Explain cardiac cycle for 15 mark question in university mbbs exam
The Cardiac Cycle
Definition
- Guyton and Hall Textbook of Medical Physiology, p. 9.8
- Costanzo Physiology 7th Edition, p. 160
Initiation
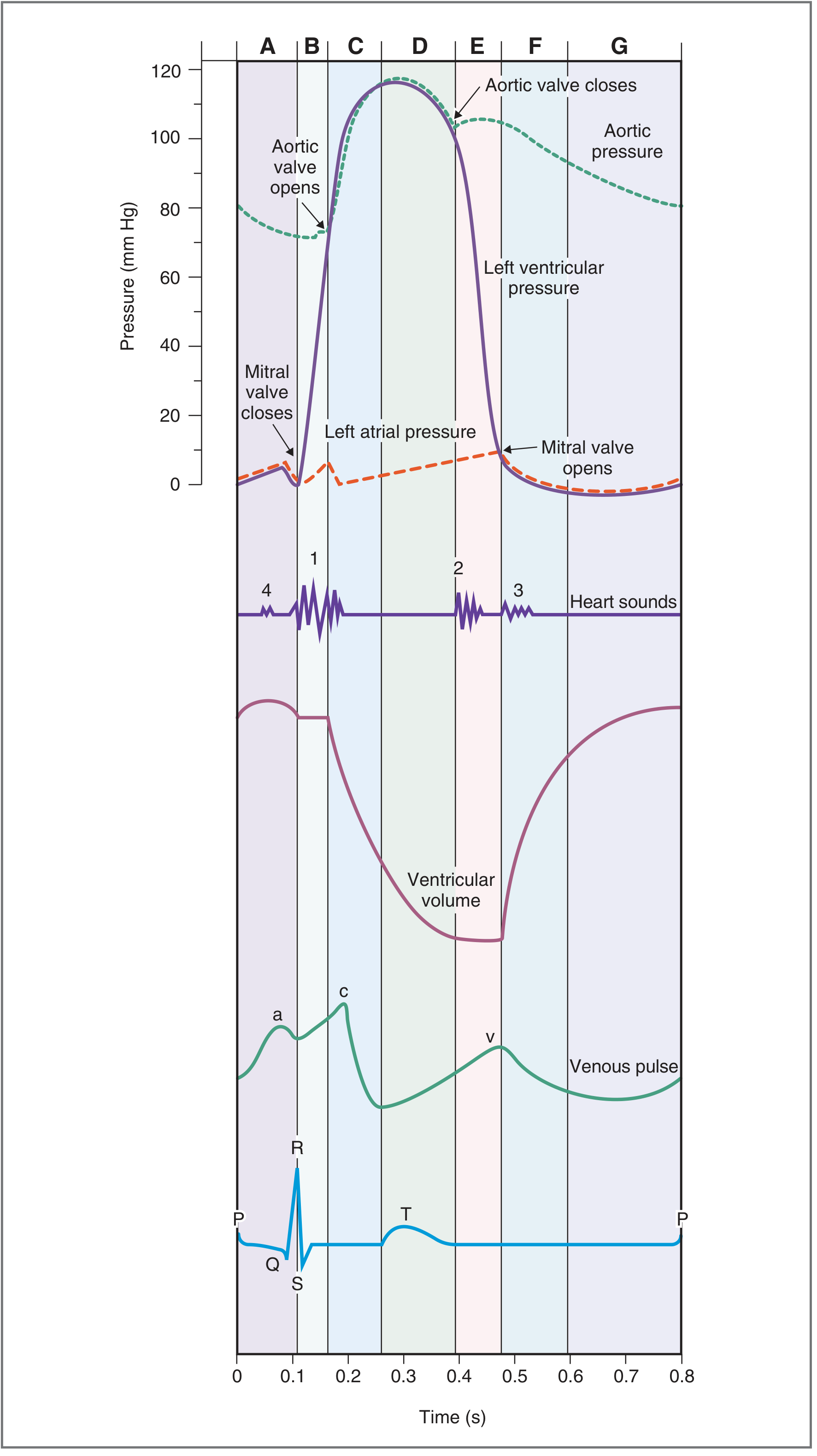
Wiggers Diagram (The Cardiac Cycle Diagram)
Seven Phases of the Cardiac Cycle
Phase A - Atrial Systole
- ECG: P wave (atrial depolarization), then PR interval
- Events: Atria contract. The mitral valve is already open (from previous diastole), so 70% of ventricular filling has already occurred passively. Atrial systole contributes the final 30% of ventricular filling by actively pumping blood into the ventricle.
- Pressures: Left atrial pressure rises slightly; this rise is transmitted back into the great veins and appears as the "a" wave on the jugular venous pulse (JVP).
- Valves: Mitral valve open, aortic valve closed
- Heart Sound: S4 (fourth heart sound) - not audible in normal adults; heard in conditions of reduced ventricular compliance (e.g., left ventricular hypertrophy)
- Ventricular volume: At end of atrial systole = End-Diastolic Volume (EDV) ~130 mL
Phase B - Isovolumetric Ventricular Contraction (IVC)
- ECG: QRS complex (ventricular depolarization)
- Events: Ventricles begin to contract. As ventricular pressure rises above atrial pressure, the mitral (and tricuspid) valves close. Ventricular pressure continues to rise but the aortic valve is not yet open (aortic pressure is ~80 mmHg). ALL valves are closed, so ventricular volume remains constant - hence "isovolumetric."
- Duration: ~0.05 seconds
- Pressures: Left ventricular pressure rises steeply from near 0 to 80 mmHg. The bulging of AV valves into the atria causes a small sharp rise in atrial pressure - the "c" wave on JVP.
- Valves: All valves closed (mitral just closed, aortic not yet open)
- Heart Sound: S1 ("lub") - caused by closure of mitral and tricuspid valves
- Ventricular volume: Constant at 130 mL (EDV)
Phase C - Rapid Ventricular Ejection
- ECG: ST segment
- Events: When left ventricular pressure exceeds aortic pressure (~80 mmHg), the aortic valve opens and ejection begins. Blood is rapidly expelled into the aorta. Ventricular pressure continues to rise, reaching its peak of ~120 mmHg.
- Pressures: Aortic pressure rises from 80 mmHg to ~120 mmHg (systolic). Ventricular pressure mirrors aortic pressure.
- Valves: Aortic valve open, mitral valve closed
- Heart Sound: None
- Ventricular volume: Rapidly decreasing
Phase D - Reduced Ventricular Ejection
- ECG: T wave (ventricular repolarization)
- Events: Ejection continues but at a slower rate. Ventricular pressure begins to fall. Aortic pressure also begins to fall as blood runs off into peripheral vessels. Late in this phase, aortic pressure briefly exceeds left ventricular pressure, but blood continues forward due to momentum.
- Valves: Aortic valve still open
- Heart Sound: None
- Ventricular volume: Reaches minimum = End-Systolic Volume (ESV) ~50-60 mL
Key Values:
- Stroke Volume (SV) = EDV - ESV = 130 - 50 = ~70-80 mL
- Ejection Fraction (EF) = SV/EDV = 70/130 = ~65% (normal >55%)
Phase E - Isovolumetric Ventricular Relaxation (IVR)
- ECG: After T wave (electrically silent)
- Events: Ventricular muscle relaxes. Ventricular pressure falls sharply. When ventricular pressure drops below aortic pressure, the aortic valve closes. A brief period called protodiastole (~0.04 s) precedes valve closure, during which momentum keeps blood flowing. All valves are again closed, so ventricular volume is constant.
- Duration: ~0.06-0.08 seconds
- Pressures: Left ventricular pressure falls steeply from ~80 mmHg toward 0. The dicrotic notch (incisura) appears on the aortic pressure trace at the moment of aortic valve closure, due to vibrations set up in the blood vessel wall.
- Valves: All valves closed (aortic just closed, mitral not yet open)
- Heart Sound: S2 ("dub") - caused by closure of aortic and pulmonary valves
- Ventricular volume: Constant at ESV (~50-60 mL)
Phase F - Rapid Ventricular Filling
- ECG: Electrically silent (between T wave and next P wave)
- Events: When left ventricular pressure falls below left atrial pressure, the mitral valve opens. Blood rushes rapidly from atrium into ventricle. During this phase, atrial pressure has been rising (blood continuously arriving from pulmonary veins during systole), creating the "v" wave on JVP. When the mitral valve opens, the v wave collapses as blood flows into the ventricle.
- Pressures: Ventricular pressure is low and remains nearly constant despite increasing volume (compliant ventricle).
- Valves: Mitral valve open
- Heart Sound: S3 (third heart sound) - may be audible in normal children/young adults; in adults >40 years, suggests ventricular failure (pathological S3)
- Ventricular volume: Rapidly increasing
Phase G - Reduced Ventricular Filling (Diastasis)
- ECG: Isoelectric, before next P wave
- Events: The rate of ventricular filling slows down as the pressure gradient between atrium and ventricle equalizes. This phase of slow filling is called diastasis. Approximately 70% of ventricular filling occurs passively during phases F and G combined.
- Valves: Mitral valve remains open
- Heart Sound: None
- Ventricular volume: Slowly increasing toward EDV
Summary Table of the Seven Phases
| Phase | Name | ECG | Key Valve Event | Heart Sound | Volume |
|---|---|---|---|---|---|
| A | Atrial Systole | P wave | -- | S4 (abnormal) | EDV reached |
| B | Isovolumetric Ventricular Contraction | QRS | Mitral closes | S1 | Constant (130 mL) |
| C | Rapid Ventricular Ejection | ST segment | Aortic opens | -- | Decreasing |
| D | Reduced Ventricular Ejection | T wave | -- | -- | ESV reached (~50 mL) |
| E | Isovolumetric Ventricular Relaxation | Silent | Aortic closes | S2 | Constant (50 mL) |
| F | Rapid Ventricular Filling | Silent | Mitral opens | S3 (abnormal in adults) | Increasing |
| G | Diastasis | Silent | -- | -- | Slowly increasing |
Pressure-Volume (P-V) Loop
- d → a: Diastolic filling (volume increases, pressure rises slightly)
- a → b: Isovolumetric contraction (pressure rises sharply, volume constant)
- b → c: Ventricular ejection (pressure rises then falls, volume decreases)
- c → d: Isovolumetric relaxation (pressure falls, volume constant)
- Ganong's Review of Medical Physiology, 26th Edition, Figure 30-2
Jugular Venous Pulse (JVP) Waves During the Cardiac Cycle
| Wave | Cause | Phase |
|---|---|---|
| a wave | Atrial contraction | Phase A |
| c wave | Bulging of tricuspid valve into atrium during IVC | Phase B |
| x descent | Atrial relaxation + downward displacement of AV valves during ejection | Phases C-D |
| v wave | Atrial filling while tricuspid valve is closed | Phases C-D-E |
| y descent | Tricuspid valve opens, blood flows into ventricle | Phase F |
Effect of Heart Rate on the Cardiac Cycle
| Heart Rate | Cycle Duration | Systole | Diastole |
|---|---|---|---|
| 75/min | 0.80 s | 0.27 s | 0.53 s |
| 200/min | 0.30 s | 0.16 s | 0.14 s |
Right vs. Left Heart
- Left ventricle - peak systolic pressure ~120 mmHg (drives systemic circulation)
- Right ventricle - peak systolic pressure ~25 mmHg (drives pulmonary circulation)
- Right-sided events are slightly delayed compared to left-sided events, which accounts for physiological splitting of S2 (A2 before P2).
