Rheumatic fever
Reading File
Finding Sources
Searching PubMed
"rheumatic fever" AND diagnosis
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks with visual material. Here is a full, detailed overview of Rheumatic Fever.
Acute Rheumatic Fever (ARF)
Definition and Overview
Acute rheumatic fever is an acute, immunologically mediated, multisystem inflammatory disease triggered by pharyngitis caused by Group A beta-hemolytic Streptococcus (GAS, Streptococcus pyogenes). It is not a direct infection of the heart or joints - rather, it is a post-infectious immune-mediated sequela. The most feared complication is rheumatic heart disease (RHD), which remains the most important form of acquired heart disease in children and young adults in low- and middle-income countries.
- Goldman-Cecil Medicine (p. 269)
- Robbins & Kumar Basic Pathology (p. 366)
Epidemiology
- Peak age: 5-15 years; rare before age 3, uncommon after 15
- More intense inflammation in younger children; adults more commonly show arthritis
- Worldwide incidence: up to 20 per 100,000; in developed nations, <2 per 100,000
- Significantly higher among indigenous populations (Australia, New Zealand: children 5-14 years)
- ARF developed in ~1.6-2.5% of untreated GAS pharyngitis cases in outbreak settings
- Rheumatic heart disease peaks in the 3rd and 4th decades; more common in women
Pathogenesis
The mechanism involves molecular mimicry:
- Streptococcal M protein and other antigens share structural similarities with human proteins (myosin, laminin, vimentin, tropomyosin)
- Cross-reactive antibodies and T cells attack host cardiac tissue, joints, and basal ganglia
- Carditis: antibody binding + T-cell infiltration of the heart
- Arthritis: immune complex deposition in joints
- Chorea: antibody cross-reactivity with basal ganglia neurons
- Skin manifestations: delayed hypersensitivity reactions
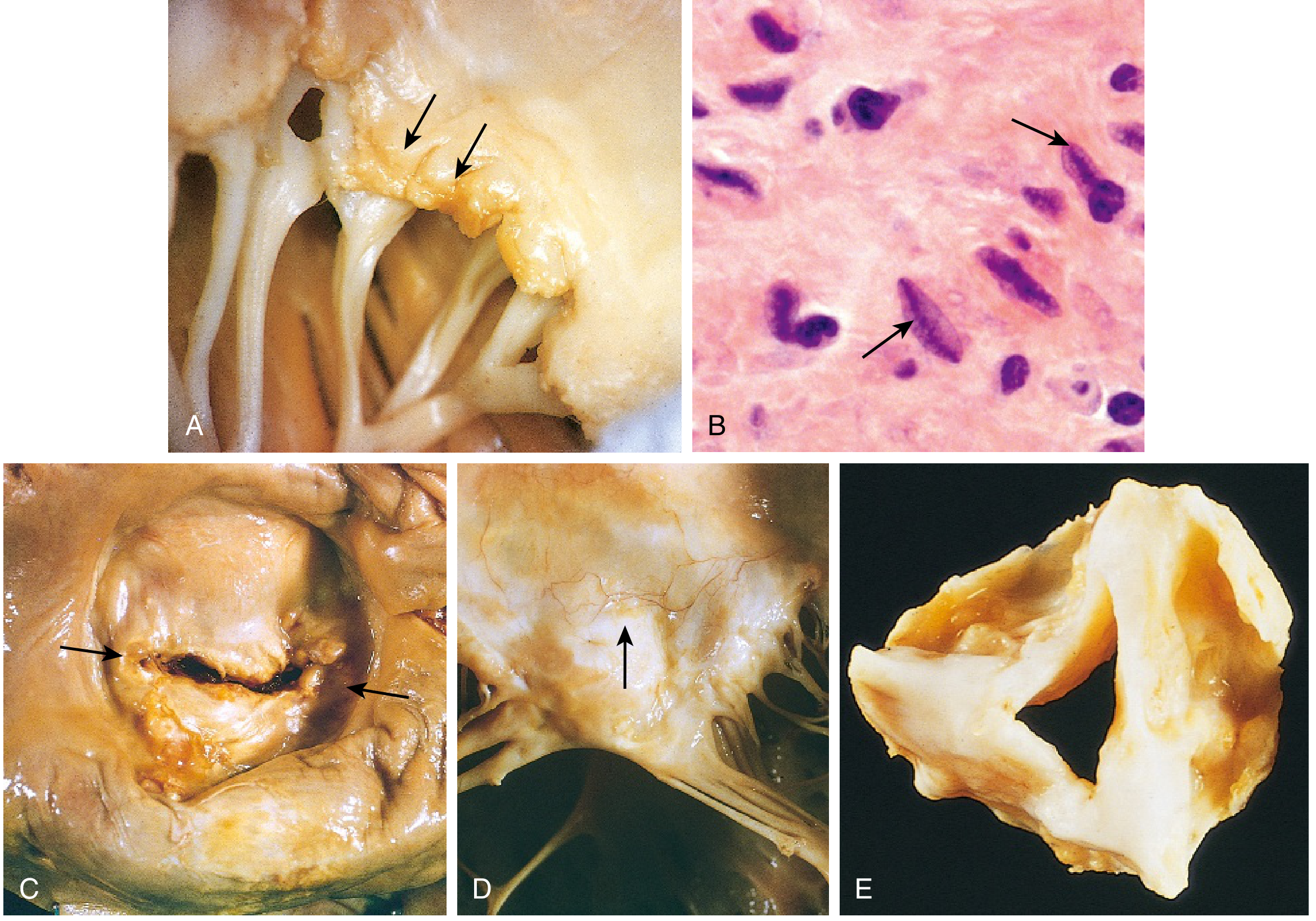
Histopathology: Aschoff Body
The hallmark histopathologic lesion of rheumatic carditis is the Aschoff body (Aschoff nodule) - a granulomatous lesion composed of:
- A central zone of fibrinoid necrosis
- Surrounded by activated macrophages called Anitschkow cells (caterpillar cells) - identified by their distinctive elongated, bar-shaped nucleus with a central chromatin ribbon resembling a caterpillar
- Accompanied by lymphocytes, plasma cells, and occasional giant cells
Aschoff nodules are typically found subendocardially. They are pathognomonic of rheumatic carditis.
Clinical Manifestations
ARF develops approximately 2-3 weeks after streptococcal pharyngitis (mean 18.6 days). Note: chorea has a longer latency of 4-8 weeks. Symptoms typically last 2-4 weeks.
