FMGE,NEET PG,INICET rank 1 oriented concise notes on Fracture healing.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here are your comprehensive, rank-1 oriented concise notes on Fracture Healing:
FRACTURE HEALING - FMGE / NEET PG / INICET High-Yield Notes
1. TYPES OF FRACTURE HEALING
A. Primary (Direct) Bone Healing
- Occurs with cortical apposition + absolute stability (zero movement at fracture site)
- No callus formation - bone heals directly
- Mechanism: Osteoclastic "cutting cones" cross the fracture line → osteoblasts lay down lamellar bone (Haversian remodeling)
- Seen with: compression plating (ORIF with lag screws/plates)
- Analogy: wound sutured directly together
B. Secondary (Indirect) Bone Healing
- Most common form of fracture healing
- Requires some movement (strain) at fracture site
- Proceeds via callus formation (endochondral + intramembranous ossification)
- Analogy: wound healing via scab formation
2. STAGES OF SECONDARY FRACTURE HEALING
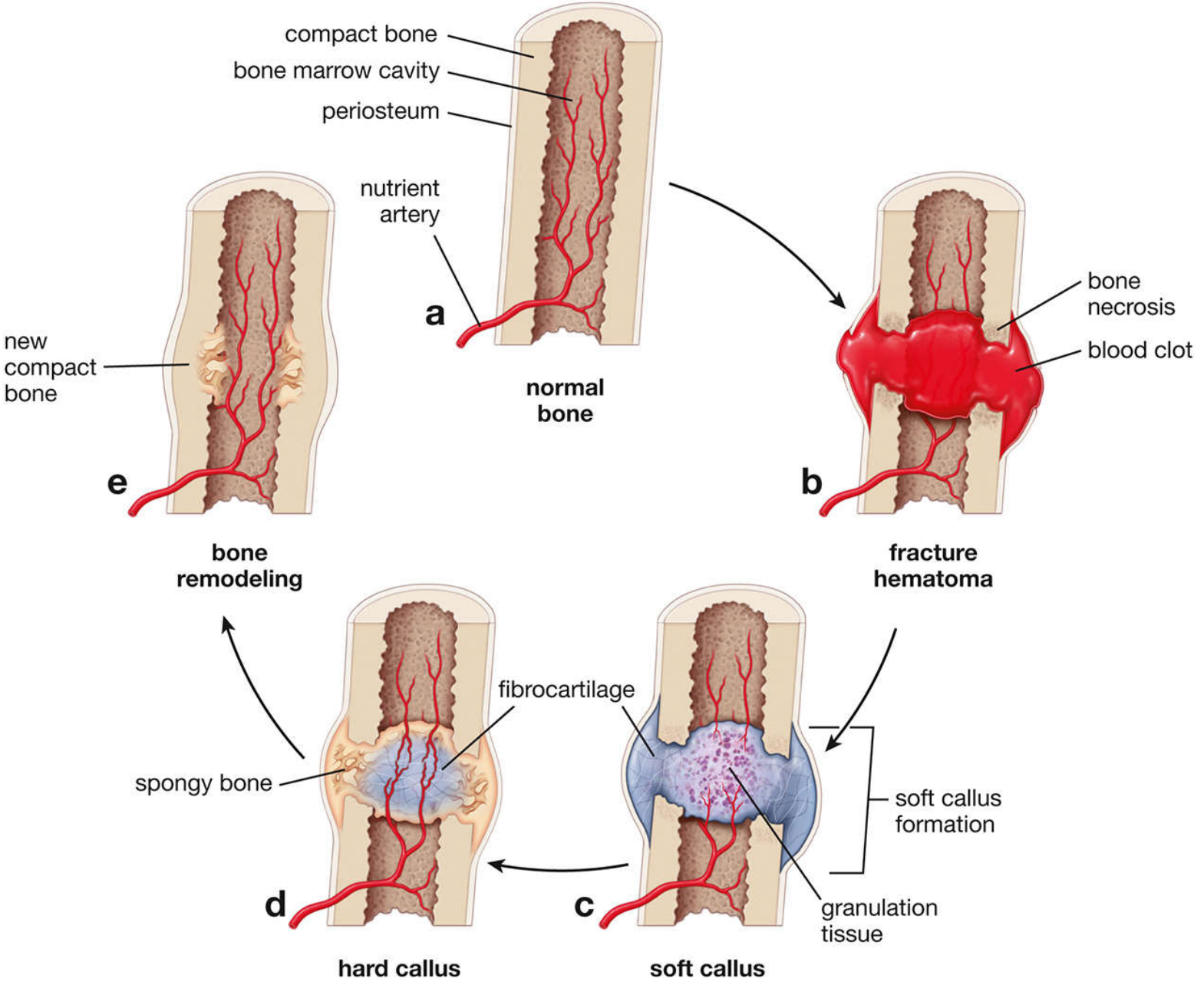
| Stage | Timeline | Key Events |
|---|---|---|
| Stage 1: Hematoma formation | Hours - days | Rupture of blood vessels → hematoma; bone necrosis at fragment ends; platelets release cytokines (TNF-α, IL-1, IL-6); neutrophils then macrophages infiltrate; provides hematopoietic cells capable of secreting growth factors |
| Stage 2: Granulation tissue / Soft callus | Days 4-5 onwards | Pluripotential mesenchymal cells invade → differentiate into fibroblasts, chondroblasts, osteoblasts; angiogenesis occurs; fibrocartilage (soft callus) bridges the gap; stabilizes fracture ends |
| Stage 3: Hard callus (Bony callus) | Weeks 3-12 | Soft cartilaginous callus undergoes endochondral ossification → replaced by woven bone (hard callus); intramembranous ossification occurs on outer periosteal surface simultaneously |
| Stage 4: Remodeling | Months to years | Woven bone → lamellar bone; medullary canal restored; bone returns to near-normal shape per Wolff's law; continues up to 7 years; complete when marrow space is repopulated |
Memory: Hematoma → Granulation → Callus → Remodeling (H-G-C-R)
3. PERREN'S STRAIN THEORY (HIGH YIELD)
- Interfragmentary strain = change in gap length / original gap length
- Strain determines what tissue forms at the fracture site:
| Strain | Tissue Formed |
|---|---|
| >100% | Fibrous tissue (no healing) |
| 10-100% | Fibrous tissue |
| 2-10% | Soft callus (cartilage) |
| <2% | Hard callus → bone |
- Key concept: A narrow gap = HIGH strain (cell rupture); a wide gap = lower strain (cells deform but survive and form tissue)
- As granulation tissue fills the gap, local strain decreases progressively, permitting escalating tissue quality: fibrous → cartilage → bone
- Clinical implication: Some movement = good (stimulates callus); too much = nonunion; zero movement with compression = primary healing
4. FOUR TYPES OF NEW BONE FORMATION IN FRACTURE REPAIR
- Osteochondral ossification (endochondral) - main soft callus pathway
- Intramembranous ossification - periosteal surface, no cartilage template
- Appositional new bone formation
- Osteonal migration (creeping substitution) - primary healing cutting cones
5. HEALING BASED ON FIXATION TYPE
| Fixation Method | Type of Healing |
|---|---|
| Cast / closed treatment | Periosteal bridging callus + endochondral ossification |