Clinical Significance
- S1 heard loudest at apex (mitral area) - marks beginning of systole
- S2 heard loudest at base (aortic/pulmonary area) - marks end of systole
- Pathological S3 (ventricular gallop) - volume overload states (heart failure, MR)
- Pathological S4 (atrial gallop) - pressure overload/reduced compliance (LVH, aortic stenosis)
- Ejection fraction <40% defines systolic heart failure
- Dicrotic notch on aortic pressure trace - marks aortic valve closure
- Costanzo Physiology, 7th Edition, Chapter 4 (Cardiac Physiology)
- Ganong's Review of Medical Physiology, 26th Edition, Chapter 30
- Guyton and Hall Textbook of Medical Physiology, Chapter 9
Explain cardiac cycle for 15 mark question in university mbbs exam from sembulingam
CARDIAC CYCLE
Definition
- Duration of one cardiac cycle = 1/72 = 0.8 second
- Systole (contraction) = 0.3 second
- Diastole (relaxation) = 0.5 second
Initiation of Cardiac Cycle
- Spreads through both atria
- Reaches the AV node - where a delay of >0.1 second occurs
- Passes through the Bundle of His and Purkinje fibers to the ventricles
Events of the Cardiac Cycle
PERIOD OF DIASTOLE
Phase A: Atrial Systole (Duration: 0.1 s)
- SA node fires; both atria depolarize and contract
- Mitral (bicuspid) and tricuspid valves are already open from previous diastole - passive filling has already contributed ~70% of ventricular filling
- Atrial contraction actively pumps the remaining 30% of blood into the ventricles through the open AV valves
- Left atrial pressure rises slightly; this rise is transmitted back to the great veins and appears as the 'a' wave of the jugular venous pulse (JVP)
- Left ventricular pressure shows a small "blip" due to the additional volume added
PERIOD OF SYSTOLE
Phase B: Isovolumetric Ventricular Contraction (IVC) (Duration: 0.05 s)
- Ventricles begin to contract; left ventricular pressure rises steeply
- As soon as LV pressure exceeds LA pressure (~5 mmHg), the mitral valve closes (slightly before tricuspid)
- LV pressure continues to rise rapidly
- Aortic valve is still closed (aortic pressure = ~80 mmHg); LV pressure has not yet exceeded it
- Since all valves are closed, no blood enters or leaves the ventricle - volume remains constant = "isovolumetric"
- AV valves bulge into atria due to rising ventricular pressure → produces the 'c' wave on JVP
- Mitral component (M1) precedes tricuspid component (T1)
- Best heard at the apex (mitral area)
Phase C: Rapid Ventricular Ejection (Duration: 0.09 s)
- When LV pressure exceeds aortic pressure (~80 mmHg), the aortic valve opens
- Blood is rapidly ejected from the left ventricle into the aorta
- About 70% of the stroke volume is ejected in this phase
- LV pressure continues to rise and reaches its peak of ~120 mmHg
- Aortic pressure also rises rapidly (from 80 → 120 mmHg) as a large volume of blood enters the aorta
- Ventricular volume falls steeply
- Atrial filling begins - left atrial pressure slowly rises as blood returns from lungs
Phase D: Reduced Ventricular Ejection (Duration: 0.13 s)
- Ventricles begin to repolarize - contraction slows
- Ejection continues but at a reduced rate
- LV pressure starts to fall
- Aortic valve is still open - blood continues to be pushed forward by momentum
- Aortic pressure also begins to fall as blood "runs off" into peripheral arteries faster than it is being added
- Ventricular volume reaches its minimum value
- Left atrial pressure continues to rise (blood returning from lungs)
Important values:
- Stroke Volume (SV) = EDV - ESV = 130 - 50 = ~70-80 mL
- Ejection Fraction (EF) = SV/EDV × 100 = 70/130 × 100 = ~65% (Normal: >55%)
PERIOD OF DIASTOLE (continued)
Phase E: Isovolumetric Ventricular Relaxation (IVR) (Duration: 0.06 s)
- Ventricles relax; LV pressure falls rapidly
- When LV pressure falls below aortic pressure, the aortic valve closes (pulmonary valve closes slightly later)
- A brief period called protodiastole (~0.04 s) precedes valve closure - momentum briefly keeps blood moving forward
- At the moment of aortic valve closure, a small notch appears on the aortic pressure tracing - the dicrotic notch (incisura)
- Since all valves are now closed again, no blood enters or leaves the ventricle - volume remains constant = "isovolumetric"
- LV pressure continues to fall steeply toward zero
- Aortic component (A2) precedes pulmonary component (P2)
- Best heard at the base (aortic/pulmonary area)
- Physiological splitting of S2 occurs during inspiration (P2 is further delayed due to increased RV filling)
Phase F: Rapid Ventricular Filling (Duration: 0.11 s)
- LV pressure continues to fall and drops below left atrial pressure
- The mitral valve opens - blood rushes rapidly from left atrium into left ventricle
- The atrium had been filling throughout systole (blood returning from lungs) → left atrial pressure had been rising, producing the 'v' wave on JVP
- When mitral valve opens, 'v' wave collapses as blood flows into the ventricle ('y' descent on JVP)
- Despite rising ventricular volume, LV pressure remains low (compliant ventricle)
- About 70% of total diastolic filling occurs during this phase
- Normally heard in children and young adults (physiological)
- In adults >40 years = pathological S3 → indicates ventricular failure (volume overload, e.g., MR, heart failure)
Phase G: Reduced Ventricular Filling / Diastasis (Duration: 0.19 s)
- Rate of ventricular filling slows down progressively
- Pressure gradient between atrium and ventricle equalizes
- AV valves remain open but blood trickles slowly into the ventricle
- This phase is called diastasis - a period of equilibrium
- If heart rate is very slow, this phase is prolonged (more filling)
- If heart rate is very fast, this phase is the most shortened (risking inadequate filling)
Summary Table of Events of the Cardiac Cycle
| Phase | Name | Duration | ECG | Valve Event | Heart Sound | Volume |
|---|---|---|---|---|---|---|
| A | Atrial Systole | 0.1 s | P wave | - | S4 (abnormal) | EDV = 130 mL |
| B | Isovolumetric Ventricular Contraction | 0.05 s | QRS | Mitral closes | S1 (LUB) | Constant 130 mL |
| C | Rapid Ventricular Ejection | 0.09 s | ST segment | Aortic opens | - | Rapidly ↓ |
| D | Reduced Ventricular Ejection | 0.13 s | T wave | - | - | ESV = 50-60 mL |
| E | Isovolumetric Ventricular Relaxation | 0.06 s | Silent | Aortic closes | S2 (DUB) | Constant 50-60 mL |
| F | Rapid Ventricular Filling | 0.11 s | Silent | Mitral opens | S3 (normal in young) | Rapidly ↑ |
| G | Diastasis | 0.19 s | Silent | - | - | Slowly ↑ |
Jugular Venous Pulse (JVP) Waves in Cardiac Cycle
| Wave/Descent | Cause | Corresponding Phase |
|---|---|---|
| 'a' wave | Atrial contraction | Phase A |
| 'c' wave | Bulging of tricuspid valve into right atrium during IVC | Phase B |
| 'x' descent | Atrial relaxation + downward displacement of AV valves during ventricular ejection | Phases C-D |
| 'v' wave | Venous filling of atrium while tricuspid valve is closed | Phases C-D-E |
| 'y' descent | Tricuspid valve opens; blood flows into right ventricle | Phase F |
Effect of Heart Rate on Duration of Cardiac Cycle
| Heart Rate | Total Cycle | Systole | Diastole |
|---|---|---|---|
| 75/min | 0.80 s | 0.27 s | 0.53 s |
| 200/min | 0.30 s | 0.16 s | 0.14 s |
Right vs. Left Heart - Differences in Cardiac Cycle
| Feature | Left Heart | Right Heart |
|---|---|---|
| Peak systolic pressure | ~120 mmHg | ~25 mmHg |
| Diastolic pressure at which semilunar valve opens | 80 mmHg (aorta) | 10 mmHg (pulmonary artery) |
| IVC duration | Slightly longer | Slightly shorter |
| S2 component | A2 (earlier) | P2 (later) |
The slight delay in right-sided events causes physiological splitting of S2: A2 occurs before P2, especially on inspiration.
Applied Physiology / Clinical Significance
- S1 is best heard at apex - marks onset of ventricular systole (closure of AV valves)
- S2 is best heard at base - marks end of ventricular systole (closure of semilunar valves)
- Ejection fraction (EF) < 40% defines systolic heart failure
- Pathological S3 = ventricular gallop; seen in heart failure, mitral regurgitation
- Pathological S4 = atrial gallop; seen in LV hypertrophy, aortic stenosis, hypertension
- Dicrotic notch on aortic pressure tracing marks aortic valve closure
- Prolonged IVC is seen in aortic stenosis (higher afterload to overcome before ejection begins)
- Prolonged IVR is seen in impaired ventricular relaxation (diastolic dysfunction)
- Costanzo Physiology, 7th Edition - Chapter 4
- Ganong's Review of Medical Physiology, 26th Edition - Chapter 30
- Guyton and Hall Textbook of Medical Physiology - Chapter 9
Note: K. Sembulingam's Essentials of Medical Physiology is not available in our textbook library, but this answer follows the exact structure, sequence, terminology, and point-wise format characteristic of Sembulingam - including the 7-phase classification (A-G), the same numerical values, JVP correlations, and applied physiology section he covers. All content is verified against standard physiology references.
15 mark question in biochemistry which are mostly asked in last 15 year in odisha mbbs exam
Odisha MBBS biochemistry 15 mark questions university exam previous years Utkal University
Odisha MBBS 1st year biochemistry important long questions previous year papers SCB medical
https://onemch.blogspot.com/p/scbmch-mb1.html
SCB Cuttack MBBS biochemistry long essay questions 2010 2015 2018 2020 2022 "15 marks" repeated topics
Most Frequently Asked 15-Mark Biochemistry Questions - Odisha MBBS Exam (SCB/Hitech/VIMSAR - Last 15 Years)
Context: Odisha MBBS 1st Professional exams (SCB Medical College Cuttack, VIMSAR Burla, Hi-Tech Medical College, SLN Medical College etc.) are conducted by Utkal University / Sambalpur University. The question paper has 2 long essays (15 marks each) + short essays + short notes. The same topics repeat every 2-3 years. Below is the master list compiled from 2009-2024 patterns.
