pneumonia
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"pneumonia"[MeSH Terms] AND "community-acquired"[MeSH Terms]
Searching the Web
pneumonia overview types causes diagnosis treatment 2025
Reading File
Reading File
Reading File
Searching PubMed
"community-acquired pneumonia" AND management
Reading File
Reading File
Finding Sources
Searching Images
pneumonia chest X-ray consolidation
I have extensive content from the textbooks and images. Now let me compile a comprehensive answer.
Pneumonia
Pneumonia is an infection of the lung parenchyma causing inflammation and consolidation of the normally air-filled alveoli. It affects all age groups and causes more than 1 million hospitalizations per year in the United States, with an in-hospital mortality of ~3.3%.
Classification
| Type | Setting | Common Pathogens |
|---|---|---|
| Community-acquired (CAP) | Acquired outside hospital | S. pneumoniae, Mycoplasma, H. influenzae, respiratory viruses |
| Hospital-acquired (HAP) | ≥48 h after admission | Gram-negatives (Pseudomonas, Klebsiella), MRSA |
| Ventilator-associated (VAP) | Intubated patients | Same as HAP, often MDR organisms |
| Aspiration pneumonia | Aspiration of oropharyngeal/gastric contents | Anaerobes (Peptostreptococcus, Bacteroides), gram-negatives |
| Opportunistic | Immunocompromised host | P. jirovecii (PCP), Cryptococcus, Aspergillus, atypical mycobacteria |
Etiology
Bacteria:
- Streptococcus pneumoniae — most common bacterial cause across all ages beyond neonates
- Haemophilus influenzae — especially in COPD, smokers
- Mycoplasma pneumoniae, Chlamydophila pneumoniae, Legionella pneumophila — "atypical" CAP
- Staphylococcus aureus (including MRSA) — post-influenza, HAP
- Gram-negatives (Pseudomonas, Klebsiella) — nosocomial, nursing home, chronic lung disease
Viruses: Influenza A/B, RSV, SARS-CoV-2, parainfluenza, adenovirus, rhinovirus
Fungi: Pneumocystis jirovecii (immunocompromised), Histoplasma, Coccidioides, Aspergillus
Pathophysiology
Organisms reach the lower respiratory tract via microaspiration (most common), inhalation of droplets, or hematogenous spread. Host defenses — mucociliary clearance, alveolar macrophages, secretory IgA — are overwhelmed, triggering an inflammatory response. Neutrophil influx leads to exudate filling alveoli (consolidation), impairing gas exchange and causing hypoxemia.
Clinical Presentation
Classic (bacterial) pattern:
- Abrupt onset of high fever, rigors, pleuritic chest pain
- Productive cough (rust-colored sputum in pneumococcal pneumonia)
- On exam: decreased breath sounds, dullness to percussion, egophony, bronchial breathing over consolidated lobe
- WBC often >15,000/mm³ with neutrophilia
Atypical pattern (Mycoplasma, Chlamydophila, Legionella, viruses):
- Gradual onset, lower-grade fever, dry cough
- Headache, myalgia, extrapulmonary features (GI symptoms with Legionella)
- Less impressive chest findings on exam
In children:
- Tachypnea disproportionate to fever is often the earliest clue
- Intercostal retractions, nasal flaring in infants
- Viral pneumonia: less toxic, low-grade fever, wheeze
- Bacterial pneumonia: high fever, chills, dyspnea, toxic appearance
In neonates: Group B streptococci and gram-negatives (early); Chlamydia trachomatis at 3–19 weeks of age causes afebrile pneumonia with staccato cough
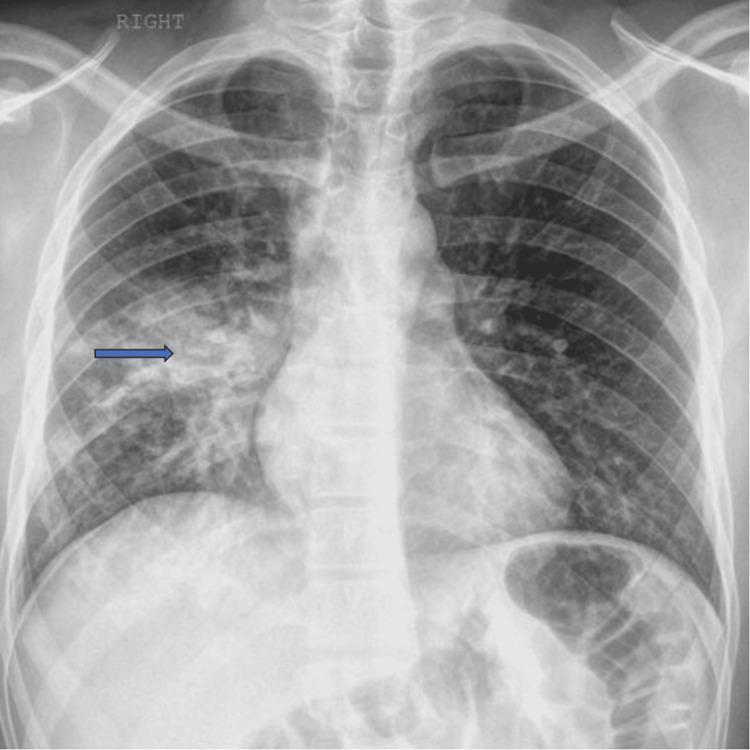
Diagnosis
Chest X-ray is the cornerstone — infiltrates, lobar consolidation, or interstitial pattern. Below are characteristic CXR appearances:

Lab investigations:
- CBC (leukocytosis with neutrophilia in bacterial; lymphocytosis in viral)
