Breast Anatomy Complete information
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
I now have all the information needed for a comprehensive, well-illustrated answer. Here is the complete breast anatomy reference:
Breast Anatomy - Complete Reference
1. Position and Surface Boundaries
The breast (mammary gland) lies between the skin and the superficial pectoral fascia on the anterior thoracic wall. In the adult female, its boundaries are:
- Superior: 2nd rib
- Inferior: 6th rib
- Medial: Lateral sternal edge
- Lateral: Midaxillary line
Posteriorly, the breast overlies the pectoralis major (upper and medial portions), the serratus anterior (inferolateral), the external abdominal oblique, and the upper rectus sheath. A tongue-like projection of glandular tissue extends superlaterally around the lower margin of the pectoralis major into the axilla - this is the axillary tail (of Spence).
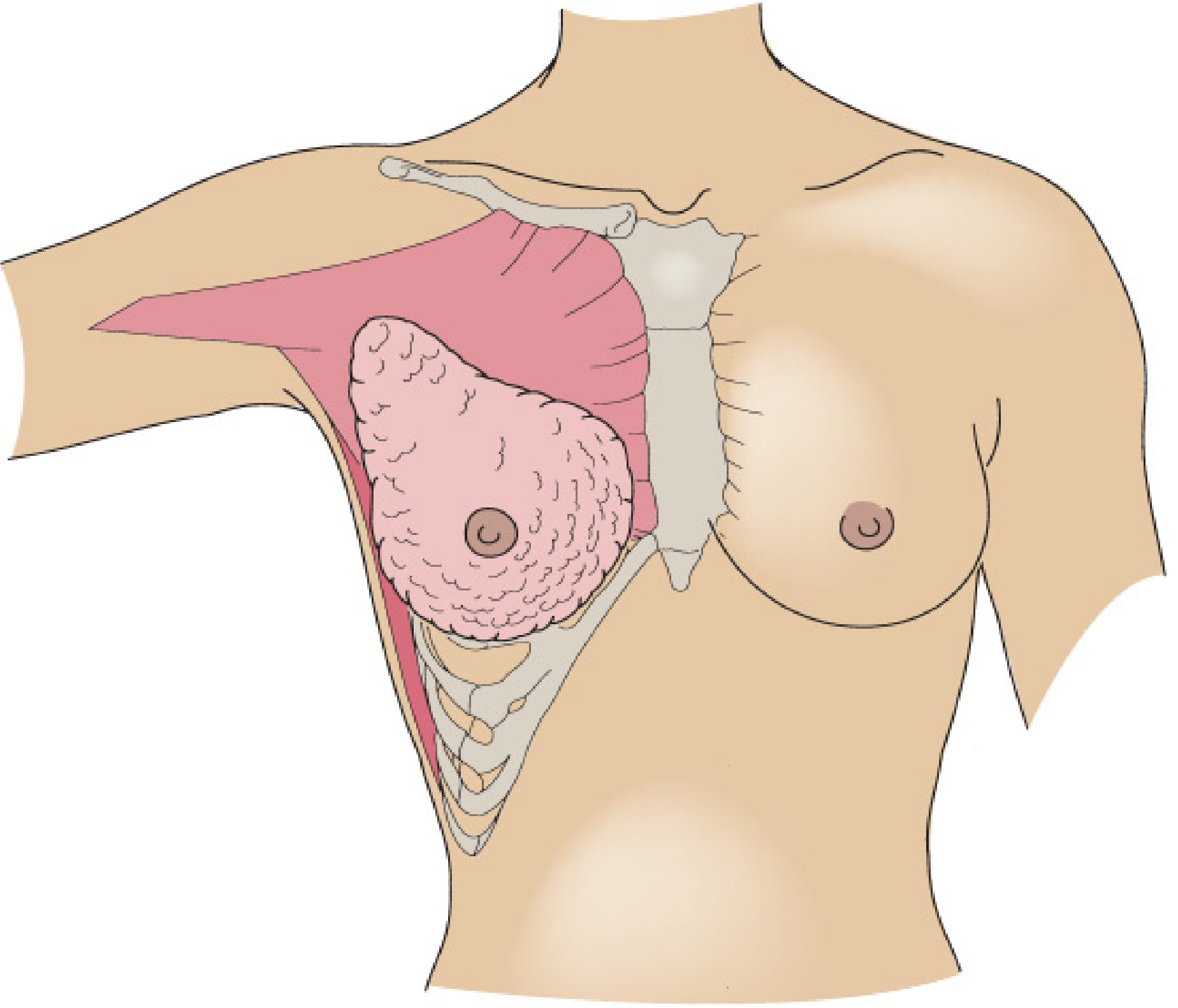
Figure: The adult female breast. The upper and medial portions rest on the pectoralis major muscle; the inferolateral portion rests on serratus anterior. (Fischer's Mastery of Surgery)
2. Gross Internal Structure
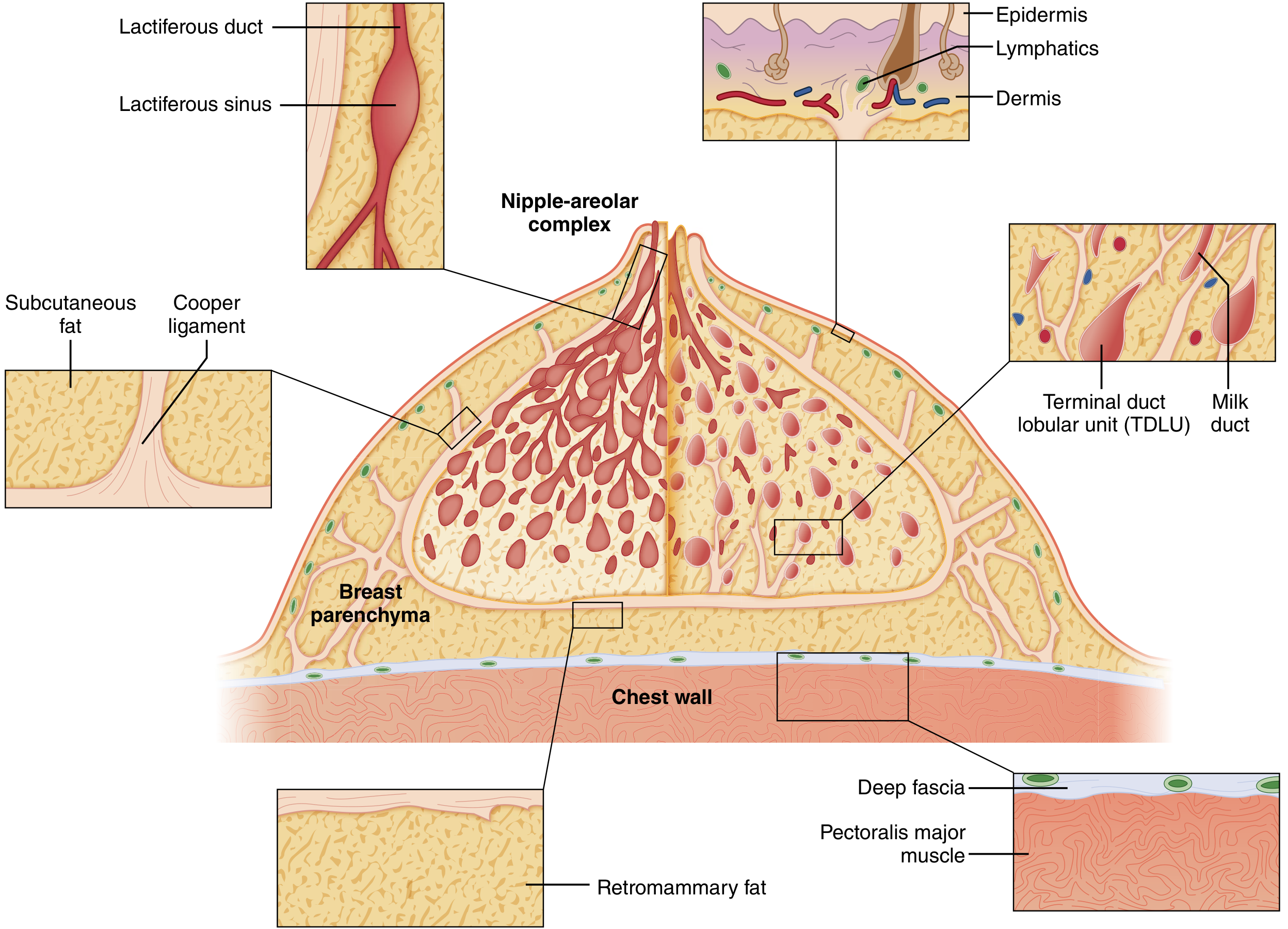
Figure: Cutaway diagram of the mature resting breast showing lactiferous ducts, lactiferous sinus, Cooper ligaments, TDLU, deep fascia, and pectoralis major. (Sabiston Textbook of Surgery)
The breast is composed of three principal tissue types:
- Glandular epithelium - the functional secretory component
- Fibrous stroma - connective tissue scaffolding
- Adipose tissue - fills the inter-lobar spaces; determines breast size
In adolescents, epithelium and stroma predominate. After menopause, glandular structures involute and are largely replaced by adipose tissue, reducing mammographic density.
