Osteoarthritis
Reading File
Finding Sources
Searching PubMed
"osteoarthritis"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have excellent, comprehensive content to write a thorough answer. Let me compile everything.
Osteoarthritis (OA)
Definition
Osteoarthritis is characterized by failed repair of synovial joint tissues after intra-articular stress. The resulting breakdown of cartilage and bone leads to symptoms of pain, stiffness, and functional disability. Although the name implies inflammation, it is primarily a degenerative disorder, with inflammation acting as a secondary contributor. - Goldman-Cecil Medicine, Ch. 241
Epidemiology
- Affects >500 million people worldwide; women are disproportionately affected
- The incidence increases rapidly between ages 50-75; ~40% of people >70 are affected
- An estimated 25% of the U.S. adult population will have physician-diagnosed OA by 2040
- OA is the 15th highest cause of years lived with disability worldwide
- Lifetime risk of symptomatic knee OA: ~40% in men, ~47% in women; rises to ~60% in persons above a healthy weight
- Knee OA accounts for ~85% of the total burden of OA
Goldman-Cecil Medicine, Ch. 241
Classification
| Type | Features |
|---|---|
| Primary (idiopathic) | Appears without identifiable cause; associated with aging; oligoarticular; affects weight-bearing joints |
| Secondary | Occurs in younger individuals; predisposing causes include prior joint injury, deformity, diabetes, or obesity (~5% of cases) |
Pathogenesis
Stages of Joint Damage
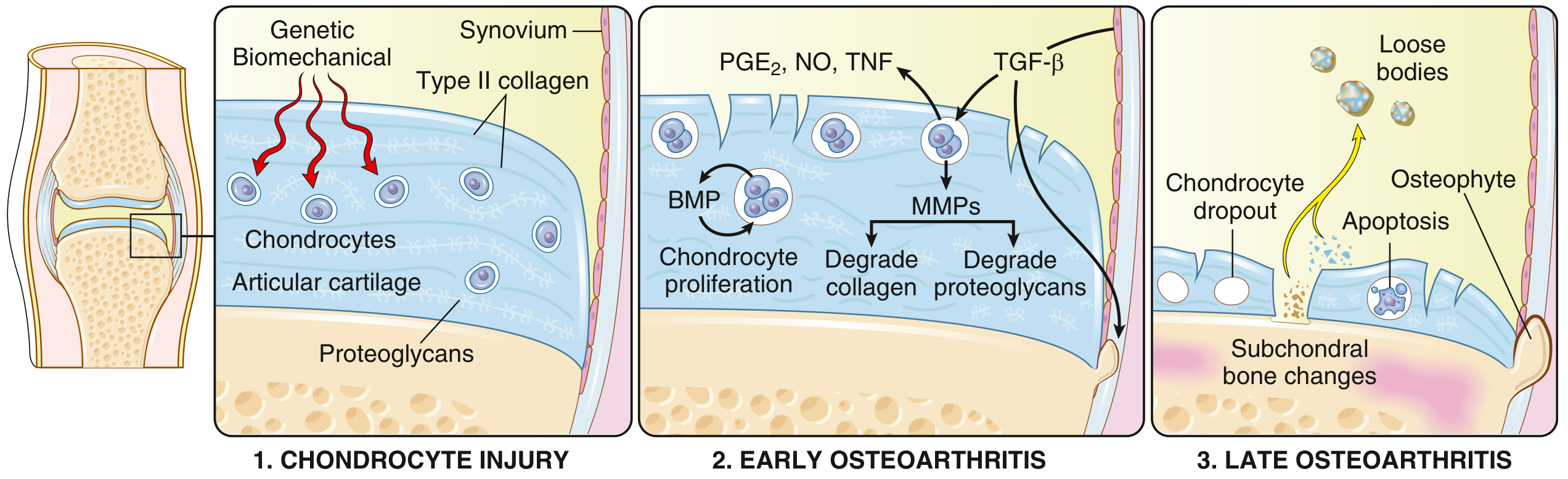
Fig. 19.31 - Robbins & Kumar Basic Pathology: Progression from chondrocyte injury (stage 1) to early OA (stage 2) to late OA (stage 3)
1. Chondrocyte injury - Genetic and biomechanical stresses injure chondrocytes, triggering changes in the extracellular matrix (Type II collagen and proteoglycans disrupted)
2. Early OA - Hypertrophic chondrocytes proliferate and attempt repair, but simultaneously release:
- Matrix metalloproteinases (MMPs) - degrade collagen and proteoglycans
- Proinflammatory mediators: PGE₂, NO, TNF
- TGF-β drives some compensatory repair (BMP signaling)
- Degradation eventually exceeds repair
3. Late OA - Chondrocyte dropout via apoptosis, full-thickness cartilage loss, subchondral bone changes, osteophyte formation, and loose bodies
Robbins & Kumar Basic Pathology, p. 790
Mechanics vs. Inflammation
Mechanical load is the primary driver when:
- Excessive strain is placed on a normal joint (obesity, occupational overuse, malalignment)
- Normal load traverses a joint that has lost mechanical protection (ligament rupture, meniscal damage, muscle weakness)
This altered mechanical load then activates inflammatory signaling pathways, which drive cartilage breakdown. Systemic obesity-related inflammation further amplifies the process. - Goldman-Cecil Medicine, Ch. 241
Morphology (Gross and Histologic)
Histology (early): Fibrillation (fraying) of the articular cartilage surface is the earliest change
Advanced disease:
- Full-thickness cartilage sloughing
- Loose bodies ("joint mice") - dislodged cartilage and bone fragments
- Bone eburnation - exposed subchondral bone polished by friction (ivory appearance)
