Pharmacological manage ment of stage 2 hypertension
Reading File
Finding Sources
Searching PubMed
"stage 2 hypertension" AND "pharmacological treatment"
Finding Sources
Searching PubMed
"hypertension" AND "antihypertensive" AND "combination therapy"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Finding Sources
Reading File
I now have everything needed for a thorough, well-illustrated answer. Let me compile the full response.
Pharmacological Management of Stage 2 Hypertension
Definition
Per the ACC/AHA 2017 guideline, Stage 2 hypertension is defined as a sustained SBP ≥ 140 mmHg and/or DBP ≥ 90 mmHg on two or more occasions. The European guideline (ESC/ESH) uses the same threshold. The treatment target is SBP/DBP < 130/80 mmHg in most adults.
Treatment Algorithm
The flowchart below summarizes BP threshold-based management, including the immediate dual-drug recommendation for Stage 2:
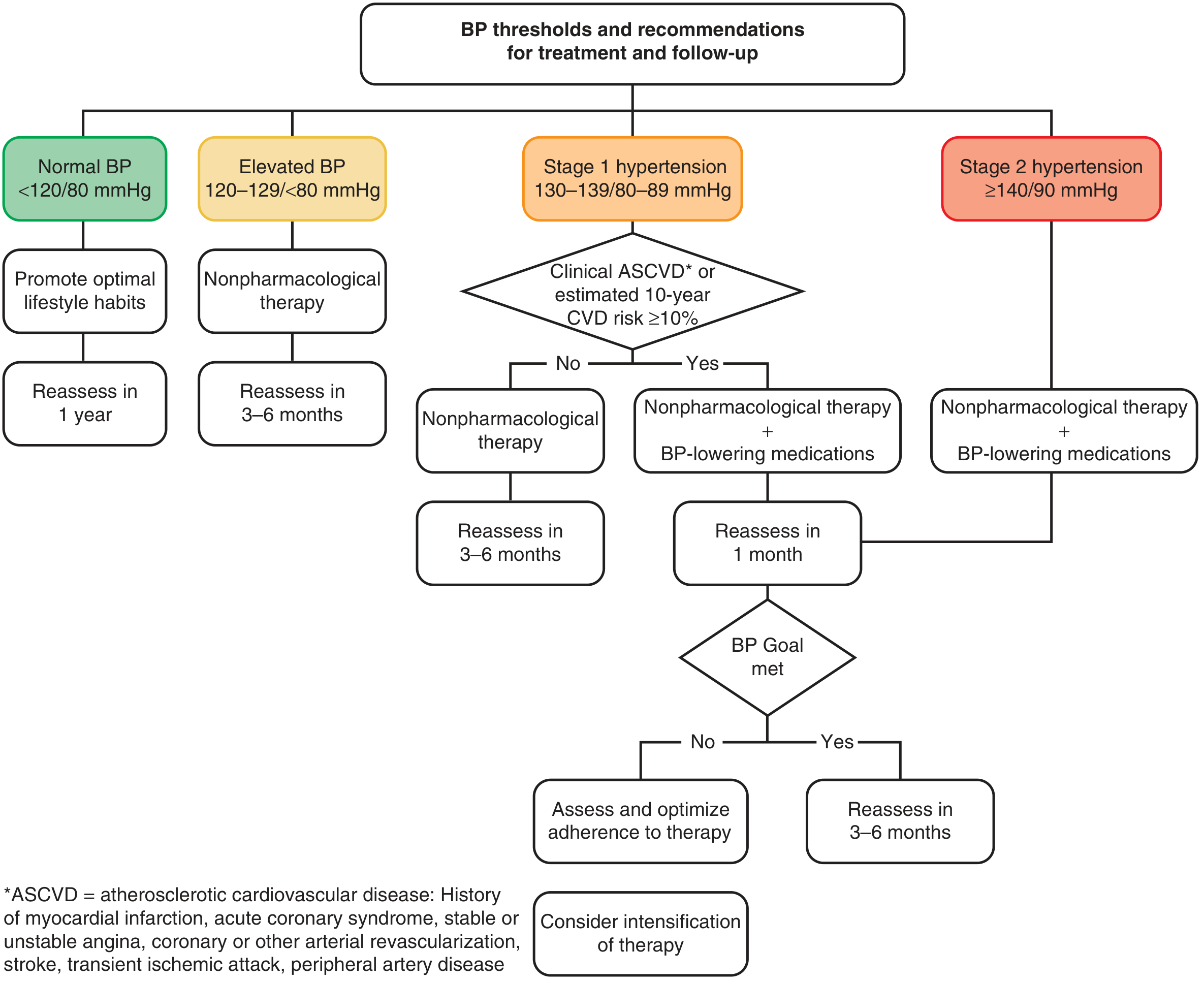
From Harrison's Principles of Internal Medicine, 22nd Ed.