Lobes and Ducts
- The breast contains 15-20 lobes of glandular tissue, arranged radially around the nipple-areolar complex (NAC).
- Each lobe is made up of 20-40 lobules, each lobule containing 10-100 alveoli (acini).
- Each lobe ends in a lactiferous duct, which dilates into a lactiferous sinus just beneath the areola, then narrows again to open through a constricted orifice at the nipple.
- There is no cross-communication between the independent duct systems.
Terminal Duct Lobular Unit (TDLU)
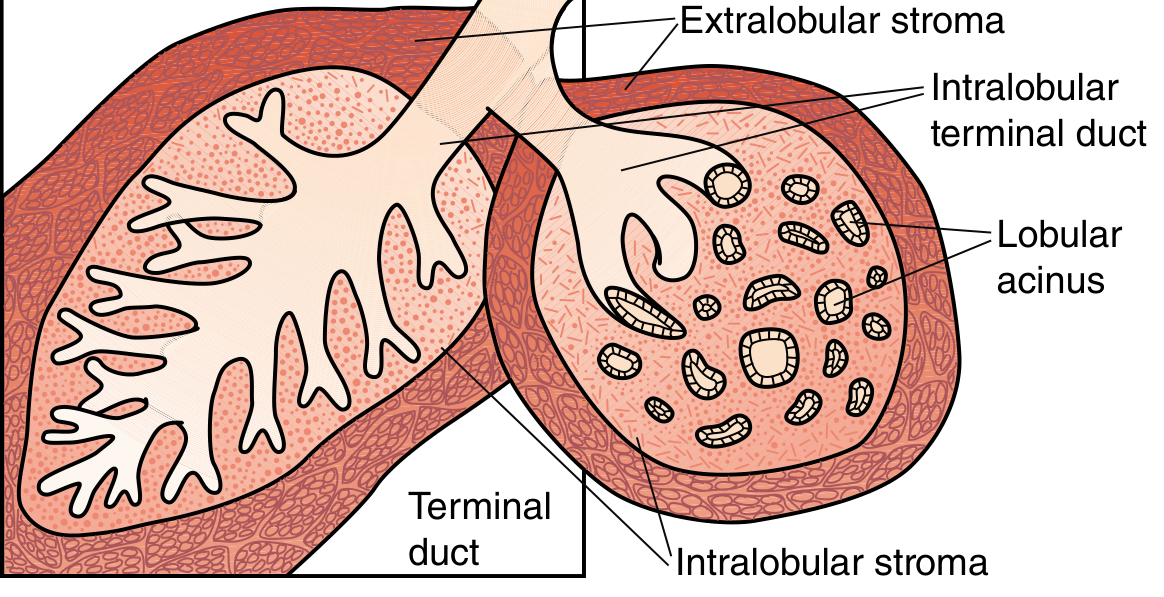
Figure: Mature resting terminal duct lobular unit (TDLU). (Sabiston Textbook of Surgery)
The TDLU is the fundamental secretory and pathological unit of the breast:
- Consists of a terminal duct + its associated lobule (cluster of acini)
- Intralobular stroma is a loose, specialized connective tissue containing capillaries and lymphocytes
- Distinct from the denser interlobular stroma containing larger ducts, blood vessels, and fat
- The entire ductal system is lined by epithelial cells surrounded by myoepithelial cells (contractile - propel milk toward nipple)
- A continuous basement membrane (laminin, type IV collagen, proteoglycans) surrounds the ducts - breaching this membrane = invasion = metastatic potential
- The TDLU is the origin of the majority of breast malignancies
Weight
- Average non-lactating breast: 150-225 g
- Lactating breast: may exceed 500 g
- The left breast is commonly slightly larger than the right
3. Suspensory Ligaments of Cooper
Fibrous connective bands (Cooper's ligaments) run between the deep fascia and the dermis, providing both support and mobility to the breast. They:
- Fuse with the overlying superficial fascia just under the dermis
- Coalesce as interlobular fascia within the parenchyma
- Connect to the deep fascia over the pectoralis muscle
- Are anchored into the skin - infiltration by cancer or breast edema causes them to contract, producing skin dimpling and the "peau d'orange" (orange-skin) appearance