- Subchondral cysts - synovial fluid forced into bone via ball-valve mechanism through fracture gaps
- Osteophytes - bony outgrowths capped by fibrocartilage at joint margins
- Synovium: mildly congested, fibrotic, with scattered chronic inflammatory cells
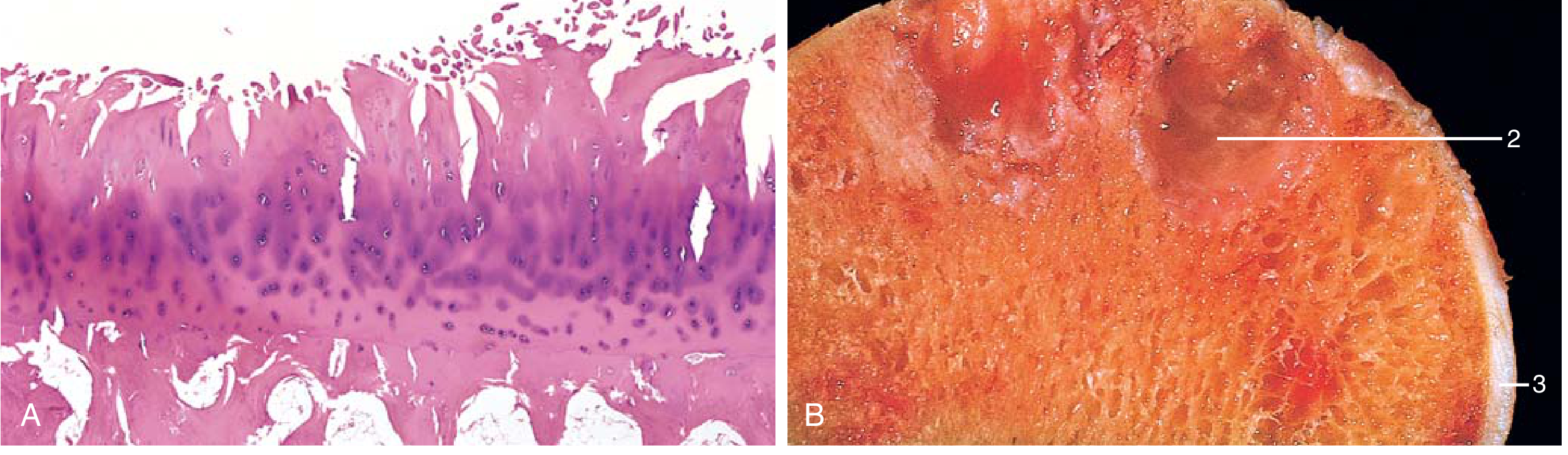
Fig. 19.32 - Robbins & Kumar: (A) Fibrillation of articular cartilage on histology; (B) Gross specimen showing eburnated surface (1), subchondral cyst (2), and residual cartilage (3)
Risk Factors
| Modifiable | Non-modifiable |
|---|---|
| Obesity (BMI - causative via Mendelian randomization) | Age |
| Joint malalignment | Sex (female > male) |
| Muscle weakness | Genetics (>80 OA loci identified in GWAS) |
| Sedentary lifestyle | Prior joint injury |
| Occupational exposure | Ethnicity |
| Athletic injuries |
Key genetic loci include GDF5 (chromosome 20), RUNX2, SMAD3, and PTHLH - genes important in skeletal and bone development. - Firestein & Kelley's Textbook of Rheumatology
OA vs. Rheumatoid Arthritis (Key Comparison)
| Feature | Osteoarthritis | Rheumatoid Arthritis |
|---|---|---|
| Primary mechanism | Mechanical injury to cartilage | Autoimmunity |
| Inflammation | Secondary; exacerbates damage | Primary cause of destruction |
| Joints involved | Weight-bearing (knees, hips); DIP/PIP/CMC | Small joints of fingers first; then multiple joints |
| Pathology | Cartilage degeneration, bone spurs, subchondral cysts; minimal inflammation | Inflammatory pannus; severe chronic inflammation; ankylosis |
| Serology | Negative (no ACPA, RF) | ACPA, rheumatoid factor positive |
| Extra-articular | None | Lungs, heart, other organs |
Robbins & Kumar Basic Pathology, Table 19.2
Clinical Features
Symptoms:
- Pain - mechanical in nature; worse with activity, better at rest; worse toward end of day; at rest in advanced disease
- Morning stiffness - localized, lasts <30 minutes (distinguishes from RA, which is >1 hour)
- Crepitus - audible and palpable during joint movement
- Functional limitation - difficulty with stairs/rising (knee), opening jars (hand), putting on shoes (hip)
- Catching or locking - especially knee (associated with falls)
Signs:
- Tenderness along joint line
- Bony swelling (osteophytes) + soft tissue swelling (effusion)
- Reduced range of motion
- Heberden nodes - osteophytes at DIP joints (more common in women)
- Bouchard nodes - osteophytes at PIP joints
- Knee: varus deformity, fixed flexion, ligamentous instability
- Hip: early loss of internal rotation
Joints most commonly affected: Hips, knees, lower lumbar and cervical vertebrae, PIP and DIP joints of fingers, first carpometacarpal joints, first tarsometatarsal joints
Spinal involvement: Osteophyte impingement on spinal foramina causes cervical/lumbar nerve root compression, radicular pain, muscle spasms, neurologic deficits
Diagnosis
Diagnosis is clinical based on:
- Symptoms: pain, brief morning stiffness, functional limitation
- Examination: crepitus, restricted/painful movement, joint tenderness, bony enlargement
Investigations:
- Plain radiographs: not required for typical presentations; useful for atypical cases
- Shows: asymmetric joint space narrowing, osteophytes, subchondral cysts, subchondral sclerosis
- Note: radiographic severity correlates poorly with symptoms