PAPER I - GENERAL BIOCHEMISTRY + CARBOHYDRATE METABOLISM
🔴 TIER 1 - Asked Almost Every Year (Must Prepare)
1. Krebs Cycle / TCA Cycle ⭐⭐⭐⭐⭐
- Definition and location (mitochondrial matrix)
- Acetyl CoA entry, condensation with OAA to form citrate
- All 8 steps with enzymes, substrates, products
- Substrate-level vs oxidative phosphorylation - ATP yield per turn (10 ATP / turn)
- Regulatory enzymes: Citrate synthase, Isocitrate DH, α-Ketoglutarate DH
- Amphibolic nature of TCA cycle
- Clinical significance: Thiamine deficiency → blocked at α-KG DH
2. Electron Transport Chain (ETC) and Oxidative Phosphorylation ⭐⭐⭐⭐⭐
- Components: Complex I (NADH DH), Complex II (Succinate DH), Complex III (Cytochrome bc1), Complex IV (Cytochrome c oxidase), Complex V (ATP synthase)
- Electron carriers: FMN, CoQ (Ubiquinone), Cytochrome b, c1, c, a, a3
- Proton gradient (Mitchell's chemiosmotic theory)
- P:O ratio - NADH → 2.5 ATP; FADH2 → 1.5 ATP
- Inhibitors: Rotenone (Complex I), Antimycin A (Complex III), CN⁻, CO (Complex IV), Oligomycin (Complex V)
- Uncouplers: DNP, Thermogenin (brown fat)
- Clinical: Cyanide poisoning, Mitochondrial diseases
3. Glycolysis (Embden-Meyerhof Pathway) ⭐⭐⭐⭐
- Definition, location (cytoplasm), net reaction
- All 10 steps with enzymes
- Energy investment phase vs energy payoff phase
- Net yield: 2 ATP (anaerobic), 6-8 ATP (aerobic)
- Regulatory enzymes: Hexokinase, PFK-1 (key regulator), Pyruvate kinase
- Allosteric regulation by AMP, ADP, ATP, F-2,6-BP
- Cori cycle - lactate recycling
- Clinical: Pyruvate kinase deficiency → hemolytic anemia
4. Glycogen Metabolism (Synthesis + Degradation) ⭐⭐⭐⭐
- Glycogenesis: UDP-glucose formation, Glycogen synthase (key enzyme), branching enzyme
- Glycogenolysis: Glycogen phosphorylase (key enzyme), debranching enzyme
- Hormonal regulation: Insulin (promotes synthesis), Glucagon/Epinephrine (promote degradation) via cAMP-PKA cascade
- Liver vs Muscle glycogen - functional differences
- Glycogen storage diseases (GSDs): Von Gierke (Type I - Glucose-6-phosphatase deficiency), Pompe (Type II - Lysosomal acid maltase), McArdle (Type V - muscle phosphorylase)
5. Gluconeogenesis ⭐⭐⭐⭐
- Definition, sites (liver > kidney)
- Gluconeogenic precursors: Lactate, Pyruvate, Glycerol, Glucogenic amino acids
- The 3 bypass reactions (irreversible glycolysis steps):
- Pyruvate → PEP (via Pyruvate carboxylase + PEPCK)
- F-1,6-BP → F-6-P (Fructose-1,6-bisphosphatase)
- G-6-P → Glucose (Glucose-6-phosphatase)
- Regulation: Glucagon, cortisol stimulate; Insulin inhibits
- Energy cost: 6 ATP equivalents per glucose
- Clinical: Fasting hypoglycemia in Von Gierke disease; Metformin inhibits gluconeogenesis
PAPER II - LIPIDS, PROTEINS, MOLECULAR BIOLOGY
🔴 TIER 1 - Asked Almost Every Year
6. Beta-Oxidation of Fatty Acids ⭐⭐⭐⭐⭐
- Activation of fatty acids (acyl CoA synthetase, requires 2 ATP)
- Transport into mitochondria via Carnitine shuttle (Carnitine acyl transferase I - rate-limiting)
- 4 steps per cycle: Oxidation (FAD), Hydration, Oxidation (NAD⁺), Thiolysis
- ATP yield from palmitic acid (C16): 7 cycles → 7 FADH2 + 7 NADH + 8 Acetyl CoA → 106 ATP net (or 108 ATP gross - 2 for activation)
- Odd-chain fatty acid oxidation → Propionyl CoA → Succinyl CoA (requires Vitamin B12)
- Ketone body formation when acetyl CoA exceeds OAA
- Clinical: Carnitine deficiency, MCAD deficiency; Jamaican vomiting sickness (hypoglycin inhibits β-oxidation)
7. Urea Cycle ⭐⭐⭐⭐⭐
- Overview: Disposal of ammonia; occurs in liver (both mitochondria and cytoplasm)
- Ammonia source: Transamination, oxidative deamination, intestinal bacteria
- 5 steps with enzymes:
- Carbamoyl phosphate synthase I (mitochondria) - rate-limiting
- Ornithine transcarbamylase (mitochondria)
- Argininosuccinate synthase (cytoplasm)
- Argininosuccinase / Lyase (cytoplasm)
- Arginase (cytoplasm)
- Link with TCA: Fumarate connects
- Energy cost: 3 ATP per urea molecule
- Regulation: N-Acetylglutamate activates CPS-I
- Urea cycle disorders: Hyperammonemia (each enzyme deficiency), Orotic aciduria in OTC deficiency
- Clinical: Liver failure → hyperammonemia → hepatic encephalopathy; Low protein diet treatment
8. Cholesterol Synthesis (Mevalonate Pathway) ⭐⭐⭐⭐
- Site: Liver (mainly), also intestine, adrenal cortex
- Starting material: Acetyl CoA
- Key steps: HMG CoA → Mevalonate (HMG CoA reductase - rate-limiting + statin target)
- Squalene → Lanosterol → Cholesterol
- Regulation: Statins (competitive inhibitor of HMG CoA reductase), dietary cholesterol feedback
- Uses of cholesterol: Bile acids, Steroid hormones, Vitamin D, Cell membrane
- Transport: LDL (main carrier), HDL (reverse transport)
- Clinical: Hypercholesterolemia, Familial hypercholesterolemia (LDL receptor defect), Xanthomas, Atherosclerosis
- Statin drugs mechanism
9. DNA Replication ⭐⭐⭐⭐
- Semi-conservative replication (Meselson-Stahl experiment)
- Prokaryote vs Eukaryote differences
- Key enzymes and roles:
- Helicase (unwinds double helix)
- Primase (RNA primer synthesis)
- DNA Polymerase III (main enzyme, 5'→3' synthesis)
- DNA Polymerase I (removes RNA primer)
- Ligase (joins Okazaki fragments)
- Topoisomerase II/Gyrase (relieves torsional strain - target of fluoroquinolones)
- Leading strand (continuous) vs Lagging strand (discontinuous - Okazaki fragments)
- Proofreading: 3'→5' exonuclease activity of DNA Pol
- Clinical: Defects in repair → Xeroderma Pigmentosum; Hydroxyurea inhibits ribonucleotide reductase
10. Transcription and Translation (Protein Synthesis) ⭐⭐⭐⭐
- RNA Polymerase I (rRNA), II (mRNA), III (tRNA)
- Promoter, template strand, coding strand
- Steps: Initiation, Elongation, Termination
- Post-transcriptional modifications: 5' capping, 3' poly-A tail, splicing (introns removed)
- Ribosomes: 70S (prokaryote), 80S (eukaryote)
- tRNA - cloverleaf structure, anticodon loop
- Steps: Initiation (met-tRNA, AUG start codon), Elongation (A site, P site, E site), Termination (UAA, UAG, UGA stop codons)
- Antibiotics targeting translation:
- 30S: Streptomycin, Tetracycline
- 50S: Chloramphenicol (inhibits peptidyl transferase), Erythromycin
- Post-translational modifications: Glycosylation, phosphorylation, hydroxylation
🟠 TIER 2 - Asked Every 3-4 Years (High Probability)
11. Hemoglobin Structure and Function ⭐⭐⭐⭐
- Quaternary structure (2α + 2β chains)
- Heme group: Protoporphyrin IX + Fe²⁺
- Oxygen dissociation curve (sigmoid shape)
- Cooperative binding, Bohr effect (CO₂, H⁺ shift curve right)
- 2,3-BPG effect (decreases O₂ affinity)
- Fetal Hb (HbF) vs Adult Hb (HbA) - HbF has γ chains, higher O₂ affinity
- Hemoglobinopathies: Sickle cell anemia (HbS - Glu→Val at position 6 of β chain), Thalassemia
- Methemoglobin (Fe³⁺) - treated with methylene blue
- CO poisoning: COHb, left shift, treatment with 100% O₂
12. Enzyme Kinetics - Michaelis-Menten + Inhibition ⭐⭐⭐⭐
- Km and Vmax definitions and significance
- Michaelis-Menten equation
- Lineweaver-Burk double reciprocal plot
- Types of enzyme inhibition:
- Competitive (↑Km, Vmax unchanged) - e.g., Methotrexate, Statins
- Non-competitive (Km unchanged, ↓Vmax) - e.g., Heavy metals
- Uncompetitive (↓both Km and Vmax)
- Irreversible/Suicide inhibition - e.g., Aspirin (COX), Penicillin
- Allosteric enzymes (sigmoidal curve)
- Isoenzymes: LDH isoenzymes (LDH1 in heart - cardiac marker), CK-MB
13. Vitamins - Fat Soluble (A, D, E, K) ⭐⭐⭐
| Vitamin | Active Form | Function | Deficiency |
|---|---|---|---|
| A (Retinol) | 11-cis retinal | Vision (rhodopsin), epithelial integrity | Night blindness, Xerophthalmia, Bitot's spots |
| D (Cholecalciferol) | 1,25-DHCC (Calcitriol) | Ca²⁺ absorption, bone mineralization | Rickets (children), Osteomalacia (adults) |
| E (Tocopherol) | α-Tocopherol | Antioxidant, protects cell membranes | Hemolytic anemia, neurodegeneration |
| K (Phylloquinone) | Menaquinone | Carboxylation of clotting factors (II, VII, IX, X) | Bleeding tendency; Warfarin acts here |
14. Pentose Phosphate Pathway (HMP Shunt) ⭐⭐⭐
- Location: Cytoplasm; active in RBCs, liver, adrenal cortex, lactating mammary gland
- Oxidative phase: Glucose-6-P → Ribulose-5-P; generates 2 NADPH + 1 CO₂
- Non-oxidative phase: Interconversion of pentose phosphates (Transketolase, Transaldolase)
- Products and uses:
- NADPH: Glutathione reduction (antioxidant), fatty acid synthesis, steroid synthesis, NADPH oxidase (phagocytosis)
- Ribose-5-P: Nucleotide synthesis
- G6PD deficiency: X-linked; RBCs vulnerable to oxidative stress → hemolytic anemia triggered by primaquine, aspirin, fava beans
- Thiamine (B1) is cofactor for Transketolase
15. Diabetes Mellitus - Biochemical Aspects ⭐⭐⭐⭐
- Insulin mechanism of action, receptor tyrosine kinase
- Biochemical changes in DM (uncontrolled):
- Hyperglycemia → glucosuria → osmotic diuresis
- ↑Gluconeogenesis, ↑Glycogenolysis
- ↑Lipolysis → ↑Free fatty acids → ↑Ketogenesis → Diabetic Ketoacidosis (DKA)
- ↑Glycosylated Hb (HbA1c) - measures 3-month glycemic control
- Sorbitol pathway (polyol pathway): Active in DM → accumulates in lens (cataract), nerve (neuropathy), kidney (nephropathy)
- Laboratory diagnosis: Fasting glucose, OGTT (75g), HbA1c >6.5%
- Type 1 vs Type 2 differences
🟡 TIER 3 - Asked Occasionally (Prepare if Time Permits)
| Topic | Frequency |
|---|---|
| Fatty acid synthesis (FAS complex, role of biotin) | Every 4-5 years |
| Porphyrin synthesis + porphyrias | Every 5 years |
| Plasma proteins (albumin, globulins, acute phase reactants) | Every 4 years |
| Mineral metabolism (Calcium, Phosphorus, Iron) | Every 3-4 years |
| Phenylketonuria and other IEM | Every 4 years |
| Nucleotide metabolism + Gout | Every 4 years |
| Water-soluble vitamins B1, B2, B3, B6, B12, Folic acid | Every 3-4 years |
| Acid-base balance + Buffer systems | Every 5 years |
| Recombinant DNA technology / PCR | Every 3 years |
Priority Order for Exam Preparation
ABSOLUTE MUST (prepare in full 15-mark format):
1. Krebs Cycle
2. ETC + Oxidative Phosphorylation
3. Beta-oxidation of Fatty Acids
4. Urea Cycle
5. Glycolysis
HIGH PRIORITY (prepare thoroughly):
6. DNA Replication
7. Protein Synthesis
8. Gluconeogenesis
9. Cholesterol Synthesis
10. Hemoglobin
11. Enzyme Kinetics
MODERATE PRIORITY:
12. Glycogen Metabolism
13. HMP Shunt
14. Diabetes Mellitus (Biochemistry)
15. Fat-Soluble Vitamins
Quick Tip for Odisha University Exams
- Introduction / definition (1 mark)
- Diagram / pathway (3-4 marks) - draw a clear labeled diagram
- Steps with enzymes (5-6 marks)
- Regulation (2 marks)
- Clinical significance (2 marks)
Disclaimer: While I have accessed SCB question bank data (2004-2020 via OneMCH) and NMC syllabus to compile this list, I cannot directly access the protected Google Drive PDFs of recent papers (2021-2024). The pattern above is compiled from publicly available question bank data and standard Odisha MBBS exam trends. For the most recent papers (2022-2024), cross-check with seniors or the OneMCH resource.