4. Nipple-Areolar Complex (NAC)
- Skin is highly pigmented, composed of stratified squamous epithelium
- Beneath the NAC are bundles of smooth muscle fibers arranged radially, circumferentially, and longitudinally - allow nipple erection from stimuli
- Montgomery glands (accessory sebaceous/mammary glands) are present along the areolar margin, with their openings - the Tubercles of Morgagni - visible as nodular elevations on the areolar surface
- Rich sensory innervation: the nipple contains numerous free nerve endings and Meissner corpuscles; the areola contains Ruffini-like endings and Krause end-bulbs
5. Blood Supply
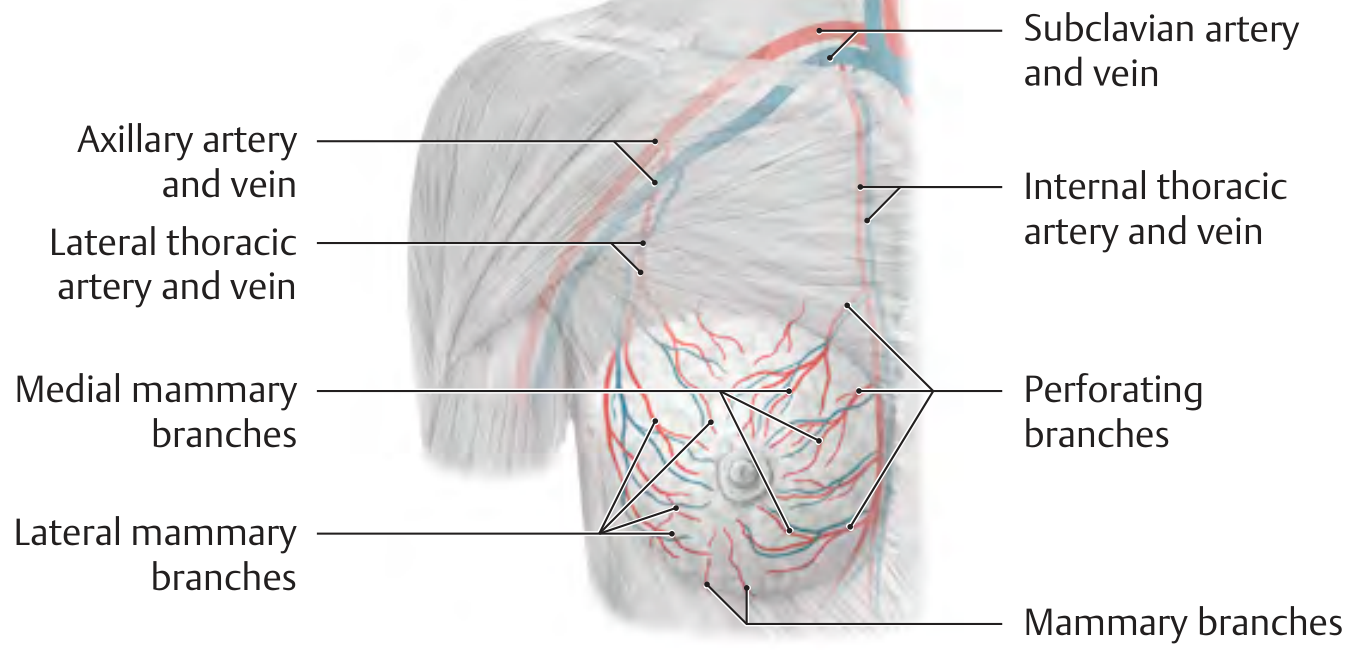
Figure: Vasculature of the breast - medial mammary branches, perforating branches, lateral thoracic branches. (THIEME Atlas of Anatomy)
Arterial Supply (three main sources)
| Artery | Branch | Supply |
|---|---|---|
| Internal thoracic (mammary) artery | Perforating branches (2nd-4th intercostal spaces) - medial mammary branches | Medial and central breast (~60%) |
| Lateral thoracic artery | Lateral mammary branches | Lateral breast |
| Axillary artery branches | Superior thoracic a., lateral thoracic a., pectoral branches of thoracoacromial a. | Upper and lateral breast |
| Posterior intercostal arteries | Lateral branches (2nd-5th spaces) - mammary branches | Posterior and lateral breast |
Venous Drainage
Parallels the arterial supply:
- Internal thoracic veins (drain medially)
- Lateral thoracic veins (drain laterally into axillary vein)
- Intercostal veins (drain posteriorly into azygos/hemiazygos)
The venous connection to the azygos and intercostal veins is a route for haematogenous metastasis - particularly to the vertebral column and lungs.
6. Lymphatic Drainage
Lymphatic channels are abundant in breast parenchyma and dermis. Specialized subareolar lymphatics form the Sappey's plexus under the nipple and areola.
