15 yrs old female came with lower abdominal pain from 1 week on and off persistent after eating no other symptoms and stable vitals
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Here is a structured clinical approach to this case:
Clinical Assessment: 15-year-old Female, Lower Abdominal Pain, 1 Week, Postprandial, On-and-Off
Key Features to Note
- Adolescent female - gynecologic causes are prominent in the differential
- Postprandial component - points toward a GI-visceral mechanism
- Subacute course (1 week, on and off) - not a surgical emergency but warrants systematic evaluation
- Stable vitals, no other symptoms - reassuring, argues against sepsis, hemorrhage, or peritonitis
Differential Diagnosis (Structured by System)
Gynecologic (Most Important Age Group to Consider)
| Condition | Features | Why it fits/Why not |
|---|---|---|
| Primary dysmenorrhea | Cyclic pain with menses, crampy, suprapubic | Most common in 1-2 years post-menarche; ask about timing with period |
| Ovarian cyst / follicular cyst | Intermittent, unilateral or bilateral, can worsen with bowel filling | Functional cysts increase after menarche |
| Ovarian torsion (intermittent) | Acute unilateral, severe - but intermittent torsion exists | Stable vitals make full torsion unlikely; intermittent form possible |
| Endometriosis | Cyclic or acyclic pain, dysmenorrhea, progressive | Can begin in teens; underdiagnosed |
| PID | Bilateral pain, cervical motion tenderness, discharge, fever | Less likely without fever/discharge; still rule out if sexually active |
| Mittelschmerz | Mid-cycle, unilateral brief pain at ovulation | Typically brief, not 1 week persistent |
Berek & Novak's Gynecology notes: "An adnexal mass can cause severe, acute, or intermittent symptoms caused by torsion, intraperitoneal rupture, or bleeding into the ovarian tissue... The pressure of an enlarging ovarian mass can cause bowel-related symptoms such as constipation, vague discomfort, and early satiety."
Gastrointestinal
| Condition | Features |
|---|---|
| Irritable Bowel Syndrome (IBS) | Postprandial pain, altered bowel habit, common in teen females; "hallmark feature is chronic or recurrent pain associated with altered stool" |
| Constipation / functional bowel disorder | Very common in adolescent girls; postprandial cramping |
| Mesenteric adenitis | Usually after a viral illness; enlarged mesenteric lymph nodes; mimic appendicitis |
| Appendicitis (early/subacute) | Right iliac fossa predominance; anorexia, low fever - must not miss |
| Inflammatory bowel disease | Crohn's can be insidious in teens; associated with systemic features eventually |
Urologic
| Condition | Features |
|---|---|
| UTI / cystitis | Suprapubic pain; usually dysuria, frequency |
| Urolithiasis | Colicky, may radiate to groin |
Approach to the Patient
History (Critical Questions)
- Menstrual history - menarche date, cycle regularity, pain relationship to period (dysmenorrhea?)
- Sexual activity - essential even if denied; ask confidentially (PID, ectopic)
- Pain character - crampy vs. dull, location (central, right, left), radiation
- Postprandial timing - minutes or hours after eating? Bloating, altered bowel habit? (IBS pointer)
- Associated symptoms - vaginal discharge, dyspareunia, urinary symptoms, nausea, fever at home
- Last menstrual period (LMP) - mandatory; consider ectopic even in teenagers
- Family history - endometriosis, IBD
Harrison's Principles of Internal Medicine (22E) emphasizes: "Specific associations with vaginal bleeding, sexual activity, defecation, urination, movement, or eating should be specifically sought. Determination of whether the pain is acute versus chronic and cyclic versus noncyclic will direct further investigation."
