgery
Blood Pressure and Heart Rate Control
The immediate goal is to reduce dP/dt (rate of pressure rise), which is the shear force that propagates the dissection.
Target: Heart rate <60-80 bpm and systolic BP <120 mmHg (Rosen's: SBP <110 mmHg)
Step 1 - IV Beta-blocker FIRST (before any vasodilator):
- Esmolol (preferred - short-acting, titratable): Bolus 500 mcg/kg IV, then infusion 0.05-0.2 mg/kg/min
- Metoprolol IV: 5 mg q5 min, up to 15 mg
- Propranolol IV: 1 mg q3-5 min
- Labetalol (alpha + beta blocker): 20 mg IV bolus q10 min; long half-life of 4-6 hours makes it less titratable but acceptable
Rationale: Beta-blockers MUST precede vasodilators. Vasodilators given first cause reflex tachycardia, which WORSENS dP/dt and propagates the dissection.
Step 2 - Vasodilator if BP still elevated after achieving HR target:
- Sodium nitroprusside: highly titratable, rapid-acting; infusion 0.5-10 mcg/kg/min
- Nicardipine or clevidipine (calcium channel blockers): alternatives if beta-blockers contraindicated
- Diltiazem/Verapamil: IV mixed calcium channel blockers if neither beta-blockers nor nitroprusside can be used
Contraindicated: Hydralazine, other direct vasodilators as monotherapy - increase hydraulic shear and heart rate, propagating dissection.
Type A (Ascending) Dissection - EMERGENCY SURGERY
Indication: All Type A dissections require immediate surgical repair (>50% mortality within 48 hours if untreated from causes such as aortic rupture, cardiac tamponade, acute AR, MI).
Surgical Procedure:
- Excision of the intimal flap at the site of entry tear
- Obliteration of the false lumen
- Interposition graft placement (Dacron tube graft)
- If aortic valve disrupted: Aortic valve repair or composite valve-graft replacement (Bentall procedure with aortic root replacement)
- Reimplantation of coronary arteries if root involved
Surgical Mortality: ~15-25% in-hospital; Complications include MI, paraplegia, renal failure, hemorrhage, tamponade, sepsis.
Type B (Descending) Dissection - Complication-Driven Approach
Uncomplicated Type B
- Medical therapy alone - initial treatment of choice
- BP and HR targets as above, continued parenterally then converted to oral therapy
- In-hospital mortality: ~12%
- Close monitoring for complications
Complicated Type B - TEVAR or Surgery
Complications requiring intervention:
- Persistent/refractory pain (suggests propagation)
- Uncontrolled hypertension despite maximal medical therapy
- Progression of dissection (expansion)
- Branch vessel ischemia (bowel, renal, limb)
- Impending or frank rupture
- Rapid aortic expansion (>10 mm/year or diameter >6 cm)
Thoracic Endovascular Aortic Repair (TEVAR):
- First-line for complicated Type B (preferred over open surgery)
- Stent graft covers the entry tear, seals the false lumen, promotes false lumen thrombosis
- Reduces morbidity/mortality significantly vs open surgery (open surgery for Type B: mortality >50%)
- Dynamic obstruction (true lumen collapse): TEVAR restores true lumen
- Static obstruction of branch vessels: Direct stenting of the compromised vessel
- Intimal flap fenestration: Creates communication between true and false lumen
Open surgery for Type B: Reserved when TEVAR is not feasible; hybrid (combined endovascular + surgical) approaches for arch + descending involvement.
Note for Marfan syndrome: Early surgery is recommended for both Type A and B given the high risk for postdissection complications.
Long-Term Management (All Types)
- Antihypertensive therapy: Lifelong; beta-blockers + ACE inhibitors/ARBs + calcium antagonists; target BP <120/80 mmHg
- Risk factor control: Smoking cessation, lipid management, glycaemic control
- Imaging surveillance: Follow-up CT/MRI at 1 month, 6 months, 12 months, then annually; monitor for aneurysmal expansion of false lumen (20-50% of Type B patients develop aneurysmal dilatation within 1-5 years)
- Activity restriction: Avoid strenuous isometric exercise, weightlifting
- Genetic counselling: If connective tissue disorder suspected (Marfan, Loeys-Dietz, Ehlers-Danlos)
Prognosis: 10-year survival ~60% with adequate follow-up and medical management.
Acute Aortic Syndrome Spectrum
Aortic dissection is part of the broader "Acute Aortic Syndrome" which includes:
| Condition | Description |
|---|---|
| Classic aortic dissection | Intimal tear with propagating false lumen |
| Intramural hematoma (IMH) | Rupture of vasa vasorum → hemorrhage into media WITHOUT intimal tear; managed like dissection by type |
| Penetrating atherosclerotic ulcer (PAU) | Erosion of atherosclerotic plaque through internal elastic lamina into media; usually in descending thoracic aorta; may progress to IMH or dissection |
Key Differentiating Points vs. Acute MI
| Feature | Aortic Dissection | Acute MI |
|---|---|---|
| Pain quality | Tearing/ripping, maximal at onset | Pressure/crushing, builds up |
| Pain location | Chest + back (migratory) | Chest ± radiation to arm/jaw |
| BP | Often hypertensive; arm differential | Variable |
| Pulse deficit | Present (in some) | Absent |
| ECG | Usually normal or LVH | ST changes, new LBBB |
| Chest X-ray | Widened mediastinum | Normal or pulmonary oedema |
| Troponin | Usually normal (elevated only if coronary involved) | Elevated |
Critical: Do NOT give thrombolytics if aortic dissection is suspected - it is catastrophic and causes massive haemorrhage.
Summary: Management Algorithm
Suspected Aortic Dissection
↓
IV Analgesia + IV Beta-blocker → Target HR <60-80 bpm
↓
Add vasodilator → Target SBP <120 mmHg
↓
CT Angiography (urgent)
↓
┌─────────────────────┐
│ TYPE A │ → Emergency cardiothoracic surgery
│ (Ascending involved)│
├─────────────────────┤
│ TYPE B (Descending) │
│ - Uncomplicated │ → Medical therapy + ICU monitoring
│ - Complicated │ → TEVAR (or open surgery if TEVAR not feasible)
└─────────────────────┘
↓
Long-term: Antihypertensives + Annual imaging surveillance
Recent Guidelines (2024-2026)
Three major guidelines are currently in force:
- 2022 ACC/AHA Guideline for aortic disease (PMID: 37389507) - comprehensive North American guidance
- 2024 ESC Guidelines for peripheral arterial and aortic diseases (PMID: 39210722) - European standard of care
- 2026 ESVS Guidelines on descending thoracic and thoraco-abdominal aortic diseases (PMID: 41448425) - the most recent, published February 2026
All three guidelines support the general principle that Type A dissection requires emergency surgery, uncomplicated Type B is treated medically, and complicated Type B is best managed with TEVAR.
Sources: Harrison's Principles of Internal Medicine (22nd ed., 2025); Sabiston Textbook of Surgery (20th ed.); Schwartz's Principles of Surgery (11th ed.); Robbins & Kumar Basic Pathology; Braunwald's Heart Disease (12th ed.); Grainger & Allison's Diagnostic Radiology; Textbook of Clinical Echocardiography; Rosen's Emergency Medicine; Current Surgical Therapy (14th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.