Create a clinical case with a diagnosis of acute or chronic tubulointerstitial nephritis
Reading File
Checking Date & Time
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
tubulointerstitial nephritis histology interstitial inflammation eosinophils
Loading Image
Loading Image
I now have all the information needed to create a comprehensive, well-structured clinical case. Here it is:
Clinical Case: Acute Drug-Induced Tubulointerstitial Nephritis
📋 Patient Presentation
Patient: M.R., 58-year-old male
Chief complaint: Decreased urine output, flank pain, and skin rash for 5 days
🩺 History of Present Illness
M.R. presents to the nephrology clinic with a 5-day history of progressive oliguria, bilateral flank tenderness, and a diffuse maculopapular rash on the trunk and upper extremities. He reports low-grade fever (38.1°C) and general malaise. Three weeks prior, he was started on omeprazole (a proton pump inhibitor) for newly diagnosed gastroesophageal reflux disease, and approximately 10 days ago his physician added sulfamethoxazole/trimethoprim for a urinary tract infection.
He denies dysuria at this point, flank trauma, or prior kidney disease. He takes no NSAIDs or other nephrotoxic agents.
🗂️ Past Medical History
- Hypertension (well-controlled on amlodipine)
- GERD (recently diagnosed)
- No history of kidney disease, diabetes, or autoimmune disorders
💊 Medications
| Medication | Duration |
|---|---|
| Amlodipine 5 mg/day | Chronic |
| Omeprazole 20 mg/day | 3 weeks |
| Sulfamethoxazole/trimethoprim | 10 days |
🔬 Physical Examination
- Vital signs: T 38.1°C, BP 148/90 mmHg, HR 92 bpm, RR 16/min, SpO₂ 98% on room air
- General: Alert, mildly distressed
- Skin: Diffuse maculopapular rash on trunk and arms (present in ~25% of cases)
- Abdomen: Bilateral costovertebral angle tenderness on palpation (tender kidneys)
- Cardiovascular/Respiratory: Normal
- No peripheral edema (glomeruli are spared)
🧪 Laboratory Results
| Test | Result | Reference |
|---|---|---|
| Serum creatinine | 4.2 mg/dL (↑ from baseline 1.0) | 0.7–1.2 mg/dL |
| BUN | 58 mg/dL | 7–20 mg/dL |
| eGFR | 15 mL/min/1.73m² | >60 |
| WBC | 13,500/µL | 4,500–11,000 |
| Eosinophils | 12% (absolute: 1,620/µL) | <500/µL |
| Serum IgE | Elevated | — |
| Na⁺ / K⁺ | 138 / 5.6 mEq/L | — |
| HCO₃⁻ | 17 mEq/L (↓) | 22–26 mEq/L |
| Serum Ca²⁺ | Normal | — |
| Urine output | 320 mL/day (oliguria) | >400 mL/day |
🧫 Urinalysis & Urine Sediment
| Finding | Result |
|---|---|
| Protein | Trace (non-nephrotic) |
| Hematuria | + (microscopic) |
| Leukocyturia (WBC casts) | Present |
| Eosinophiluria | Present (Giemsa-stained cytocentrifuged specimen) |
| Granular casts | Absent |
| Urine culture | Negative |
Interpretation: The combination of pyuria with WBC casts and eosinophiluria — in the absence of bacteriuria — is the hallmark of acute allergic tubulointerstitial nephritis (ATIN). Absence of nephrotic-range proteinuria distinguishes this from glomerular disease.
🖼️ Renal Biopsy — Histopathology
Renal biopsy was performed given the severity of AKI and unclear timeline.