And the step-by-step antihypertensive drug algorithm:
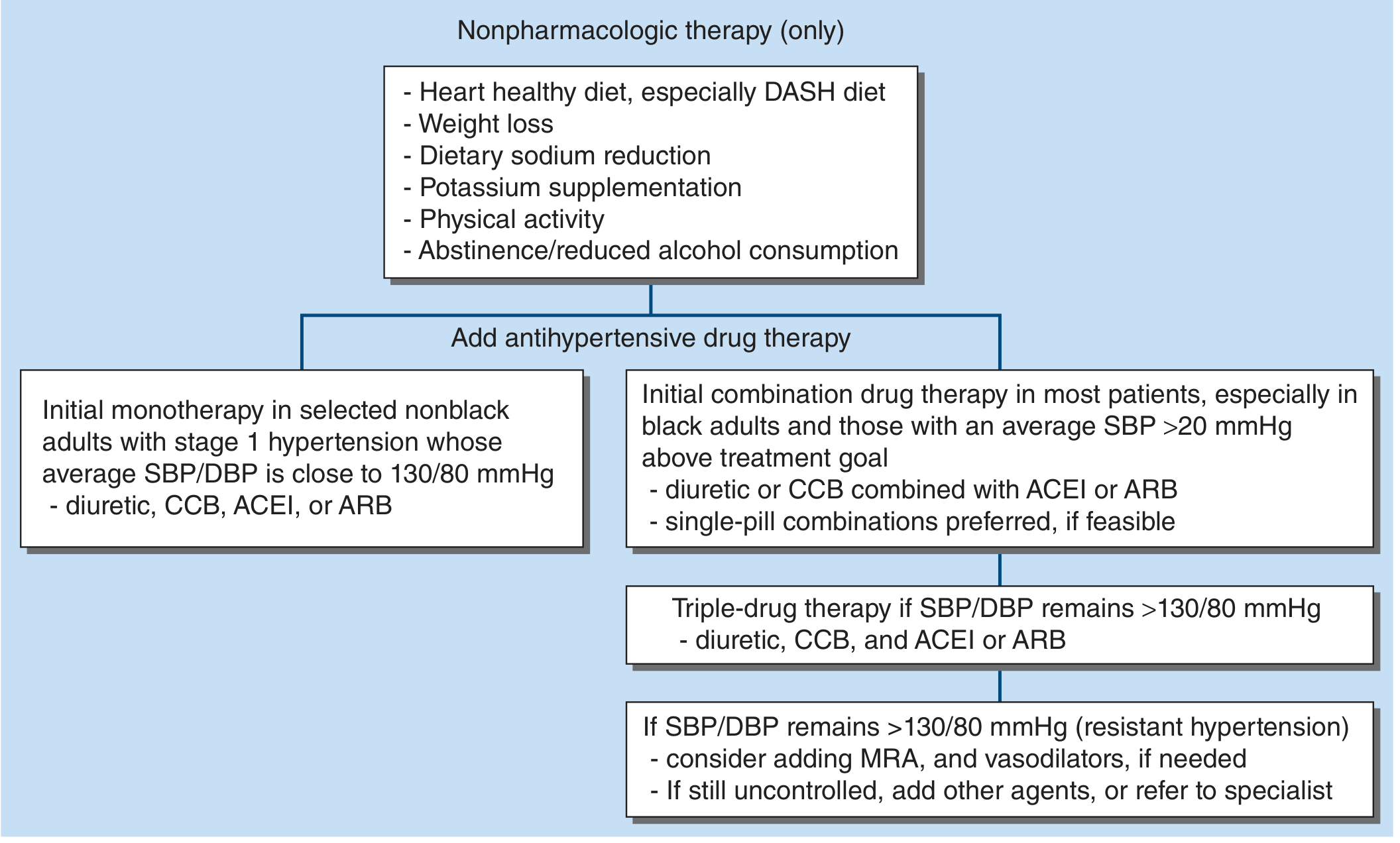
From Harrison's Principles of Internal Medicine, 22nd Ed.