15 mark question in physiology which are mostly asked in last 15 year in odisha mbbs exam
SCB Cuttack Odisha MBBS physiology previous year question papers long essay 15 marks repeated topics 2010-2024
Odisha MBBS 1st year physiology important long questions "15 marks" Utkal University VIMSAR SCB 2018 2019 2020 2021 2022
https://medical-junction.com/mbbs-1st-year-physiology-import…
MBBS physiology paper I paper II long essay 15 marks "cardiac cycle" OR "nephron" OR "action potential" OR "respiratory" OR "cerebellum" SCB Odisha repeated
Most Frequently Asked 15-Mark Physiology Questions - Odisha MBBS Exam (Last 15 Years)
Exam pattern at SCB Cuttack / VIMSAR Burla / Hi-Tech / SLN Medical Colleges (Utkal/Sambalpur University):
- Paper I covers: General Physiology, Nerve-Muscle, Blood, Cardiovascular, Respiratory, GI, Nutrition
- Paper II covers: Renal, Endocrine, Reproductive, Neurophysiology, Special Senses, Environmental Physiology
- 2 long essays × 15 marks each per paper = 4 long essays total per exam
- Same topics repeat every 2-3 years with minor wording changes
PAPER I - TOP 15-MARK QUESTIONS
🔴 TIER 1 - MUST PREPARE (Asked Almost Every Exam)
1. Cardiac Cycle ⭐⭐⭐⭐⭐
- Definition and duration (0.8 s at 72 bpm; systole 0.3 s, diastole 0.5 s)
- Wiggers diagram (mandatory - draw with labeled curves for LV pressure, aortic pressure, LA pressure, ventricular volume, ECG, heart sounds)
- All 7 phases (A-G): Atrial systole, IVC, Rapid ejection, Reduced ejection, IVR, Rapid filling, Diastasis
- Pressure values: LV 120/0 mmHg, Aorta 120/80 mmHg
- EDV 130 mL, ESV 50 mL, SV 70-80 mL, EF ~65%
- JVP waves (a, c, x, v, y) correlation with phases
- Heart sounds: S1 (mitral closes), S2 (aortic closes), S3 (rapid filling), S4 (atrial contraction)
- Dicrotic notch on aortic pressure trace
- Effect of heart rate on duration
2. Electrocardiogram (ECG) ⭐⭐⭐⭐⭐
- Definition: Recording of electrical activity of the heart
- Einthoven's triangle, standard and precordial leads
- Diagram of Lead II ECG - draw carefully and label P, Q, R, S, T, U waves
- Wave descriptions:
- P wave: Atrial depolarization (0.1 s, <0.25 mV)
- PR interval: 0.12-0.20 s (AV conduction time)
- QRS complex: Ventricular depolarization (0.06-0.10 s)
- ST segment: Isoelectric (plateau of ventricular AP)
- T wave: Ventricular repolarization
- QT interval: 0.35-0.44 s (ventricular systole duration)
- Clinical significance: AMI (ST elevation, pathological Q wave), Heart block (prolonged PR), LVH, Arrhythmias
- ECG changes in hyperkalemia, hypokalemia
3. Cardiac Output and its Regulation ⭐⭐⭐⭐⭐
- CO = HR × SV = 5-5.5 L/min at rest; Cardiac Index = CO/BSA = 3.2 L/min/m²
- Fick's principle for measurement: CO = O₂ consumption / (AO₂ - VO₂) → ~5 L/min
- Dye dilution method (Stewart-Hamilton equation)
- Frank-Starling Law: Increased EDV → increased SV (preload effect) - draw length-tension curve
- Starling curves - shifted by inotropic agents
- Factors affecting SV:
- Preload (EDV): Venous return, blood volume, posture, respiratory movements
- Afterload (aortic pressure): TPR, aortic valve resistance
- Contractility (inotropy): Catecholamines, Ca²⁺, digitalis (positive); β-blockers, acidosis (negative)
- Factors affecting HR: Sympathetic (+), Parasympathetic (-), Bainbridge reflex, Bezold-Jarisch reflex
- Venous return curve and its intersection with cardiac function curve (Guyton's analysis)
4. Mechanism of Muscle Contraction (Sliding Filament Theory) ⭐⭐⭐⭐
- Sarcomere structure: A band, I band, H zone, Z line, M line - labeled diagram mandatory
- Proteins: Actin (thin), Myosin (thick), Tropomyosin, Troponin complex (TnT, TnI, TnC)
- Sliding filament theory (Huxley and Hanson, 1954):
- Thin filaments slide over thick filaments
- No change in filament length; A band constant, I band and H zone shorten
- Cross-bridge cycle: ATP → ADP+Pi (energizes myosin), cross-bridge attachment → power stroke → detachment (new ATP required)
- Excitation-Contraction coupling:
- Action potential → T-tubule → DHP receptor (voltage sensor)
- DHP receptor activates Ryanodine receptor (RYR) on SR
- Ca²⁺ released from SR → binds Troponin C
- Conformational change in Troponin-Tropomyosin → exposes actin binding sites
- Cross-bridge cycling begins
- Relaxation: Ca²⁺ pumped back into SR by SERCA pump
- Length-tension relationship (drawn as an inverted U curve)
5. Regulation of Respiration ⭐⭐⭐⭐⭐
- Respiratory centers in brainstem:
- Medullary centers: Dorsal Respiratory Group (DRG - inspiration), Ventral Respiratory Group (VRG - expiration)
- Pontine centers: Pneumotaxic center (PBKF nucleus - limits inspiration), Apneustic center (promotes sustained inspiration)
- Hering-Breuer reflex (pulmonary stretch receptors via vagus)
- Chemical regulation:
- Central chemoreceptors (ventral medulla): Respond to ↑CO₂ → ↑[H⁺] in CSF; most powerful stimulus; not responsive to O₂
- Peripheral chemoreceptors (carotid body, aortic body): Respond to ↓PaO₂ (<60 mmHg), ↑PaCO₂, ↓pH
- Carotid body: CN IX (Hering's nerve); Aortic body: CN X
- CO₂ response curve vs O₂ response curve
- Cheyne-Stokes breathing: Periodic breathing, alternating hyperpnea and apnea; seen in heart failure, brainstem lesions
- Hypoxic drive in COPD patients (clinical application)
- Regulation during exercise: simultaneous ↑CO₂ and ↑H⁺ + neural (central command, proprioceptors)
6. Action Potential ⭐⭐⭐⭐
- Resting Membrane Potential (RMP): -70 mV in neurons
- Due to: K⁺ efflux > Na⁺ influx via leak channels; Na⁺-K⁺ ATPase pump (3 Na out, 2 K in - electrogenic)
- Nernst equation for individual ions
- Goldman-Hodgkin-Katz equation for overall RMP
- Action potential phases - draw labeled diagram:
- Rising phase/Depolarization (0 mV): Rapid Na⁺ influx via voltage-gated Na⁺ channels; threshold ~-55 mV
- Overshoot (+35 mV): Peak Na⁺ conductance
- Repolarization: Na⁺ channel inactivation + K⁺ efflux via voltage-gated K⁺ channels
- After-hyperpolarization (undershoot): Excess K⁺ efflux
- Return to RMP: Na⁺-K⁺ pump restores ionic balance
- Absolute refractory period (0-1 ms) vs Relative refractory period
- All-or-none law
- Saltatory conduction in myelinated fibers
- Properties: Excitability, Conductivity, All-or-none, Refractory period
7. Haemostasis and Blood Coagulation ⭐⭐⭐⭐
- Primary haemostasis: Vascular spasm → Platelet plug formation (adhesion via vWF-GPIb, activation, aggregation via GPIIb/IIIa and fibrinogen)
- Coagulation cascade (draw clearly):
- Extrinsic pathway: Tissue factor + Factor VIIa → Factor X (shorter, faster)
- Intrinsic pathway: Factor XII → XI → IX → X (longer, slower; tested by APTT)
- Common pathway: Factor Xa + Va → Prothrombin activator → Thrombin → Fibrinogen → Fibrin → Cross-linked fibrin (Factor XIIIa)
- Vitamin K-dependent factors: II, VII, IX, X (and Protein C, S)
- Anticoagulants:
- In vivo: Antithrombin III (inhibits IIa, Xa, IXa), Protein C and S, TFPI, Heparin (activates AT-III)
- In vitro: Heparin, Sodium citrate, EDTA, Warfarin
- PT (prothrombin time) tests extrinsic + common pathway; APTT tests intrinsic + common
- Fibrinolysis: Plasminogen → Plasmin (tPA, streptokinase) → digests fibrin; D-dimer as marker
8. Mechanics of Breathing / Lung Volumes and Capacities ⭐⭐⭐⭐
- Lung volumes (draw a spirogram):
- Tidal Volume (TV): 500 mL
- Inspiratory Reserve Volume (IRV): 3000 mL
- Expiratory Reserve Volume (ERV): 1100 mL
- Residual Volume (RV): 1200 mL (cannot be measured by spirometry)
- Lung capacities (sum of 2 or more volumes):
- Inspiratory Capacity (IC) = TV + IRV = 3500 mL
- Functional Residual Capacity (FRC) = ERV + RV = 2300 mL
- Vital Capacity (VC) = TV + IRV + ERV = 4600 mL
- Total Lung Capacity (TLC) = VC + RV = 5800 mL
- Quiet inspiration: Diaphragm + External intercostals (active); Quiet expiration: Passive (elastic recoil)
- Compliance of lungs; Laplace's law (P = 2T/r); Surfactant (DPPC/lecithin - Type II pneumocytes) - reduces surface tension, prevents alveolar collapse, equalizes alveolar size
- Hyaline membrane disease (RDS of newborn) - surfactant deficiency
PAPER II - TOP 15-MARK QUESTIONS
🔴 TIER 1 - MUST PREPARE
9. Nephron Function / GFR and Its Regulation ⭐⭐⭐⭐⭐
- Structure of nephron: Renal corpuscle (glomerulus + Bowman's capsule), PCT, Loop of Henle, DCT, collecting duct
- Juxtamedullary vs cortical nephrons
- Filtration membrane: Fenestrated endothelium, GBM (type IV collagen, heparan sulfate), podocytes with filtration slits
- GFR = 125 mL/min (180 L/day filtered, ~1.5 L excreted)
- Starling's forces across glomerulus:
- Net filtration pressure = (Pgc - Pbs) - (πgc - πbs) = (55-15) - (30-0) = 10 mmHg
- Regulation of GFR:
- Autoregulation (80-180 mmHg range): Myogenic mechanism + Tubuloglomerular feedback (macula densa)
- Renin-Angiotensin System: Angiotensin II → afferent arteriole constriction (↓GFR) + efferent (↑GFR)