| Compression plate (ORIF) | Primary cortical healing (cutting-cone / Haversian remodeling) - NO callus |
| Intramedullary nail | Early: periosteal bridging callus + endochondral; Late: medullary callus + intramembranous |
| External fixator (rigid) | Primary cortical healing + intramembranous |
| External fixator (less rigid) | Periosteal bridging callus + endochondral |
| Inadequate immobilization + good blood supply | Hypertrophic nonunion (type II collagen predominates) |
| Inadequate immobilization + poor blood supply | Atrophic nonunion |
| Inadequate reduction + displacement | Oligotrophic nonunion |
Key rule: Amount of callus is inversely proportional to extent of immobilization
6. BIOCHEMISTRY OF FRACTURE HEALING - COLLAGEN TYPES
| Step | Collagen Types Present |
|---|---|
| Mesenchymal phase | I, II, III, V |
| Chondroid (cartilage) phase | II, IX |
| Chondroid-osteoid (calcifying cartilage) | I, II, X |
| Osteogenic (bone) phase | Type I only |
- In unstable fracture: Type II collagen expressed early, followed by Type I
- Collagen X = marker of hypertrophic chondrocytes (calcifying cartilage)
7. GROWTH FACTORS IN FRACTURE HEALING
| Growth Factor | Action | Notes |
|---|---|---|
| BMP (Bone Morphogenetic Protein) | Osteoinductive - induces mesenchymal cells → osteoblasts | Signals via serine-threonine kinase receptors; intracellular mediators = SMADs |
| TGF-β | Induces MSCs → Type II collagen + proteoglycans; induces osteoblasts → collagen synthesis | Found in fracture hematoma; regulates cartilage and bone in callus |
| IGF-2 | Stimulates Type I collagen, cellular proliferation, cartilage matrix + bone formation | Signals via tyrosine kinase receptors |
| PDGF | Chemotactic for macrophages; stimulates MSC proliferation | |
| FGF | Promotes angiogenesis + MSC proliferation | |
| VEGF | Angiogenesis at fracture site |
BMP subtypes (EXAM FAVOURITE):
- BMP-2 → Used for acute open tibial fractures
- BMP-3 → No osteogenic activity
- BMP-4 → Mutations cause Fibrodysplasia Ossificans Progressiva (FOP)
- BMP-7 (OP-1) → Used for tibial nonunions
- BMPs activate SMADs → osteoblastic differentiation
8. ENDOCRINE / HORMONAL EFFECTS ON FRACTURE HEALING
| Hormone/Factor | Effect | Mechanism |
|---|---|---|
| Cortisone (steroids) | Negative (-) | Decreased callus proliferation |
| Calcitonin | Positive (+?) | Unknown |
| Thyroid hormone / PTH | Positive (+) | Bone remodeling |
| Growth hormone | Positive (+) | Increased callus volume |
| Head injury | Positive (+) | Increases osteogenic response |
9. FACTORS IMPAIRING FRACTURE HEALING
Systemic (Biologic)
- Smoking/Nicotine - increases time to healing; increases nonunion risk (especially tibia); decreases callus strength; increases pseudarthrosis risk after lumbar fusion by up to 500%
- NSAIDs - inhibit COX-2 (required for normal endochondral ossification) → adverse effect on fracture healing and spinal fusions
- Quinolone antibiotics - toxic to chondrocytes, inhibit fracture healing
- Diabetes mellitus - microangiopathy impairs tissue perfusion
- Steroids - decrease callus
- Protein malnutrition - decreased periosteal callus, decreased callus strength, increased fibrous tissue in callus
- Radiation (high-dose) - long-term changes in Haversian system, decreased cellularity
- Age (elderly heal slower)
- Vascular disease / peripheral vascular disease
Local / Mechanical
- Poor blood supply / avascular necrosis