Core Principle
Stage 2 hypertension requires pharmacological therapy in ALL patients, initiated simultaneously with nonpharmacologic measures. Unlike Stage 1, there is no option to defer drug therapy pending a lifestyle trial. Most patients need two-drug combination therapy from the outset, since the average SBP in Stage 2 is far above the treatment goal and a single agent rarely achieves the needed reduction. - Harrison's Principles of Internal Medicine, 22nd Ed.
First-Line Drug Classes (Without Compelling Indications)
The four first-line classes proven to prevent cardiovascular disease are:
| Drug Class | Preferred Agents | Usual Daily Dose | Key Mechanism |
|---|---|---|---|
| Thiazide/thiazide-like diuretics | Chlorthalidone (preferred), Indapamide, HCTZ | Chlorthalidone 12.5-25 mg OD | Volume depletion + vasodilation |
| ACE Inhibitors (ACEI) | Lisinopril, Ramipril, Enalapril | Lisinopril 10-40 mg OD | Block Ang II production → vasodilation |
| Angiotensin Receptor Blockers (ARB) | Losartan, Valsartan, Telmisartan | Losartan 50-100 mg OD | Block AT1 receptor |
| Calcium Channel Blockers (CCB) | Amlodipine (DHP), Diltiazem (non-DHP) | Amlodipine 5-10 mg OD | Vascular smooth muscle relaxation |
Beta-blockers are NOT recommended as first-line agents for uncomplicated hypertension - they are inferior to the above four classes, especially for stroke prevention. They retain a role when there are compelling indications (heart failure, post-MI, angina, AF rate control). - Harrison's Principles of Internal Medicine, 22nd Ed.
Initial Combination Strategy
For most patients with Stage 2 hypertension (SBP > 20 mmHg above goal):
Preferred initial regimen:
- Diuretic (chlorthalidone/indapamide) + CCB (amlodipine), or
- Diuretic + ACEI/ARB, or
- CCB + ACEI/ARB
Single-pill combinations (SPC) are preferred where available, as they improve adherence. ACEI and ARB should never be combined with each other (dual RAS blockade increases adverse events without additional BP benefit). - Goodman & Gilman's The Pharmacological Basis of Therapeutics
Hemodynamic Effects of Key Drug Classes
| Drug Class | Heart Rate | Cardiac Output | Total Peripheral Resistance | Plasma Volume |
|---|---|---|---|---|
| ACEI/ARB | ↔ | ↔ | ↓ | ↔ |
| CCB | ↓ or ↑ | ↔ | ↓ | ↔ |
| Thiazide diuretics | ↑ | ↓ | ↓ | ↓ |
| Beta-blockers | ↓ | ↓ | ↔ or ↓ | ↔ |
Special Populations - Compelling Indications
Certain comorbidities dictate drug selection regardless of BP stage:
| Comorbidity | Preferred Agent(s) |
|---|---|
| Diabetes mellitus / CKD with proteinuria | ACEI or ARB (preferred - slow renal progression) |
| Heart failure with reduced EF | ACEI or ARB + beta-blocker + MRA + diuretic |
| Post-MI / Ischemic heart disease | ACEI + beta-blocker |
| Atrial fibrillation (rate control) | Beta-blocker or non-DHP CCB (diltiazem/verapamil) |
| Stable angina | Beta-blocker or CCB |
| Pregnancy | Methyldopa, Labetalol, Nifedipine (NOT ACEI/ARB) |
| Black adults (without DM/CKD) | Thiazide diuretic or CCB (ACEI/ARB less effective as monotherapy) |
| Isolated systolic hypertension (elderly) | Thiazide diuretic or long-acting DHP-CCB |