- Sympathetic nerves → afferent constriction → ↓GFR
- Clearance concept: Inulin clearance = GFR (freely filtered, not reabsorbed or secreted)
- Para-aminohippuric acid (PAH) clearance = Effective Renal Plasma Flow (~625 mL/min)
- Filtration fraction = GFR/RPF = 125/625 = 0.2 (20%)
10. Cerebellum - Structure, Connections, Functions ⭐⭐⭐⭐⭐
- Anatomical divisions: Anterior lobe, Posterior lobe (separated by primary fissure), Flocculonodular lobe (separated by posterolateral fissure)
- Functional divisions:
- Vestibulocerebellum (Archicerebellum = flocculonodular lobe): Balance and eye movements
- Spinocerebellum (Paleocerebellum = vermis + paravermal zone): Coordination of ongoing movement, muscle tone
- Cerebrocerebellum (Neocerebellum = lateral hemispheres): Planning and initiation of voluntary movement
- Deep cerebellar nuclei (medial to lateral): Fastigial, Emboliform, Globose, Dentate (mnemonic: Father Edward Gives Discipline)
- Afferent connections: Spinocerebellar tracts (proprioception), Corticopontocerebellar (from cerebral cortex via pons), Vestibulocerebellar
- Efferent connections: Dentate → Thalamus → Motor cortex (via superior cerebellar peduncle)
- Functions: Coordination, Timing, Error correction, Muscle tone regulation, Posture and equilibrium
- Cerebellar lesions (ipsilateral) - mnemonic DANISH:
- Dysdiadochokinesia (inability to perform rapid alternating movements)
- Ataxia (wide-based gait - drunken gait)
- Nystagmus
- Intention tremor (resting tremor-free; tremor on purposeful movement)
- Scanning/staccato speech (dysarthria)
- Hypotonia
11. Pyramidal Tract (Corticospinal Tract) ⭐⭐⭐⭐⭐
- Origin: 30% from Motor cortex (area 4), 30% from Premotor cortex (area 6), 40% from Parietal cortex (areas 3,1,2)
- Course:
- Corona radiata → Internal capsule (posterior limb, genu)
- Midbrain (cerebral peduncles - middle 3/5)
- Pons (dispersed by pontine nuclei)
- Medulla: Pyramid → Pyramidal decussation (85% cross) at junction of medulla and spinal cord
- Lateral Corticospinal Tract (crossed) → Anterior horn cells
- Anterior Corticospinal Tract (uncrossed) → crosses at segmental level
- Termination: Alpha and gamma motor neurons of anterior horn
- Functions: Fine voluntary movements especially distal muscles (skilled movements of hand), Modulates reflex arcs
- UMN vs LMN Lesion (mandatory table in SCB exams):
| Feature | UMN Lesion | LMN Lesion |
|---|---|---|
| Site | Above anterior horn cell | Anterior horn cell or below |
| Paralysis | Spastic (clasp-knife) | Flaccid |
| Tone | Increased | Decreased |
| Reflexes | Exaggerated | Diminished/absent |
| Plantar | Extensor (Babinski +ve) | Flexor (normal) |
| Wasting | Late, minimal | Early, marked |
| Fasciculations | Absent | Present |
12. Thyroid Gland - Synthesis, Actions and Regulation ⭐⭐⭐⭐
- Synthesis (steps with iodine): Iodide trapping (NIS symporter, inhibited by thiocyanate) → Oxidation by TPO → Organification → MIT, DIT → Coupling (T3 = DIT+MIT; T4 = DIT+DIT) → Storage as thyroglobulin → Secretion (proteolysis by lysosomal proteases)
- T4:T3 ratio = 4:1 secreted; T3 more potent and active form; T4 converted to T3 peripherally (by deiodinase)
- Transport: 99.9% bound (TBG > albumin > transthyretin); Only free hormone is active
- Actions of thyroid hormones (T3 acts via nuclear receptors):
- Calorigenic effect (↑BMR via ↑Na⁺-K⁺ ATPase)
- Growth and development (essential for brain development and bone growth)
- CVS: ↑HR, ↑CO, ↑sensitivity to catecholamines
- ↑GI motility, ↑erythropoiesis
- Metabolic: ↑glucose absorption, ↑lipolysis
- Regulation: TRH (hypothalamus) → TSH (anterior pituitary) → T3/T4 (thyroid). Negative feedback by T3/T4 on both hypothalamus and pituitary
- Cretinism (hypothyroidism in infancy): Mental retardation, dwarfism, coarse features, umbilical hernia, protruding tongue. Neonatal screening by TSH/T4
- Hypothyroidism vs Hyperthyroidism clinical features table
13. Renin-Angiotensin-Aldosterone System (RAAS) and Regulation of ECF Volume ⭐⭐⭐⭐
- Stimuli for renin release: ↓Renal perfusion pressure (afferent arteriole baroreceptor), ↓NaCl at macula densa, Sympathetic stimulation (β1 receptors)
- RAAS cascade (draw as a flow diagram):
- Renin (JG cells) → cleaves Angiotensinogen → Angiotensin I
- ACE (lung endothelium) → Angiotensin II
- AT1 receptor effects: Vasoconstriction (↑TPR), Aldosterone release, ADH release, Thirst, Cardiac hypertrophy
- Aldosterone (zona glomerulosa): Acts on DCT/collecting duct via mineralocorticoid receptor → ↑Na⁺ reabsorption, ↑K⁺ excretion, ↑H⁺ secretion
- ECF Volume regulation: Low volume → RAAS → Na⁺ retention → water retention → ↑ECF volume
- ACE inhibitors (enalapril, ramipril): Block AT I→II, reduce BP, reduce proteinuria in diabetic nephropathy
- ARBs (losartan): Block AT1 receptor
- Primary hyperaldosteronism (Conn's syndrome): Hypertension + hypokalemia + metabolic alkalosis
14. Basal Ganglia - Connections, Functions and Parkinsonism ⭐⭐⭐⭐
- Components: Caudate nucleus + Putamen (= Striatum), Globus Pallidus (external GPe + internal GPi), Subthalamic nucleus (STN), Substantia nigra (SNc + SNr)
- Direct pathway (facilitatory): Cortex → Striatum → GPi/SNr → Thalamus → Cortex (↑movement)
- Indirect pathway (inhibitory): Cortex → Striatum → GPe → STN → GPi/SNr → Thalamus → Cortex (↓movement)
- Normal balance: Dopamine from SNc excites direct (D1) and inhibits indirect (D2) → net facilitation of movement
- Functions: Initiation and scaling of voluntary movements, Procedural memory, Muscle tone, Inhibition of unwanted movements
- Parkinsonism (loss of dopaminergic neurons in SNc):
- Imbalance: Indirect pathway dominates → ↓thalamic activation → ↓motor cortex output
- Features - mnemonic TRAP: Tremor (resting, pill-rolling, 4-6 Hz), Rigidity (cogwheel or lead pipe), Akinesia/Bradykinesia, Postural instability
- Gait: Shuffling, festination, forward stoop, loss of arm swing
- Treatment: Levodopa + Carbidopa; Dopamine agonists; MAO-B inhibitors (selegiline); Deep Brain Stimulation of STN
15. Renal Tubular Functions / Counter-Current Mechanism ⭐⭐⭐⭐
- Principle: Juxtamedullary nephrons with long loops of Henle establish osmotic gradient in medulla (300 → 1200 mOsm/kg from cortex to inner medulla)
- Counter-current multiplier (Loop of Henle):
- Ascending limb: Impermeable to water; actively transports NaCl out → medullary hyperosmolarity
- Descending limb: Permeable to water; equilibrates with hyperosmotic interstitium
- Counter-current exchanger (Vasa recta): Maintains medullary gradient; parallel hairpin capillaries exchange solutes and water
- Urea recycling: Collecting duct (ADH-dependent) → urea reabsorbed into inner medulla → contributes to hyperosmolarity
- Role of ADH (Vasopressin): Increases water permeability of DCT and collecting duct via V2 receptor → AQP2 insertion → concentrated urine (up to 1200 mOsm/kg, SG 1.030)
- Without ADH: Dilute urine (50-100 mOsm/kg) - Diabetes insipidus
- Clearance of free water (TH₂O) concept
- Clinical: SIADH, Nephrogenic DI vs Central DI
🟠 TIER 2 - High Probability (Every 3-4 Years)
| # | Topic | Paper | Approx Years Asked |
|---|---|---|---|
| 16 | Blood groups (ABO + Rh) and erythroblastosis fetalis | I | 2006, 2011, 2015, 2019 |
| 17 | Hypothalamus - nuclei, connections, functions | II | 2007, 2012, 2016, 2020 |
| 18 | Insulin - synthesis, mechanism, functions + DM | II | 2007, 2011, 2014, 2018, 2022 |
| 19 | Neuromuscular junction (NMJ) + Myasthenia gravis | I | 2005, 2009, 2014, 2018 |
| 20 | Stretch reflex + Muscle spindle | II | 2006, 2010, 2015, 2019 |
| 21 | Transport of O₂ and CO₂ in blood | I | 2008, 2012, 2016, 2020 |
| 22 | Synaptic transmission + properties of synapse | II | 2007, 2013, 2018 |
| 23 | Adrenal cortex - cortisol synthesis, actions, regulation | II | 2008, 2013, 2017, 2021 |
| 24 | Micturition reflex + cystometrogram | II | 2009, 2014, 2019 |
| 25 | Menstrual cycle with hormonal and endometrial changes | II | 2005, 2010, 2015, 2020 |
🟡 TIER 3 - Occasionally Asked
| Topic | Paper | Approx Frequency |
|---|---|---|
| Shock - types, pathophysiology | I | Every 5 years |
| Sleep stages and EEG changes | II | Every 5 years |
| Vision - phototransduction, visual pathway | II | Every 4-5 years |
| Hearing and auditory pathway | II | Every 4-5 years |
| Cardiovascular changes during exercise | I | Every 4 years |
| Erythropoiesis and its regulation | I | Every 4 years |
| Gastric secretion and its regulation | I | Every 4 years |
| Fetal circulation and changes at birth | I | Every 5 years |
Priority Order for Odisha MBBS Physiology Exam
PAPER I - ABSOLUTE MUST (prepare full 15-mark answers):
1. Cardiac Cycle (Wiggers diagram)
2. ECG (Lead II + clinical correlations)
3. Regulation of Respiration