Physical Examination
- Abdominal exam: guarding, rebound, tenderness localization (RIF vs. suprapubic vs. adnexal)
- Pelvic exam (if appropriate/indicated): cervical motion tenderness, adnexal masses, discharge
- Rectal exam if appendicitis suspected
Investigations (Stepwise)
First line - mandatory:
- Urine beta-hCG (pregnancy test) - must be done before all else, regardless of stated sexual activity
- Urinalysis and urine culture (UTI)
- Full blood count (infection, inflammation - WBC)
- CRP/ESR (inflammatory process)
- Pelvic/abdominal ultrasound (USG) - primary imaging tool; evaluates ovaries, uterus, appendix, free fluid
If sexually active:
- Vaginal swab/NAAT for Chlamydia trachomatis and Neisseria gonorrhoeae (PID)
- Wet mount preparation
If USG inconclusive or appendicitis strongly suspected:
- CT abdomen/pelvis or MRI (MRI preferred in adolescents to avoid radiation)
If GI cause suspected:
- Stool tests (FOBT, culture if diarrhea present)
- Consider gastroenterology referral if IBS/IBD features
Adnexal Mass Classification in Adolescents
The diagram below (from Berek & Novak's Gynecology) shows the classification framework for adnexal masses in adolescents - relevant if USG shows a pelvic mass:
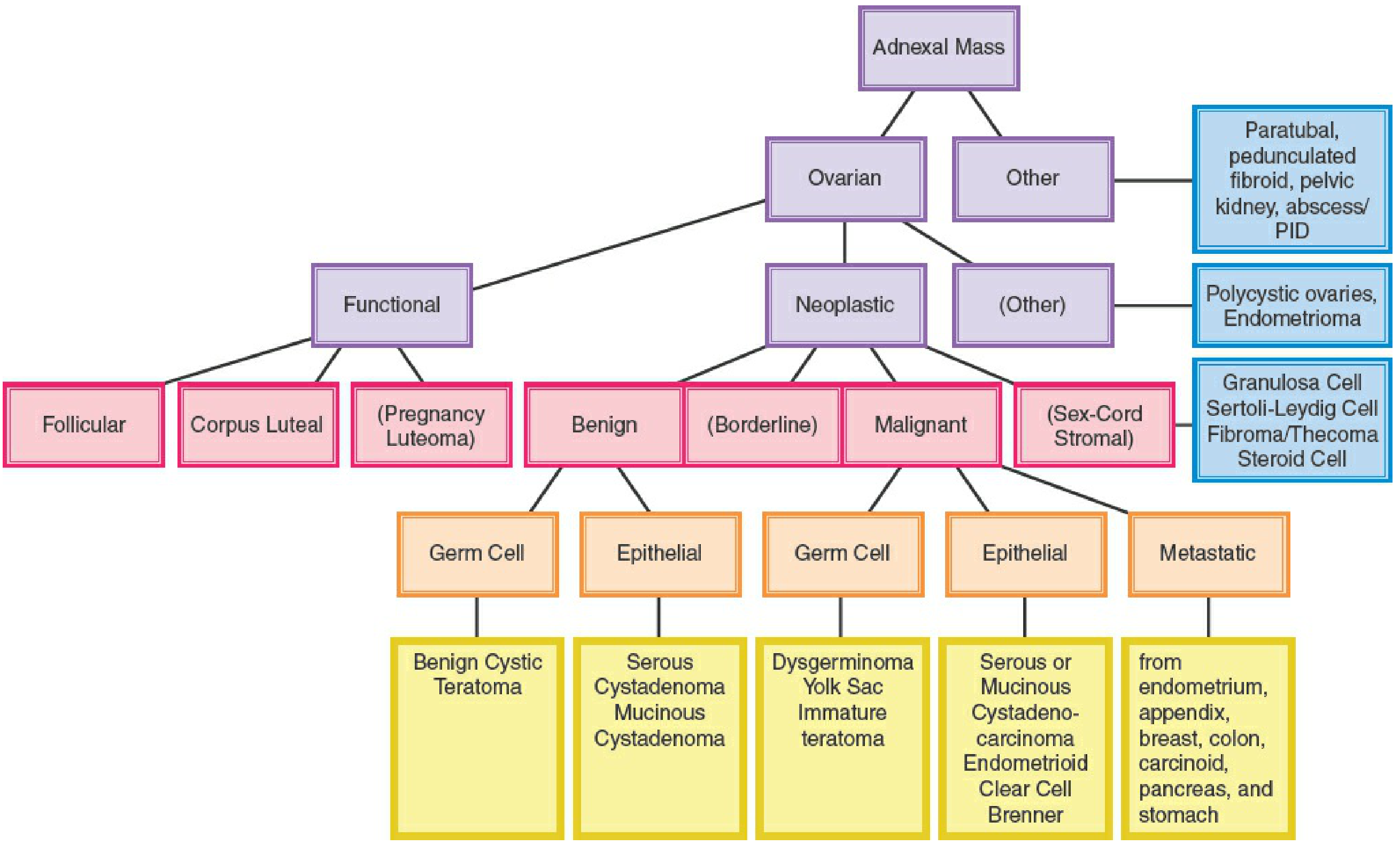
Figure: Algorithm for adnexal masses in adolescents - Berek & Novak's Gynecology
Red Flags Requiring Urgent Action
- Signs of peritonitis (rebound, guarding, rigidity)
- Hemodynamic instability
- Positive beta-hCG with pain (ectopic pregnancy - emergency)
- Absent Doppler flow to ovary on USG (ovarian torsion - surgical emergency)
- Fever with pelvic tenderness (PID with tubo-ovarian abscess)
Most Likely Diagnoses Given This Presentation
Given the mild/stable nature, postprandial component, and subacute course in a teenage female, the top considerations are:
- Functional/GI cause (IBS, constipation) - most common in this demographic, postprandial pattern fits
- Primary dysmenorrhea - if pain is cyclic and peri-menstrual (most common gynecologic cause in teens)
- Functional ovarian cyst - intermittent, common in post-menarchal adolescents
- Mittelschmerz - if mid-cycle and brief; but duration argues against
- Mesenteric adenitis or subacute appendicitis - must exclude
The pregnancy test and pelvic ultrasound are the two most important immediate next steps.
Sources: Harrison's Principles of Internal Medicine 22E (2025); Berek & Novak's Gynecology; Textbook of Family Medicine 9e; Tintinalli's Emergency Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.