- Harrison's Principles of Internal Medicine, 22nd Ed.; Goodman & Gilman's, Fuster and Hurst's The Heart
Stepwise Escalation
Step 1 (Stage 2): Nonpharmacologic therapy + TWO drugs (diuretic or CCB + ACEI/ARB)
↓ [Reassess in 1 month]
Step 2 (not at goal): TRIPLE therapy → diuretic + CCB + ACEI or ARB
↓
Step 3 (resistant HTN): Add MRA (e.g., spironolactone 25-50 mg) ± vasodilators
↓
Step 4 (refractory): Add alpha-blocker, centrally acting agent, or refer to specialist
Resistant hypertension = BP remains > 130/80 mmHg despite 3 drugs (including a diuretic), or requires ≥4 drugs. Before escalating, exclude: white coat effect, medication nonadherence, secondary causes (renal artery stenosis, primary aldosteronism, OSA, pheochromocytoma). - Harrison's Principles of Internal Medicine, 22nd Ed.
Drug-Specific Considerations
Diuretics
- Chlorthalidone and indapamide are preferred over HCTZ - longer half-life provides 24-hour BP coverage including nocturnal control, and most landmark U.S. trials used chlorthalidone.
- Watch for: hypokalemia, hyperuricemia, mild hyperglycemia, hyponatremia.
- Potassium-sparing agents (amiloride, triamterene) can be added to counter diuretic-induced hypokalemia. - Harrison's Principles of Internal Medicine, 22nd Ed.
ACEI
- Preferred in: diabetic nephropathy, CKD with proteinuria, post-MI, systolic HF.
- Main adverse effect: dry cough (5-20%, class effect due to bradykinin accumulation) - switch to ARB if this occurs.
- Contraindicated in: pregnancy, bilateral renal artery stenosis, angioedema history, hyperkalemia.
ARB
- Same indications as ACEI; use when ACEI-induced cough occurs.
- Side effects are rare; no angioedema or cough.
- Do not combine ACEI + ARB (dual RAS blockade increases risk of renal impairment and hyperkalemia). - Goodman & Gilman's The Pharmacological Basis of Therapeutics
CCB (dihydropyridines - amlodipine)
- Especially useful in: Black adults, elderly, isolated systolic HTN, angina, Raynaud's.
- Adverse effects: peripheral edema (especially at higher doses), flushing, reflex tachycardia.
- No metabolic adverse effects.
Non-DHP CCB (diltiazem, verapamil)
- Use for rate control in AF, angina.
- Avoid in HFrEF (negative inotropy).
- Do not combine with beta-blockers (risk of bradycardia/AV block).
Nonpharmacologic Therapy (Mandatory Adjunct)
Even with drug therapy, lifestyle modification must continue:
- DASH diet: reduces SBP by ~5 mmHg
- Sodium restriction (< 2.4 g/day): ~5 mmHg reduction
- Weight loss: ~1 mmHg per kg lost
- Aerobic exercise (30 min/day, 5 days/week): ~4-5 mmHg reduction
- Alcohol moderation: ≤2 drinks/day men, ≤1 drink/day women
- Smoking cessation (no direct BP effect but major CVD risk reduction)
Follow-Up
- Reassess in 1 month after initiating therapy for Stage 2 HTN.
- If BP goal is met, reassess every 3-6 months.
- If goal is not met, assess adherence, then intensify therapy.
- Home BP monitoring (HBPM) - 3 morning and 3 evening readings on 3 days prior to clinic visits - is recommended to guide management.
Key References:
- ACC/AHA 2017 Hypertension Guideline - Whelton et al.