FIG. 1 — Drug-Induced Tubulointerstitial Nephritis (H&E stain)
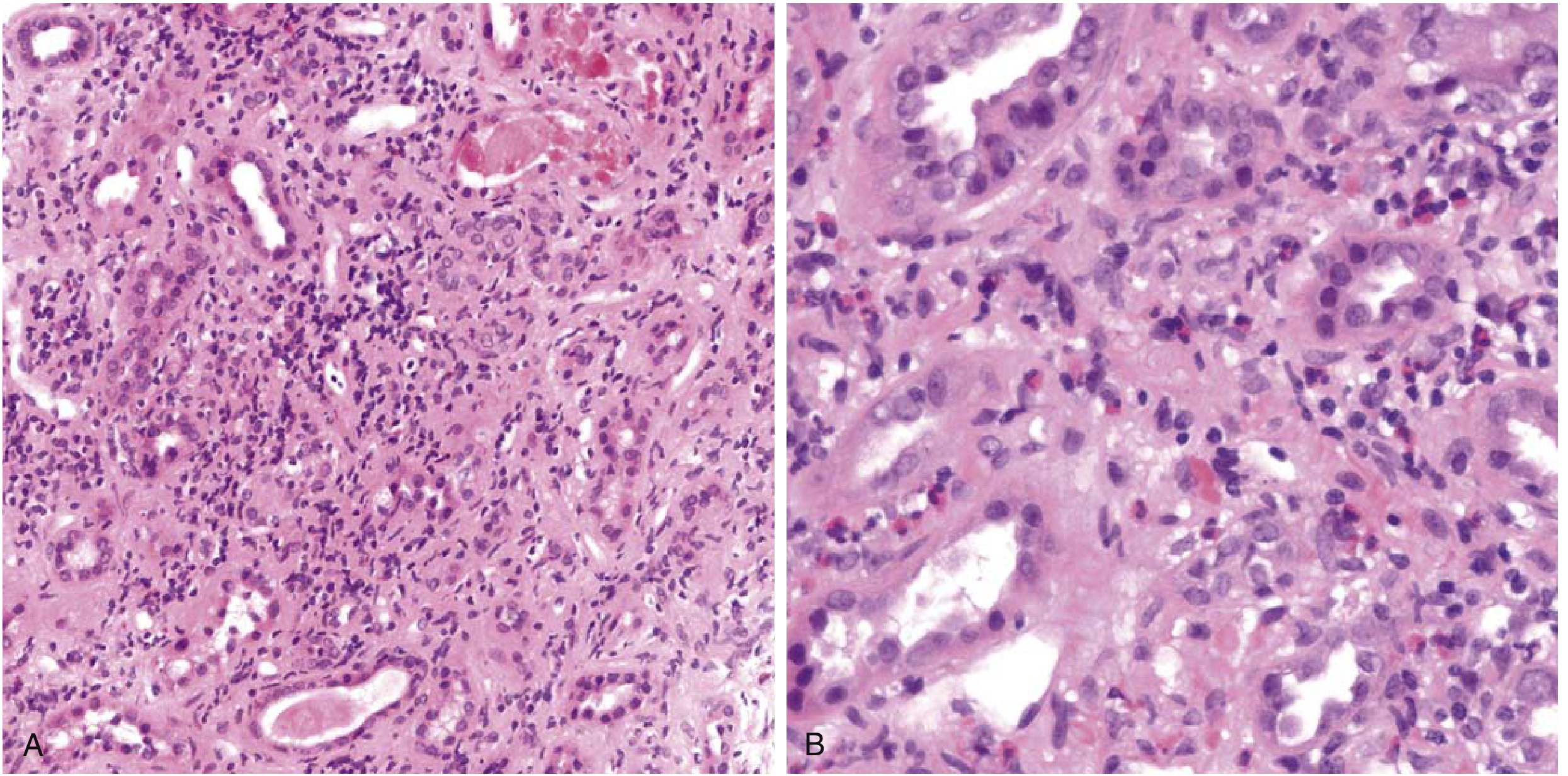
FIG. 1 — Drug-induced tubulointerstitial nephritis. (A) Interstitial edema with dense mononuclear infiltrate (lymphocytes and macrophages) and tubular injury. (B) High-power view showing a prominent eosinophilic infiltrate characteristic of hypersensitivity reaction. Glomeruli appear normal. — Robbins & Kumar Basic Pathology
Histological findings:
- Interstitial edema and dense infiltration by lymphocytes, macrophages, and eosinophils
- Tubulitis (lymphocytes invading tubular epithelium)
- Normal glomeruli (no nephritic or nephrotic changes)
- No granuloma formation (granulomas may appear with thiazides or rifampin)
FIG. 2 — Acute Tubulointerstitial Nephritis (H&E stain, renal cortex)
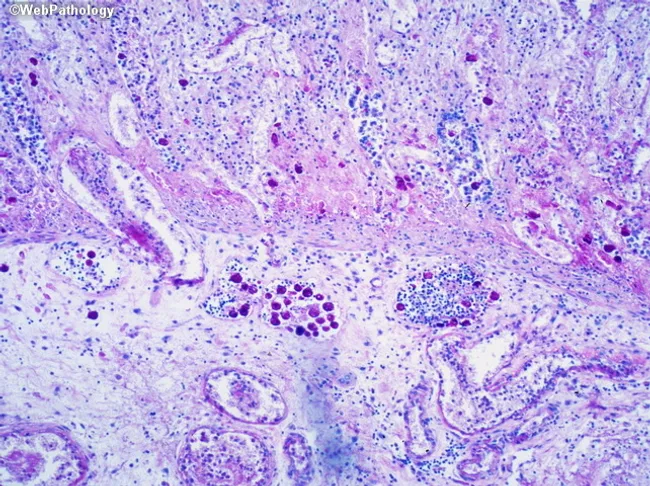
FIG. 2 — Renal cortex biopsy demonstrating diffuse interstitial inflammatory infiltrate (lymphocytes, plasma cells, scattered eosinophils), peritubular inflammation with tubulitis, and relatively preserved glomerular architecture — consistent with acute tubulointerstitial nephritis.