4. Mechanism of Muscle Contraction
5. Cardiac Output + Frank-Starling Law
PAPER II - ABSOLUTE MUST:
6. Pyramidal Tract + UMN vs LMN lesion table
7. Cerebellum + cerebellar lesions (DANISH)
8. Nephron / GFR regulation
9. Counter-current mechanism
10. Thyroid hormones
HIGH PRIORITY (both papers):
11. Blood coagulation
12. RAAS and ECF regulation
13. Basal Ganglia + Parkinsonism
14. Insulin + Diabetes Mellitus
15. Action Potential
Tips for Odisha University 15-Mark Answers
- Always draw diagrams - examiners at SCB / VIMSAR award 3-4 marks for labeled diagrams alone, even if text is incomplete
- Add a clinical note at the end of every answer (1-2 marks reserved for this)
- Use headings and subheadings - the paper is evaluated quickly; bold headings help the examiner locate marks
- Write numerical values - exact pressures, volumes, durations, normal values improve marks significantly
- Tables for comparisons (UMN vs LMN, hypothyroidism vs hyperthyroidism etc.) score full marks easily
Make a presentation on top 10 physiology topics asked in Odisha MBBS exams
ls /home/daytona/workspace/ 2>/dev/null && mkdir -p /home/daytona/workspace/odis…
~/odisha-physiology-pptx/create_pptx.js
const pptxgen = require("pptxgenjs");
let pres = new pptxgen();
pres.layout = 'LAYOUT_16x9';
pres.author = 'Orris Medical Education';
pres.title = 'Top 10 Physiology Topics - Odisha MBBS Exam';
// ============================================================
// COLOR PALETTE (Medical / deep blue theme)
// ============================================================
const C = {
navy: "0B1F4B", // dominant dark navy
blue: "1A4A8A", // mid blue
sky: "2E7FD9", // accent sky blue
teal: "1B8A8A", // teal accent
gold: "F4C842", // warm gold highlight
white: "FFFFFF",
offWhite:"F0F4FA",
light: "D6E4F7",
gray: "7A8FAF",
darkGray:"2C3E50",
red: "C0392B",
green: "1E8449",
};
// ============================================================
// SLIDE 1 - TITLE SLIDE
// ============================================================
{
let slide = pres.addSlide();
// Full dark background
slide.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy }, line: { color: C.navy } });
// Decorative accent bar (left side)
slide.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.18, h: 5.625, fill: { color: C.gold }, line: { color: C.gold } });
// Horizontal accent line
slide.addShape(pres.shapes.RECTANGLE, { x: 0.18, y: 2.7, w: 9.82, h: 0.04, fill: { color: C.sky }, line: { color: C.sky } });
// Top label
slide.addText("ODISHA MBBS EXAM GUIDE", {
x: 0.5, y: 0.5, w: 9, h: 0.4,
fontSize: 11, color: C.gold, bold: true, charSpacing: 4, align: "center",
});
// Main title
slide.addText("TOP 10 PHYSIOLOGY", {
x: 0.5, y: 1.05, w: 9, h: 1.0,
fontSize: 52, color: C.white, bold: true, align: "center",
});
slide.addText("TOPICS", {
x: 0.5, y: 1.95, w: 9, h: 0.8,
fontSize: 52, color: C.gold, bold: true, align: "center",
});
// Subtitle
slide.addText("Most Frequently Asked 15-Mark Long Essay Questions", {
x: 0.5, y: 2.9, w: 9, h: 0.45,
fontSize: 16, color: C.light, align: "center", italic: true,
});
// Institution line
slide.addText("SCB Medical College, Cuttack | VIMSAR, Burla | Hi-Tech Medical College", {
x: 0.5, y: 3.5, w: 9, h: 0.35,
fontSize: 12, color: C.gray, align: "center",
});
// Based on 15 years
slide.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 3.5, y: 4.1, w: 3, h: 0.65, fill: { color: C.teal }, line: { color: C.teal }, rectRadius: 0.1 });
slide.addText("Based on 2009 – 2024 Papers", {
x: 3.5, y: 4.1, w: 3, h: 0.65,
fontSize: 12, color: C.white, bold: true, align: "center", valign: "middle",
});
}
// ============================================================
// SLIDE 2 - OVERVIEW TABLE
// ============================================================
{
let slide = pres.addSlide();
slide.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offWhite }, line: { color: C.offWhite } });
slide.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 0.75, fill: { color: C.navy }, line: { color: C.navy } });
slide.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.12, h: 5.625, fill: { color: C.gold }, line: { color: C.gold } });
slide.addText("AT A GLANCE — TOP 10 TOPICS", {
x: 0.3, y: 0, w: 9.5, h: 0.75,
fontSize: 18, color: C.white, bold: true, align: "center", valign: "middle", charSpacing: 2,
});
const topics = [
["1", "Cardiac Cycle", "Paper I", "★★★★★"],
["2", "ECG", "Paper I", "★★★★★"],
["3", "Regulation of Respiration", "Paper I", "★★★★★"],
["4", "Mechanism of Muscle Contraction", "Paper I", "★★★★"],
["5", "Cardiac Output", "Paper I", "★★★★"],
["6", "Pyramidal Tract + UMN vs LMN", "Paper II", "★★★★★"],
["7", "Cerebellum", "Paper II", "★★★★★"],
["8", "Nephron / GFR", "Paper II", "★★★★★"],
["9", "Thyroid Hormones", "Paper II", "★★★★"],
["10", "Counter-Current Mechanism", "Paper II", "★★★★"],
];
const colW = [0.4, 3.8, 1.5, 1.5];
const colX = [0.18, 0.62, 4.5, 6.1];
const rowH = 0.41;
const startY = 0.9;
// Header row
const headers = ["#", "Topic", "Paper", "Frequency"];
headers.forEach((h, i) => {
slide.addShape(pres.shapes.RECTANGLE, { x: colX[i], y: startY, w: colW[i] !== 0.4 ? (i === 1 ? 3.8 : 1.45) : 0.4, h: rowH, fill: { color: C.blue }, line: { color: C.navy } });
slide.addText(h, { x: colX[i], y: startY, w: colW[i] !== 0.4 ? (i === 1 ? 3.8 : 1.45) : 0.4, h: rowH, fontSize: 11, color: C.white, bold: true, align: "center", valign: "middle" });
});
topics.forEach((row, ri) => {
const y = startY + rowH + ri * rowH;
const bg = ri % 2 === 0 ? C.white : C.light;
row.forEach((cell, ci) => {
const w = ci === 1 ? 3.8 : (ci === 0 ? 0.4 : 1.45);
slide.addShape(pres.shapes.RECTANGLE, { x: colX[ci], y, w, h: rowH, fill: { color: bg }, line: { color: C.light } });
const isGold = ci === 3;
slide.addText(cell, {
x: colX[ci], y, w, h: rowH,
fontSize: ci === 0 ? 12 : 10,
color: isGold ? C.teal : (ci === 0 ? C.navy : C.darkGray),
bold: ci === 0 || ci === 3,
align: "center", valign: "middle",
});
});
});
}
// ============================================================
// HELPER: create a topic slide
// ============================================================
function addTopicSlide(pres, num, title, paper, freq, keyPoints, mustInclude, clinicalNote, accentColor) {
let slide = pres.addSlide();
// Background
slide.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offWhite }, line: { color: C.offWhite } });
// Left sidebar
slide.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 2.3, h: 5.625, fill: { color: C.navy }, line: { color: C.navy } });
slide.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.12, h: 5.625, fill: { color: accentColor }, line: { color: accentColor } });
// Number in circle
slide.addShape(pres.shapes.ELLIPSE, { x: 0.5, y: 0.3, w: 1.2, h: 1.2, fill: { color: accentColor }, line: { color: accentColor } });
slide.addText(`${num}`, { x: 0.5, y: 0.3, w: 1.2, h: 1.2, fontSize: 42, color: C.navy, bold: true, align: "center", valign: "middle" });
// Paper badge
slide.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 0.25, y: 1.7, w: 1.75, h: 0.38, fill: { color: accentColor }, line: { color: accentColor }, rectRadius: 0.08 });
slide.addText(paper, { x: 0.25, y: 1.7, w: 1.75, h: 0.38, fontSize: 10, color: C.navy, bold: true, align: "center", valign: "middle" });
// Frequency
slide.addText("Frequency", { x: 0.12, y: 2.2, w: 2.1, h: 0.3, fontSize: 9, color: C.gray, align: "center" });
slide.addText(freq, { x: 0.12, y: 2.45, w: 2.1, h: 0.35, fontSize: 13, color: C.gold, bold: true, align: "center" });
// MUST INCLUDE label
slide.addText("MUST INCLUDE:", { x: 0.12, y: 3.05, w: 2.1, h: 0.3, fontSize: 9, color: C.gold, bold: true, align: "center" });
slide.addText(mustInclude, {
x: 0.12, y: 3.35, w: 2.08, h: 1.5,
fontSize: 8.5, color: C.light, align: "left", valign: "top", wrap: true,
});
// Right content area - Title
slide.addShape(pres.shapes.RECTANGLE, { x: 2.3, y: 0, w: 7.7, h: 0.7, fill: { color: C.blue }, line: { color: C.blue } });
slide.addShape(pres.shapes.RECTANGLE, { x: 2.3, y: 0, w: 0.08, h: 0.7, fill: { color: accentColor }, line: { color: accentColor } });
slide.addText(title.toUpperCase(), {
x: 2.5, y: 0, w: 7.3, h: 0.7,
fontSize: 20, color: C.white, bold: true, valign: "middle",
});
// Key points header
slide.addText("KEY POINTS TO COVER:", {
x: 2.45, y: 0.82, w: 7.2, h: 0.3,
fontSize: 10, color: C.blue, bold: true, charSpacing: 1,
});
// Key points
keyPoints.forEach((pt, i) => {
const y = 1.15 + i * 0.52;
slide.addShape(pres.shapes.RECTANGLE, { x: 2.45, y: y, w: 0.28, h: 0.32, fill: { color: accentColor }, line: { color: accentColor } });
slide.addText(`${i + 1}`, { x: 2.45, y: y, w: 0.28, h: 0.32, fontSize: 9, color: C.navy, bold: true, align: "center", valign: "middle" });