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025), Chapter 288
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, Chapter 32
Note from recent literature: A 2024 meta-analysis (PMID 38532223) confirms fixed-dose combination therapy for cardiovascular prevention is effective; and a 2024 systematic review (PMID 38616212) highlights emerging drug strategies (renal denervation, novel mineralocorticoid antagonists) for resistant hypertension. A 2025 systematic review (PMID 41036884) reinforces that atenolol is inferior to other first-line agents and should not be used as first-line monotherapy for uncomplicated hypertension.
Used and adverse effects of Amlodipine
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"amlodipine" AND "adverse effects" AND "hypertension"
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
I have all the content needed. Here is the comprehensive answer:
Amlodipine - Uses and Adverse Effects
Drug Profile
| Property | Detail |
|---|---|
| Class | Dihydropyridine (DHP) calcium channel blocker (CCB) |
| Prototype | Amlodipine (also: nifedipine ER, felodipine, isradipine) |
| Route | Oral only |
| Dose | 2.5-10 mg once daily |
| Half-life | 30-50 hours (longest among CCBs - allows once-daily dosing) |
| Onset | Gradual (no sharp BP drop - reduces risk of reflex tachycardia compared to short-acting nifedipine) |
- Morgan and Mikhail's Clinical Anesthesiology, 7th Ed.
Mechanism of Action
Amlodipine blocks L-type voltage-gated calcium channels in vascular smooth muscle and cardiac muscle. This prevents calcium influx during depolarization, resulting in:
- Vascular smooth muscle relaxation → decreased peripheral vascular resistance → BP reduction
- Coronary artery vasodilation → increased oxygen supply to myocardium
- Minimal effect on cardiac conduction (AV node, SA node) - this distinguishes it from non-DHP CCBs like verapamil/diltiazem
Amlodipine functions primarily as an arteriolar vasodilator with very little negative inotropic or chronotropic effect at therapeutic doses. - Lippincott Illustrated Reviews: Pharmacology
Therapeutic Uses
1. Hypertension (Primary Use)
- A first-line antihypertensive - among the most prescribed drugs worldwide
- Particularly effective in:
- Black patients (good efficacy as monotherapy; RAS blockers are less effective alone in this population)
- Elderly patients with isolated systolic hypertension
- Patients with concurrent angina
- Patients with Raynaud's phenomenon (vasodilatory benefit)
- Used in Stage 2 HTN combination therapy: typically paired with an ACEI/ARB (CCB + ACEI/ARB is a preferred first-step combination)
- Long-acting DHP CCBs like amlodipine are among the first-choice agents in HTN per current guidelines - Goodman & Gilman's The Pharmacological Basis of Therapeutics
2. Angina Pectoris
a) Stable (effort-induced) angina:
- Reduces myocardial O2 demand by decreasing afterload (peripheral vasodilation)
- Reduces cardiac workload
b) Variant (Prinzmetal/vasospastic) angina:
- Highly effective - relaxes coronary artery spasm directly
- The vasodilatory effect of amlodipine is particularly useful in variant angina caused by spontaneous coronary spasm - Lippincott Illustrated Reviews: Pharmacology
3. Other Uses
- Coronary artery disease (CAD) - reduces anginal episodes
- Hypertensive urgency (oral, slower onset than IV agents but safe for subacute use)
- Hypertension in CKD - no dose adjustment needed; no nephrotoxicity
- Hypertension + Heart Failure with Preserved EF (HFpEF) - DHP CCBs are safe (unlike non-DHP CCBs)
Note: Short-acting dihydropyridines (sublingual nifedipine) should be avoided in CAD - evidence of increased mortality post-MI and increased risk of acute MI in hypertensive patients due to excessive reflex sympathetic activation. - Lippincott Illustrated Reviews: Pharmacology
Adverse Effects
Common (Vasodilation-Related)
| Adverse Effect | Mechanism | Notes |
|---|---|---|