Direction of flow: skin → subareolar (Sappey's) plexus → interlobular parenchymal lymphatics
| Drainage Route | Proportion |
|---|---|
| Axillary lymph nodes | 70-80% (primary) |
| Internal mammary nodes | Predominant in ~2-3%; secondary route in ~20% |
| Supraclavicular nodes | Via Level III nodes |
Axillary Lymph Node Levels
Defined by relationship to the pectoralis minor muscle:
- Level I - lateral to the lateral border of pectoralis minor (low axilla)
- Level II - posterior to pectoralis minor + interpectoral (Rotter's) nodes between pectoralis major and minor
- Level III - medial to pectoralis minor; includes infraclavicular nodes
The apex of the axilla is the costoclavicular (Halsted) ligament, where the axillary vein becomes the subclavian vein. Drainage continues to supraclavicular nodes (outside the axilla proper).
7. Nerve Supply (Sensory Innervation)
The sensory innervation has a segmental arrangement:
- Lateral and anterior cutaneous branches of intercostal nerves T2-T6 - primary supply to the breast
- Medial branches of supraclavicular nerves (from cervical plexus C3-C4) - supply upper breast skin
- The 4th intercostal nerve (lateral cutaneous branch, T4) provides the dominant innervation to the nipple-areolar complex
8. Important Surgical Nerves in the Axilla
| Nerve | Origin | Muscle Innervated | Injury Consequence |
|---|---|---|---|
| Long thoracic nerve (nerve of Bell) | C5, C6, C7 | Serratus anterior | Winged scapula |
| Thoracodorsal nerve | Posterior cord of brachial plexus | Latissimus dorsi | Weakness in shoulder extension/adduction |
| Medial pectoral nerve | Medial cord of brachial plexus | Pectoralis major | Weakness in adduction/medial rotation |
| Intercostobrachial nerves | Lateral cutaneous branches T1-T3 | Sensation (medial upper arm + chest wall) | Numbness/chronic pain syndrome |
9. Fascial Relationships
- The breast lies within the superficial fascia of the anterior thoracic wall
- The retromammary space (between deep surface of breast and pectoralis fascia) contains loose areolar tissue and lymphatics - allows the breast to move freely over the chest wall
- The clavipectoral fascia encloses the pectoralis minor and extends laterally to fuse with the axillary fascia
10. Breast Development and Age-Related Changes
| Phase | Changes |
|---|---|
| Adolescence | Epithelium and stroma predominate; ductal growth under estrogen |
| Reproductive years | TDLU development; cyclic changes (breast volume increases by ~15-45 mL during the luteal phase) |
| Pregnancy (wk 5-6) | Ductal sprouting under estrogen; new terminal buds develop |
| Mid-pregnancy | Ducts canalize; alveoli differentiate under prolactin and progesterone |
| Lactation | Columnar glandular cells secrete milk (apocrine secretion); myoepithelial cells contract under oxytocin; prolactin maintained by nipple stimulation |
| Post-menopausal (involution begins 35-45 yrs) | Glandular tissue replaced by adipose; Cooper ligaments lose tension; mammographic density decreases |
11. Quadrant Distribution
The breast is divided into four quadrants for clinical reference:
- Upper outer quadrant (UOQ)
- Upper inner quadrant (UIQ)
- Lower outer quadrant (LOQ)
- Lower inner quadrant (LIQ)
- Retroareolar region (central)
The upper outer quadrant contains the greatest volume of breast parenchyma and is the most frequent site of both benign and malignant breast disease.
12. Breast Density and Clinical Significance
The ACR BI-RADS system defines four density patterns (1 = almost entirely fatty → 4 = extremely dense):
- Younger women: denser background (more glandular)
- Older women: less dense (replaced by fat)
- Women with the densest background have 4-6 times the risk of breast cancer vs. almost entirely fatty breasts
- Dense tissue also obscures lesions on mammography
Key Sources:
- Sabiston Textbook of Surgery, Ch. 68 - Breast Anatomy, Development, and Physiology
- Fischer's Mastery of Surgery (8th ed.), Ch. 74 - Anatomy of the Breast
- Mulholland and Greenfield's Surgery (7th ed.), Ch. 74 - Surgical Anatomy of the Breast
- THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System, Ch. C/D - Gross, Microscopic Anatomy, Blood and Nerve Supply
- Color Atlas of Human Anatomy Vol. 2 - Internal Organs - Microscopic Structure and Function of the Female Breast
- Grainger & Allison's Diagnostic Radiology - Normal Breast Anatomy (Radiological perspective)
- Gray's Anatomy for Students - Surface Anatomy of the Breast
This is a shared conversation. Sign in to Orris to start your own chat.