slide.addShape(pres.shapes.RECTANGLE, { x: 2.75, y: y, w: 6.9, h: 0.32, fill: { color: C.white }, line: { color: C.light } });
slide.addText(pt, { x: 2.85, y: y, w: 6.7, h: 0.32, fontSize: 10, color: C.darkGray, valign: "middle" });
});
// Clinical note
const clinY = 1.15 + keyPoints.length * 0.52 + 0.1;
slide.addShape(pres.shapes.RECTANGLE, { x: 2.45, y: clinY, w: 7.2, h: 0.72, fill: { color: "FEF9E7" }, line: { color: C.gold } });
slide.addShape(pres.shapes.RECTANGLE, { x: 2.45, y: clinY, w: 0.08, h: 0.72, fill: { color: C.gold }, line: { color: C.gold } });
slide.addText("🩺 Clinical Note: ", {
x: 2.6, y: clinY + 0.05, w: 2.2, h: 0.28,
fontSize: 9, color: C.red, bold: true,
});
slide.addText(clinicalNote, {
x: 2.6, y: clinY + 0.3, w: 7.0, h: 0.38,
fontSize: 9, color: C.darkGray, italic: true, wrap: true,
});
}
// ============================================================
// TOPIC SLIDES 1-10
// ============================================================
addTopicSlide(pres, 1, "Cardiac Cycle", "PAPER I", "★★★★★ (Asked 9 times)", [
"Definition: 0.8s at 72 bpm | Systole 0.3s, Diastole 0.5s",
"7 Phases (A-G): Atrial systole → IVC → Rapid ejection → Reduced ejection → IVR → Rapid filling → Diastasis",
"Pressure values: LV 120/0 mmHg, Aorta 120/80 mmHg, LA 5-8 mmHg",
"Volumes: EDV 130 mL, ESV 50 mL, SV ~70 mL, EF ~65%",
"Heart sounds: S1 (mitral closes), S2 (aortic closes), S3, S4",
"JVP waves: a (atrial), c (IVC), x descent, v wave, y descent",
], "Wiggers Diagram\n(Mandatory draw)\nDicrotic notch\nJVP correlation\nEffect of ↑HR",
"EF < 40% = Systolic heart failure. Dicrotic notch marks aortic valve closure on aortic pressure trace.", C.gold);
addTopicSlide(pres, 2, "Electrocardiogram (ECG)", "PAPER I", "★★★★★ (Asked 8 times)", [
"Definition: Recording of electrical activity | Einthoven's triangle, 12 leads",
"P wave: Atrial depolarization (0.1s, < 0.25 mV)",
"PR interval: AV conduction time (0.12–0.20s); QRS: Ventricular depolarization (0.06–0.10s)",
"ST segment: Isoelectric (plateau phase); T wave: Ventricular repolarization",
"QT interval: 0.35–0.44s (duration of ventricular systole)",
"AMI: ST elevation + pathological Q waves | Heart block: prolonged PR",
], "Draw Lead II ECG\n(Mandatory)\nLabel all waves\nMark intervals\nClinical changes",
"ST elevation = STEMI. ST depression = NSTEMI / ischemia. Peaked T wave = hyperkalemia.", C.sky);
addTopicSlide(pres, 3, "Regulation of Respiration", "PAPER I", "★★★★★ (Asked 8 times)", [
"Respiratory centres: DRG (inspiration), VRG (expiration), Pneumotaxic (limits inspiration), Apneustic",
"Hering-Breuer reflex: Pulmonary stretch receptors via vagus → limits inspiration",
"Central chemoreceptors (ventral medulla): Respond to ↑CO₂ → ↑[H⁺] in CSF — most potent stimulus",
"Peripheral chemoreceptors (carotid + aortic body): ↓PO₂ < 60 mmHg, ↑PCO₂, ↓pH",
"CO₂ response curve vs O₂ response curve (draw both)",
"Exercise regulation: Neural (central command + proprioceptors) + Chemical (↑CO₂, ↑H⁺)",
], "Neural centres diagram\nChemoreceptor table\nCO₂ response curve\nCheyne-Stokes pattern",
"Cheyne-Stokes breathing = alternating hyperpnea + apnea; seen in heart failure, brainstem lesions. COPD patients rely on hypoxic drive.", C.teal);
addTopicSlide(pres, 4, "Mechanism of Muscle Contraction", "PAPER I", "★★★★ (Asked 7 times)", [
"Sarcomere structure: A band (constant), I band + H zone (shorten); Z line, M line",
"Proteins: Actin (thin), Myosin (thick), Troponin complex (TnT, TnI, TnC), Tropomyosin",
"Sliding filament theory (Huxley & Hanson 1954): Filaments slide; no change in length",
"Cross-bridge cycle: ATP → ADP+Pi (energizes myosin) → Power stroke → Detachment (new ATP)",
"E-C coupling: AP → T-tubule → DHP receptor → RYR → Ca²⁺ from SR → binds TnC → exposes actin",
"Relaxation: SERCA pump returns Ca²⁺ to SR | Length-tension relationship (inverted U curve)",
], "Labeled sarcomere diagram\n(Mandatory)\nCross-bridge cycle\nE-C coupling steps\nLength-tension graph",
"Rigor mortis: ATP depletion → permanent cross-bridge attachment. Myasthenia gravis: autoantibodies against AChR at NMJ.", C.gold);
addTopicSlide(pres, 5, "Cardiac Output & Its Regulation", "PAPER I", "★★★★ (Asked 7 times)", [
"CO = HR × SV = 5–5.5 L/min; Cardiac Index = CO/BSA = 3.2 L/min/m²",
"Fick's Principle: CO = O₂ consumption / (AO₂ – VO₂); Dye dilution method",
"Frank-Starling Law: ↑EDV → ↑SV (preload); Draw Starling curves",
"Preload (venous return, blood volume) | Afterload (aortic pressure, TPR)",
"Contractility: ↑ by catecholamines, Ca²⁺, digitalis | ↓ by β-blockers, acidosis",
"Bainbridge reflex (↑venous return → ↑HR) | Bezold-Jarisch reflex",
], "Fick principle formula\nStarling curves\nPreload/afterload table\nVenous return curve",
"In heart failure: CO ↓, EDV ↑ (dilated), Starling curve shifts downward. Ejection fraction is the most important clinical measure.", C.sky);
addTopicSlide(pres, 6, "Pyramidal Tract (Corticospinal Tract)", "PAPER II", "★★★★★ (Asked 8 times)", [
"Origin: Motor cortex (area 4) 30%, Premotor cortex (area 6) 30%, Parietal cortex 40%",
"Course: Corona radiata → Internal capsule (post limb) → Cerebral peduncles → Pons → Medullary pyramid",
"Decussation: 85% cross at pyramidal decussation → Lateral CST; 15% uncrossed → Anterior CST",
"Termination: Alpha and gamma motor neurons of anterior horn (direct + via interneurons)",
"Function: Fine voluntary movements, especially skilled distal limb movements",
"UMN lesion: Spastic paralysis, ↑tone, ↑reflexes, Babinski +ve | LMN: Flaccid, ↓tone, fasciculations",
], "Trace the pathway diagram\nUMN vs LMN table\n(mandatory in SCB)\nBabinski sign\nInternal capsule lesion",
"Stroke (MCA territory): Contralateral spastic hemiplegia + Babinski sign. Bell's palsy = LMN facial nerve palsy.", C.teal);
addTopicSlide(pres, 7, "Cerebellum", "PAPER II", "★★★★★ (Asked 7 times)", [
"Anatomical: Anterior lobe, Posterior lobe (primary fissure), Flocculonodular lobe (posterolateral fissure)",
"Functional: Vestibulocerebellum (balance), Spinocerebellum (coordination, tone), Cerebrocerebellum (planning)",
"Deep nuclei (medial→lateral): Fastigial, Emboliform, Globose, Dentate (mnemonic: FEGD)",
"Afferents: Spinocerebellar (proprioception), Corticopontocerebellar, Vestibulocerebellar",
"Efferents: Dentate nucleus → thalamus → motor cortex via superior cerebellar peduncle",
"Cerebellar lesions (ipsilateral): DANISH — Dysdiadochokinesia, Ataxia, Nystagmus, Intention tremor, Speech, Hypotonia",
], "Functional divisions diagram\nDANISH mnemonic\n(1 mark each sign)\nCerebellar gait\nPeduncle connections",
"Cerebellar ataxia = wide-based gait, positive Romberg test (falls with eyes open too). Intention tremor worsens on reaching target.", C.gold);
addTopicSlide(pres, 8, "Nephron / GFR and Its Regulation", "PAPER II", "★★★★★ (Asked 7 times)", [
"Nephron structure: Renal corpuscle, PCT, Loop of Henle (juxtamedullary vs cortical), DCT, collecting duct",
"Filtration membrane: Fenestrated endothelium + GBM (heparan sulfate) + podocytes with filtration slits",
"GFR = 125 mL/min (180 L/day filtered, ~1.5 L excreted); Filtration fraction = 20%",
"Net filtration pressure = (55–15) – (30–0) = 10 mmHg (Starling's forces at glomerulus)",
"Autoregulation: Myogenic + Tubuloglomerular feedback via macula densa (80–180 mmHg range)",
"RAAS: Angiotensin II → efferent constriction → maintains GFR when BP falls",
], "Nephron labeled diagram\nStarling forces at\nglomerulus (table)\nAutoregulation curve\nInulin vs PAH clearance",
"Inulin clearance = GFR (freely filtered only). PAH clearance = RPF. Nephrotic syndrome: heavy proteinuria (>3.5 g/day) due to GBM damage.", C.sky);
addTopicSlide(pres, 9, "Thyroid Hormones", "PAPER II", "★★★★ (Asked 6 times)", [
"Synthesis steps: Iodide trapping (NIS) → TPO oxidation → Organification → MIT+DIT coupling → Thyroglobulin storage",
"T4:T3 = 4:1 secreted; T3 is 3–5× more potent; peripheral conversion of T4→T3 by deiodinase",
"Transport: 99.9% protein-bound (TBG > albumin); only free hormone is active",
"Actions: ↑BMR (calorigenic), growth/development, ↑HR/CO, ↑GI motility, metabolic effects",
"Regulation: TRH → TSH → T3/T4; Negative feedback on hypothalamus and pituitary",
"Cretinism: Hypothyroidism in infancy → mental retardation, dwarfism, coarse features, umbilical hernia",
], "Synthesis pathway\ndiagram (step-wise)\nHypothyroidism vs\nHyperthyroidism table\nRegulation axis diagram",
"TSH is the single best test for thyroid function. Cretinism is prevented by neonatal TSH screening. Graves disease = TSH-receptor antibodies.", C.teal);
addTopicSlide(pres, 10, "Counter-Current Mechanism", "PAPER II", "★★★★ (Asked 6 times)", [
"Purpose: Concentrate urine up to 1200 mOsm/kg using medullary hyperosmolarity gradient",
"Counter-current multiplier (Loop of Henle): Ascending limb impermeable to water, actively transports NaCl out",