- Laboratory tests: limited role; mainly to exclude alternatives (infection, crystal arthropathy, RA)
- Synovial fluid: mildly inflammatory, low WBC (<2000 cells/µL), few PMNs
Red flags suggesting alternative diagnosis:
- Prolonged morning stiffness (>1 hr) → RA
- Hot, swollen joint → crystal disease (gout/pseudogout) or septic arthritis
- Recent trauma
Goldman-Cecil Medicine, Ch. 241; Rosen's Emergency Medicine
Management
Management should be individually tailored and focus on core treatments.
Non-Pharmacologic (First-Line)
- Exercise (land and water-based) - most evidence-based intervention; reduces pain and improves function
- Weight loss - BMI reduction relieves joint load; particularly effective for knee/hip OA
- Self-management education - activity modification, pacing
- Physical/occupational therapy - strengthening, gait aids, assistive devices
- Orthoses/bracing - appropriate footwear, splints, knee braces for malalignment
- TENS, acupuncture - limited but some evidence for pain relief
Pharmacologic
| Drug | Notes |
|---|---|
| Acetaminophen (paracetamol) | First-line; best safety profile; recent data suggest minimal benefit as monotherapy in knee OA |
| Topical NSAIDs (diclofenac gel) | Similar efficacy to oral NSAIDs; lower GI risk; preferred in elderly/high GI-risk patients |
| Oral NSAIDs | More effective than acetaminophen for pain; use when acetaminophen fails; risk: GI bleed, renal impairment, CV events |
| COX-2 inhibitors | Lower GI bleeding risk than non-selective NSAIDs; residual CV risk with long-term use |
| Duloxetine | Centrally-acting SNRI; effective for chronic musculoskeletal pain/knee OA; initiated in outpatient setting |
| Topical capsaicin | Useful for small hand joints; systemic toxicity low; significant local skin reaction limits use |
| Intra-articular corticosteroids | For acute flares; pain relief for weeks; unpredictable; no long-term benefit; may worsen arthritis with repeated use |
| Intra-articular hyaluronic acid | Best studied in knee; may improve function; no strong long-term benefit |
| Tramadol/Opioids | Not recommended; risks outweigh benefits for long-term OA management |
| Glucosamine/chondroitin | Supplements with limited demonstrated benefit |
Rosen's Emergency Medicine; Goldman-Cecil Medicine, Ch. 241
Surgical
- Joint replacement (arthroplasty) - indicated when:
- Functional status interferes with activities of daily living
- Supportive care and other measures have failed
- Pain is severe and persistent
- Knee replacement and hip replacement are among the most successful surgical procedures in medicine
Prognosis
- Natural history is highly variable; usually evolves over decades
- Progressive disease punctuated by periods of increased activity
- 80% of affected individuals have movement limitations
- 25% have difficulty with major activities of daily living
- No disease-modifying treatment currently exists - all current therapies are symptomatic
- Joint fusion (ankylosis) does NOT occur (distinguishing OA from RA)
Sources: Robbins & Kumar Basic Pathology, p. 789-791 | Goldman-Cecil Medicine, Ch. 241 | Rosen's Emergency Medicine, Ch. 102 | Firestein & Kelley's Textbook of Rheumatology
This is a shared conversation. Sign in to Orris to start your own chat.