| Manifestation | Frequency | Key Features |
|---|---|---|
| Fever | >90% | Usually >38.5°C |
| Polyarthritis | 75% | Migratory, large joints (knees 76%, ankles 50%, elbows/wrists 12-15%); exquisite tenderness disproportionate to findings; sterile synovial fluid with lymphocyte predominance; responds rapidly to NSAIDs |
| Carditis (pancarditis) | >50% | Affects pericardium, myocardium, and endocardium; most significant: mitral valvulitis (regurgitation initially); aortic valve less commonly |
| Sydenham Chorea | 30% | Involuntary, non-rhythmic, purposeless movements; more pronounced on one side; stops during sleep; also called "St. Vitus dance" |
| Erythema marginatum | <10% | Pink, non-pruritic, blanching macules/papules spreading in a serpiginous pattern on trunk and proximal limbs |
| Subcutaneous nodules | <10% | 0.5-2 cm, painless, over bony prominences or extensor tendons |
Other findings:
- Elevated inflammatory markers (ESR, CRP)
- ECG: prolonged PR interval
- Normochromic normocytic anemia, leukocytosis
- Tachycardia out of proportion to fever
Diagnosis: Revised Jones Criteria (2015 AHA)
There is no single definitive test. Diagnosis requires fulfillment of the Jones Criteria plus evidence of antecedent GAS infection (positive throat culture, rapid strep test, or elevated streptococcal antibody titers - ASO or anti-DNase B).
The 2015 revision introduced population-based risk stratification:
- Low-risk population: ARF incidence <2/100,000 school-aged children/year or RHD prevalence ≤1/1,000/year
- Moderate/High-risk population: higher incidence regions (requires lower threshold to avoid false negatives)
Major Criteria
| Low-Risk Populations | Moderate/High-Risk Populations |
|---|---|
| Carditis (clinical and/or subclinical echocardiographic valvulitis) | Carditis (clinical and/or subclinical echocardiographic valvulitis) |
| Polyarticular arthritis | Mono- or polyarticular arthritis |
| Chorea | Chorea |
| Erythema marginatum | Erythema marginatum |
| Subcutaneous nodules | Subcutaneous nodules |
Minor Criteria
| Low-Risk | Moderate/High-Risk |
|---|---|
| Polyarthralgia | Monoarthralgia |
| Fever ≥38.5°C | Fever ≥38.5°C |
| ESR ≥60 mm AND/OR CRP ≥3.0 mg/dL | ESR ≥30 mm AND/OR CRP ≥3.0 mg/dL |
| Prolonged PR interval (if carditis not already a major criterion) | Prolonged PR interval (same caveat) |
Diagnostic Rule
- Initial ARF: 2 major criteria, OR 1 major + 2 minor criteria
- Recurrent ARF: 2 major, OR 1 major + 2 minor, OR 3 minor criteria
Note: Subclinical (echocardiographic) carditis is now included as a major criterion - echocardiography with Doppler is recommended in all suspected cases to detect valvulitis not apparent clinically.