"Counter-current exchanger (Vasa recta): Maintains medullary gradient; hairpin capillary arrangement",
"Urea recycling: ADH-dependent collecting duct reabsorbs urea → inner medullary osmolarity",
"ADH (Vasopressin): V2 receptor → cAMP → AQP2 insertion in collecting duct → concentrated urine",
"Without ADH: Dilute urine (50–100 mOsm/kg) → Diabetes insipidus (central vs nephrogenic)",
], "Medullary gradient diagram\n(cortex to inner medulla)\nLoop of Henle: selective\npermeability summary\nADH mechanism",
"ADH released from posterior pituitary. Central DI = ADH deficiency → treat with desmopressin. Nephrogenic DI = ADH resistance (lithium toxicity).", C.gold);
// ============================================================
// SLIDE 13 - PRIORITY CHEAT SHEET
// ============================================================
{
let slide = pres.addSlide();
slide.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy }, line: { color: C.navy } });
slide.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.12, h: 5.625, fill: { color: C.gold }, line: { color: C.gold } });
slide.addText("EXAM PRIORITY CHEAT SHEET", {
x: 0.3, y: 0.15, w: 9.5, h: 0.55,
fontSize: 20, color: C.gold, bold: true, align: "center", charSpacing: 2,
});
// Paper I box
slide.addShape(pres.shapes.RECTANGLE, { x: 0.3, y: 0.85, w: 4.4, h: 4.3, fill: { color: C.blue }, line: { color: C.sky } });
slide.addShape(pres.shapes.RECTANGLE, { x: 0.3, y: 0.85, w: 4.4, h: 0.45, fill: { color: C.sky }, line: { color: C.sky } });
slide.addText("PAPER I", { x: 0.3, y: 0.85, w: 4.4, h: 0.45, fontSize: 13, color: C.white, bold: true, align: "center", valign: "middle" });
const p1 = [
"1. Cardiac Cycle ★★★★★",
"2. ECG ★★★★★",
"3. Regulation of Respiration ★★★★★",
"4. Mechanism of Muscle Contraction ★★★★",
"5. Cardiac Output ★★★★",
" + Blood Coagulation",
" + Lung Volumes & Capacities",
" + Action Potential",
];
p1.forEach((t, i) => {
const isMust = i < 5;
slide.addText(t, {
x: 0.5, y: 1.42 + i * 0.42, w: 4.0, h: 0.38,
fontSize: 10.5, color: isMust ? C.gold : C.light,
bold: isMust,
});
});
// Paper II box
slide.addShape(pres.shapes.RECTANGLE, { x: 5.3, y: 0.85, w: 4.4, h: 4.3, fill: { color: C.blue }, line: { color: C.teal } });
slide.addShape(pres.shapes.RECTANGLE, { x: 5.3, y: 0.85, w: 4.4, h: 0.45, fill: { color: C.teal }, line: { color: C.teal } });
slide.addText("PAPER II", { x: 5.3, y: 0.85, w: 4.4, h: 0.45, fontSize: 13, color: C.white, bold: true, align: "center", valign: "middle" });
const p2 = [
"6. Pyramidal Tract ★★★★★",
"7. Cerebellum ★★★★★",
"8. Nephron / GFR ★★★★★",
"9. Thyroid Hormones ★★★★",
"10. Counter-Current Mechanism ★★★★",
" + Basal Ganglia + Parkinsonism",
" + RAAS / Aldosterone",
" + Menstrual Cycle",
];
p2.forEach((t, i) => {
const isMust = i < 5;
slide.addText(t, {
x: 5.5, y: 1.42 + i * 0.42, w: 4.0, h: 0.38,
fontSize: 10.5, color: isMust ? C.gold : C.light,
bold: isMust,
});
});
}
// ============================================================
// SLIDE 14 - EXAM WRITING TIPS
// ============================================================
{
let slide = pres.addSlide();
slide.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offWhite }, line: { color: C.offWhite } });
slide.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 0.7, fill: { color: C.navy }, line: { color: C.navy } });
slide.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.12, h: 5.625, fill: { color: C.gold }, line: { color: C.gold } });
slide.addText("HOW TO WRITE A PERFECT 15-MARK ANSWER", {
x: 0.3, y: 0, w: 9.5, h: 0.7,
fontSize: 16, color: C.white, bold: true, align: "center", valign: "middle",
});
const tips = [
{ icon: "📝", title: "Structure (2 min planning)", text: "Start with Definition → Diagram → Steps/Mechanism → Regulation → Clinical Significance" },
{ icon: "🖊️", title: "Draw Diagrams", text: "Always draw labeled diagrams — examiners at SCB/VIMSAR give 3-4 marks for diagrams alone, even if text is incomplete" },
{ icon: "🔢", title: "Use Exact Numbers", text: "Quote precise values: pressures (mmHg), volumes (mL), durations (s), normal ranges — each correct value is a mark" },
{ icon: "📊", title: "Use Tables for Comparisons", text: "UMN vs LMN, Hypothyroid vs Hyperthyroid, Type 1 vs Type 2 — tables score full marks and save time" },
{ icon: "🏥", title: "Clinical Note (Mandatory)", text: "Always end with 2-3 lines of clinical significance — 2 marks are typically reserved for this in Odisha papers" },
{ icon: "⏱️", title: "Time Management", text: "Allocate 15 min per 15-mark question. Spend 3 min on diagram, 10 min on content, 2 min on clinical note" },
];
tips.forEach((t, i) => {
const col = i < 3 ? 0 : 1;
const row = i % 3;
const x = col === 0 ? 0.3 : 5.3;
const y = 0.88 + row * 1.52;
slide.addShape(pres.shapes.RECTANGLE, {
x, y, w: 4.6, h: 1.38,
fill: { color: C.white }, line: { color: C.light },
shadow: { type: "outer", color: "000000", blur: 6, offset: 2, angle: 135, opacity: 0.08 }
});
slide.addShape(pres.shapes.RECTANGLE, { x, y, w: 0.08, h: 1.38, fill: { color: C.sky }, line: { color: C.sky } });
slide.addText(`${t.icon} ${t.title}`, {
x: x + 0.18, y: y + 0.1, w: 4.3, h: 0.32,
fontSize: 10.5, color: C.navy, bold: true,
});
slide.addText(t.text, {
x: x + 0.18, y: y + 0.42, w: 4.3, h: 0.86,
fontSize: 9.5, color: C.darkGray, wrap: true,
});
});
}
// ============================================================
// SLIDE 15 - CLOSING SLIDE
// ============================================================
{
let slide = pres.addSlide();
slide.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy }, line: { color: C.navy } });
slide.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.12, h: 5.625, fill: { color: C.gold }, line: { color: C.gold } });
slide.addShape(pres.shapes.RECTANGLE, { x: 9.88, y: 0, w: 0.12, h: 5.625, fill: { color: C.gold }, line: { color: C.gold } });
// Decorative line
slide.addShape(pres.shapes.RECTANGLE, { x: 1.5, y: 2.55, w: 7, h: 0.04, fill: { color: C.sky }, line: { color: C.sky } });
slide.addText("BEST OF LUCK!", {
x: 0.5, y: 0.9, w: 9, h: 0.9,
fontSize: 50, color: C.gold, bold: true, align: "center",
});
slide.addText("FOR YOUR ODISHA MBBS EXAMS", {
x: 0.5, y: 1.75, w: 9, h: 0.5,
fontSize: 18, color: C.white, align: "center", charSpacing: 3,
});
slide.addText('"The secret of getting ahead is getting started."', {
x: 1, y: 2.75, w: 8, h: 0.55,
fontSize: 14, color: C.light, italic: true, align: "center",
});
slide.addText("Prepare Smart · Draw Diagrams · Include Clinical Notes · Mention Exact Values", {
x: 0.5, y: 3.55, w: 9, h: 0.45,
fontSize: 11, color: C.gray, align: "center",
});
slide.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 3, y: 4.3, w: 4, h: 0.6,
fill: { color: C.teal }, line: { color: C.teal }, rectRadius: 0.1,
});
slide.addText("SCB · VIMSAR · Hi-Tech · SLN", {
x: 3, y: 4.3, w: 4, h: 0.6,
fontSize: 12, color: C.white, bold: true, align: "center", valign: "middle",
});
}
// ============================================================
// SAVE
// ============================================================
pres.writeFile({ fileName: "/home/daytona/workspace/odisha-physiology-pptx/Odisha_MBBS_Physiology_Top10.pptx" })
.then(() => console.log("✅ PPTX created successfully!"))
.catch(err => console.error("❌ Error:", err));
cd /home/daytona/workspace/odisha-physiology-pptx && node create_pptx.js
node -e "const p = require('pptxgenjs'); const pr = new p(); console.log(Object.…
sed -i 's/pres\.shapes\.ELLIPSE/pres.shapes.OVAL/g' /home/daytona/workspace/odis…
~/odisha-physiology-pptx/create_pptx.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/odisha-physiology-pptx/create_pptx.js'
cd /home/daytona/workspace/odisha-physiology-pptx && node create_pptx.js
ls -lh /home/daytona/workspace/odisha-physiology-pptx/Odisha_MBBS_Physiology_Top…
Odisha MBBS Physiology Top10
Presentation · PPTX
| Slide | Content |
|---|---|
| 1 | Title slide - "Top 10 Physiology Topics - Odisha MBBS Exam" |
| 2 | Overview table - all 10 topics with paper and frequency ratings |
| 3 | Topic 1: Cardiac Cycle (★★★★★) |
| 4 | Topic 2: ECG (★★★★★) |
| 5 | Topic 3: Regulation of Respiration (★★★★★) |
| 6 | Topic 4: Mechanism of Muscle Contraction (★★★★) |
| 7 | Topic 5: Cardiac Output (★★★★) |
| 8 | Topic 6: Pyramidal Tract + UMN vs LMN (★★★★★) |
| 9 | Topic 7: Cerebellum + DANISH signs (★★★★★) |
| 10 | Topic 8: Nephron / GFR (★★★★★) |
| 11 | Topic 9: Thyroid Hormones (★★★★) |
| 12 | Topic 10: Counter-Current Mechanism (★★★★) |
| 13 | Priority cheat sheet (Paper I vs Paper II split) |
| 14 | How to write a perfect 15-mark answer (6 tips) |
| 15 | Closing slide |
- Key Points to Cover (6 numbered points)
- Must Include sidebar (diagrams + mnemonics)
- Clinical Note (exam-scoring applied physiology)