| Peripheral/ankle edema | Arteriolar dilation → increased capillary hydrostatic pressure → fluid shift into interstitium | Most common side effect (5-15% of patients). Not due to sodium retention - calcium antagonists are actually natriuretic. Due to vasodilation with impaired venous return. Can be partially countered by adding an ACEI/ARB |
| Flushing | Cutaneous vasodilation | More common at initiation or dose increase; often subsides with time |
| Headache | Cerebral vasodilation | Usually transient |
| Reflex tachycardia | Drop in BP → baroreceptor-mediated sympathetic activation | Less common with amlodipine than with short-acting nifedipine, due to slow onset/long half-life |
| Dizziness / postural hypotension | Excessive BP lowering, especially in elderly | - Brenner & Rector's The Kidney, 2-Volume Set |
Less Common
| Adverse Effect | Notes |
|---|---|
| Gingival hyperplasia | Class effect of CCBs (also seen with nifedipine, cyclosporine, phenytoin). Reversible on stopping drug. |
| Palpitations | Due to reflex sympathetic stimulation |
| Nausea / abdominal pain | Uncommon; GI smooth muscle relaxation |
| Fatigue | Occasionally reported |
Rare but Notable
- Exacerbation of heart failure - amlodipine is relatively safe in HF compared to other CCBs, but high doses may worsen HF in some patients. The PRAISE trials found amlodipine did not increase mortality in HFrEF, unlike non-DHP CCBs.
- Drug interactions via CYP3A4 - amlodipine is a CYP3A4 substrate; levels may increase with CYP3A4 inhibitors (e.g., diltiazem, verapamil, erythromycin, grapefruit juice) and decrease with inducers (e.g., rifampin) - Goodman & Gilman's The Pharmacological Basis of Therapeutics
Key Pharmacological Comparison: DHP vs. Non-DHP CCBs
| Feature | Amlodipine (DHP) | Verapamil/Diltiazem (Non-DHP) |
|---|---|---|
| Main effect | Peripheral vasodilation | Vasodilation + ↓ HR + ↓ AV conduction |
| Heart rate | ↑ (reflex) or no change | ↓ (direct) |
| AV node | No significant effect | Slows conduction - useful for SVT/AF |
| Negative inotropy | Minimal | Significant |
| Use in HFrEF | Relatively safe | Contraindicated |
| Use with beta-blockers | Safe | Avoid (risk of bradycardia, heart block) |
| Angina type | Stable + vasospastic | Stable + vasospastic + rate control |
- Lippincott Illustrated Reviews: Pharmacology; Morgan and Mikhail's Clinical Anesthesiology, 7th Ed.
Contraindications and Cautions
| Contraindication | Reason |
|---|---|
| Severe aortic stenosis | Fixed obstruction - vasodilation can cause severe hypotension |
| Cardiogenic shock | Vasodilation worsens hemodynamics |
| Hypersensitivity to amlodipine or DHP CCBs | - |
| Caution in severe hepatic impairment | Extensive hepatic metabolism (start at 2.5 mg) |
| Pregnancy | Use only if benefit outweighs risk; generally avoided |
Amlodipine is safe in CKD - no dose adjustment required based on renal function. It does not cause hyperkalemia or worsen renal function.
Key Clinical Pearls
- Ankle edema from amlodipine can be reduced by combining it with an ACEI/ARB (venodilation counters the arteriolar-predominant vasodilation), rather than automatically stopping the drug or adding a diuretic.
- Because of its 30-50 hour half-life, amlodipine provides stable 24-hour BP coverage, making it excellent for once-daily dosing and reducing the risk of BP surges between doses.
- It is metabolically neutral - no effects on glucose, lipids, uric acid, or electrolytes. This distinguishes it from thiazide diuretics and beta-blockers.
- Unlike beta-blockers, amlodipine does not mask hypoglycemia symptoms and is safe in diabetics.
Sources: Lippincott Illustrated Reviews: Pharmacology | Goodman & Gilman's The Pharmacological Basis of Therapeutics | Morgan and Mikhail's Clinical Anesthesiology, 7th Ed. | Brenner & Rector's The Kidney, 2nd Vol. | Harrison's Principles of Internal Medicine, 22nd Ed.
This is a shared conversation. Sign in to Orris to start your own chat.