- Goldman-Cecil Medicine, Table 269-3 (adapted from AHA 2015 Scientific Statement)
Treatment
1. Eradication of GAS (Primary Treatment)
| Agent | Regimen |
|---|---|
| IM Benzathine Penicillin G (preferred) | 1.2 million units single dose (600,000 units if <27 kg) |
| Oral Penicillin V | 500 mg 3x/day for 10 days |
| Amoxicillin | 500 mg twice daily for 10 days |
| Clarithromycin (penicillin allergy) | 250 mg twice daily for 10 days |
2. Anti-inflammatory Therapy
Arthritis and fever:
- Aspirin (traditional first-line): 50-100 mg/kg/day in 4-5 divided doses (max 4-8 g/day in adults); monitor for salicylate toxicity (tinnitus, nausea, vomiting)
- Naproxen (increasingly preferred): 10-20 mg/kg/day in 2 divided doses; fewer GI side effects, twice-daily dosing; validated in small studies
- Continue for 2-4 weeks, reducing dose as symptoms resolve
NSAIDs do NOT alter cardiac outcomes.
Carditis (severe, with heart failure):
- Glucocorticoids: Prednisone 1-2 mg/kg/day (max 80 mg), up to 3 weeks. Meta-analyses have not definitively proven benefit over placebo/salicylates, but many clinicians use them in severe carditis based on evidence of improved echocardiographic parameters.
Chorea:
- Mild: calm environment, reassurance
- Severe: Carbamazepine or sodium valproate preferred over haloperidol; response in 1-2 weeks
- Corticosteroids (prednisone 0.5 mg/kg/day) may accelerate resolution in severe/refractory cases
Bed rest: No longer required long-term; prescribe as needed during active arthritis or heart failure.
- Harrison's Principles of Internal Medicine 22E (p. 2901)
- Rosen's Emergency Medicine (p. 2572-2575)
Secondary Prophylaxis (Prevention of Recurrence)
Every recurrence of ARF can cause additional cumulative cardiac damage. Long-term penicillin prophylaxis is mandatory.
Drug of choice: IM Benzathine Penicillin G 1.2 million units every 4 weeks (every 3 weeks in very high-risk patients)
- Oral Penicillin V 250 mg twice daily (less reliable adherence)
- Azithromycin 250 mg daily (macrolide alternative in penicillin allergy)
Duration (AHA Recommendations)
| Category | Duration |
|---|---|
| ARF without carditis | 5 years after last attack, or until age 21 (whichever is longer) |
| ARF with carditis, no residual valvular disease | 10 years after last attack, or until age 21 (whichever is longer) |
| ARF with persistent valvular disease | 10 years after last attack, or until age 40 (whichever is longer); sometimes lifelong |
A 2024 Cochrane systematic review (PMID 39312290) confirmed that long-term antibiotic prophylaxis prevents recurrence and progression to RHD, supporting current guidelines. A 2024 meta-analysis (PMID 39542478) highlighted that adherence to secondary prophylaxis remains a major clinical challenge, particularly in endemic regions.
- Harrison's Principles of Internal Medicine 22E, Table 371-4
Cardiac Sequelae: Rheumatic Heart Disease
Repeated episodes of ARF cause progressive scarring:
- Mitral stenosis: the essentially only acquired cause; fibrotic thickening, commissural fusion, chordal thickening/shortening
- Mitral regurgitation (early), mitral stenosis (late)
- Aortic valve next most commonly affected
- Tricuspid and pulmonary valves less commonly involved
- Chronic RHD is the most common cause of acquired heart disease in children/young adults in low-income countries
Key Distinguishing Points (High-Yield Summary)
| Feature | Detail |
|---|---|
| Organism | Group A beta-hemolytic Strep (S. pyogenes) - pharyngitis only (skin infections do not cause ARF) |
| Latency | 2-3 weeks (chorea: 4-8 weeks) |
| Pathognomonic lesion | Aschoff body (Anitschkow cells) |
| Most common manifestation | Arthritis (75%) |
| Most serious manifestation | Carditis - valvulitis (mitral > aortic) |
| Only acquired cause of mitral stenosis | Rheumatic fever |
| Diagnostic framework | Revised Jones Criteria (2015 AHA) |
| Prophylaxis drug of choice | IM Benzathine Penicillin G q4 weeks |
| Treatment for arthritis | Aspirin or naproxen (NSAIDs) |
| Chorea treatment | Carbamazepine or valproate |
This is a shared conversation. Sign in to Orris to start your own chat.