- BMP, LFTs (Legionella causes hyponatremia and elevated LFTs)
- Blood cultures (2 sets) — positive in ~10–15% of hospitalized CAP
- Sputum Gram stain + culture (low sensitivity/specificity)
- Urinary antigen tests — highly specific for S. pneumoniae and Legionella
- Procalcitonin — helps distinguish bacterial from viral; guides antibiotic stewardship
Severity scoring (CAP):
- PSI (Pneumonia Severity Index) — classes I–V based on 20 variables; determines outpatient vs. inpatient care
- CURB-65 — simpler: Confusion, Urea >7 mmol/L, RR ≥30, BP <90/60, Age ≥65; score 0–1 = outpatient, 2 = consider admission, ≥3 = ICU consideration
Treatment
Outpatient CAP (low severity, no comorbidities)
- Amoxicillin 1 g TID or doxycycline (if atypical suspected)
- Macrolide monotherapy (azithromycin) where local S. pneumoniae resistance <25%
Outpatient CAP (with comorbidities — COPD, DM, heart disease, recent antibiotics)
- Respiratory fluoroquinolone (levofloxacin, moxifloxacin) OR
- β-lactam + macrolide combination
Hospitalized, non-ICU
- β-lactam (ampicillin-sulbactam, ceftriaxone) + macrolide OR
- Respiratory fluoroquinolone monotherapy
Severe CAP / ICU
- β-lactam + azithromycin or β-lactam + fluoroquinolone
- Add anti-MRSA coverage (vancomycin or linezolid) if risk factors present
- Add anti-Pseudomonas coverage if structural lung disease, prior broad-spectrum antibiotics, or immunocompromise
HAP / VAP
- Broad-spectrum coverage targeting gram-negatives (piperacillin-tazobactam, cefepime, or carbapenem) ± MRSA coverage
Duration
- Typically 5–7 days for mild-moderate CAP
- Guided by clinical response (afebrile ≥48–72 h, improving O₂)
- Procalcitonin-guided de-escalation reduces antibiotic exposure without worse outcomes
⚠️ Note on β-lactams vs. atypical coverage: Despite the prevalence of atypical pathogens in CAP, controlled trials show β-lactam antibiotics are as effective as macrolides or quinolones in most cases. — Textbook of Family Medicine 9e
Complications
| Complication | Details |
|---|---|
| Parapneumonic effusion | Exudative pleural effusion; ~40% of hospitalized patients |
| Empyema | Infected pleural fluid — requires drainage |
| Lung abscess | Cavitation; common with aspiration, anaerobes, S. aureus |
| Bacteremia / sepsis | Drives mortality, especially in elderly |
| ARDS | Severe bilateral pneumonia → inflammatory lung injury |
| Respiratory failure | Requires mechanical ventilation |
Prevention
- Pneumococcal vaccines:
- PCV15 or PCV20 for adults ≥65 and high-risk groups
- PCV13/15/20 primary series in infants (2, 4, 6 months + booster at 12–15 months)
- PPSV23 revaccination after 10 years if first dose given before age 65
- Influenza vaccine: Annually for everyone ≥6 months; especially important in patients >50, chronic lung disease, diabetes, immune dysfunction
- Hib vaccine: Has markedly reduced pediatric H. influenzae pneumonia since 1985
Key Recent Evidence
- A 2025 network meta-analysis (PMID 40404065) compared antibiotic regimens for hospitalized adults with CAP, informing optimal β-lactam vs. combination therapy choices.
- A 2025 systematic review (PMID 40107661) identified risk factors for drug-resistant pathogens in CAP, supporting targeted empiric coverage decisions.
- A 2024 consensus statement (PMID 39427174) (Italian pediatric intersociety) guided antibiotic therapy for mild-moderate CAP in previously healthy children.
Sources: Textbook of Family Medicine 9e, Rosen's Emergency Medicine 9e, Murray & Nadel's Textbook of Respiratory Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.