🔍 Pathogenesis
The most likely sequence of events in this patient:
- Omeprazole and/or SMX-TMP are secreted by tubular cells and covalently bind to cytoplasmic or extracellular tubular components, creating immunogenic neoantigens
- Two concurrent hypersensitivity mechanisms operate:
- Type I (immediate): Elevated IgE → eosinophilia, rash
- Type IV (delayed, cell-mediated): T lymphocyte infiltration → tubular injury and interstitial inflammation
- The reaction is idiosyncratic (not dose-dependent), explaining why most patients tolerate these drugs
- Re-exposure triggers a faster anamnestic response (1 day vs. 1–2 weeks on first exposure)
PPIs are among the most common causes of ATIN and may also potentiate ATIN risk in patients concurrently taking immune checkpoint inhibitors. — Harrison's Principles of Internal Medicine, 22E
🧠 Differential Diagnosis
| Diagnosis | Argument For | Argument Against |
|---|---|---|
| Acute TIN (drug-induced) ✅ | Fever, rash, eosinophilia, recent drug exposure, WBC/eosinophil casts, non-nephrotic proteinuria, biopsy findings | — |
| Acute pyelonephritis | Fever, flank pain, pyuria | Negative urine culture, no bacteriuria, eosinophiluria |
| Acute tubular injury (ATI) | AKI, oliguria | No granular casts, no hypotension/nephrotoxin, eosinophiluria present |
| Glomerulonephritis | Rising Cr | Absent nephritic/nephrotic syndrome, normal glomeruli on biopsy |
| NSAID-induced minimal change | WBC casts, proteinuria | No NSAID use, biopsy shows no podocyte effacement |
✅ Final Diagnosis
Acute allergic (drug-induced) tubulointerstitial nephritis (ATIN), most likely caused by sulfamethoxazole and/or omeprazole, presenting as AKI with oliguria, fever, rash, eosinophilia, and eosinophiluria.
💊 Management
| Step | Action |
|---|---|
| 1. Immediate withdrawal of offending drugs | Discontinue SMX-TMP and omeprazole |
| 2. Supportive care | Fluid management, electrolyte correction (hyperkalemia, metabolic acidosis) |
| 3. Corticosteroids | Prednisone 1 mg/kg/day × 2–4 weeks (evidence supports earlier steroid use in severe or unresponsive cases) |
| 4. Renal replacement therapy | Hemodialysis if severe uremia, refractory hyperkalemia, or fluid overload |
| 5. Monitoring | Serial creatinine, urine output, urinalysis weekly until recovery |
| 6. Alternative medications | Switch to H₂ blocker (e.g., famotidine) for GERD; alternative antibiotic for UTI if needed |
Clinical recognition is imperative: withdrawal of the offending drug is followed by recovery, though it may take several months for renal function to return to normal. Recovery is incomplete in approximately 40% of cases, particularly in older patients or when diagnosis is delayed. — Robbins & Kumar Basic Pathology
📊 Expected Clinical Course
- Creatinine should begin to decline within 1–2 weeks of drug withdrawal
- Full recovery in ~60% of cases; partial recovery or progression to chronic TIN in ~40%
- Recurrence is likely if the same or structurally similar drug is reintroduced
📚 Sources
- Robbins & Kumar Basic Pathology — Drug-Induced Tubulointerstitial Nephritis, p. 518
- Robbins, Cotran & Kumar Pathologic Basis of Disease — Tubulointerstitial Nephritis, p. 862
- Harrison's Principles of Internal Medicine 22E (2025) — Acute Tubulointerstitial Nephritis, Chapter 319
Make a ppt only on case
Reading File
Reading File
Reading File
Running Command
ls -la /home/daytona/workspace/ 2>/dev/null || echo "workspace empty or missing"
Running Command
mkdir -p /home/daytona/workspace/tin-case-ppt
Running Command
node /home/daytona/skills/shared/scripts/fetch_images.js "https://cdn.orris.care/cdss_images/2ae13bc8e7c08035e047856674acf9869383d208997cf87931eb609970e5db9b.png" 2>&1 | head -5
!
Your input exceeds the context window of this model. Please adjust your input and try again.
We encountered an error while processing your request. Please try again or reach out to us for help.
This is a shared conversation. Sign in to Orris to start your own chat.