- Infection (esp. open fractures)
- Excessive movement (instability)
- Extensive soft-tissue injury
- Bone loss / large defect
- Inadequate reduction
10. DEFINITIONS - CLINICAL OUTCOMES
| Term | Definition |
|---|---|
| Union | Clinical: fracture withstands physiological loads, minimal pain/tenderness. Radiological: callus bridges fracture site |
| Delayed union | Fracture slow to heal; not healed in expected timeframe (no fixed duration for all fractures) |
| Non-union | No healing + no potential to heal without intervention; OR no radiological/clinical improvement over 3 months; labeled nonunion at 6 months post-injury |
| Malunion | Fracture healed in abnormal position (angulation, rotation, shortening) |
| Consolidation | Follows union; bone returns to normal strength; radiologically: return of normal cortical pattern |
| Remodeling | Bone assumes normal configuration per forces (Wolff's law); occurs in children > adults |
11. TYPES OF NON-UNION
| Type | Cause | Biology/Vascularity |
|---|---|---|
| Hypertrophic | Inadequate immobilization, good blood supply | Good vascularity; abundant callus ("elephant foot" or "horse hoof" pattern on X-ray); type II collagen predominates |
| Atrophic | Poor blood supply (+ poor immobilization) | Avascular; no callus; biological problem |
| Oligotrophic | Inadequate reduction with displacement | Minimal callus |
- Hypertrophic nonunion → treat with stabilization alone
- Atrophic nonunion → needs bone graft + stabilization
12. BONE GRAFTING - PROPERTIES
| Property | Definition |
|---|---|
| Osteogenesis | Graft contains live cells that form new bone (only autograft) |
| Osteoinduction | Stimulates host undifferentiated mesenchymal cells → osteoblasts (BMPs) |
| Osteoconduction | Scaffold/framework for ingrowth of new bone from host |
| Graft Type | Osteogenesis | Osteoinduction | Osteoconduction |
|---|---|---|---|
| Autograft (gold standard) | Yes | Yes | Yes |
| Fresh allograft | No | Yes (BMP preserved) | Yes |
| Fresh-frozen allograft | No | Yes (BMP preserved) | Yes |
| Freeze-dried (lyophilized) allograft | No | No (BMP depleted) | Yes |
| DBM (Demineralized Bone Matrix) | No | Minimal | Yes |
| Synthetic (HA, TCP) | No | No | Yes |
- Cancellous autograft incorporates via creeping substitution (osteoblasts lay new bone on old trabeculae)
- Hydroxyapatite does NOT elicit an immune response
13. ELECTRICAL / PHYSICAL STIMULATION OF FRACTURE HEALING
| Stimulus | Mechanism/Use |
|---|---|
| Low-intensity pulsed ultrasound (LIPUS) | 30 mW/cm² - accelerates fracture healing, increases callus mechanical strength |
| Direct current | Stimulates inflammatory-like response, decreases O₂, increases tissue pH |
| Alternating current | Affects cAMP + collagen synthesis/calcification during repair |
| Pulsed electromagnetic fields (PEMF) | Initiates calcification of fibrocartilage (but NOT fibrous tissue) |
14. QUICK-FIRE HIGH-YIELD POINTS
- Wolff's law - bone remodels along lines of mechanical stress (piezoelectric charges)
- Woven bone → replaced by lamellar bone in remodeling
- Remodeling begins in middle of repair phase, continues up to 7 years
- Complete healing = when marrow space is repopulated
- Radioisotope scan shows increased activity long after clinical and radiological union (remodeling continues)
- Fracture in children heals faster; remodeling potential much greater than adults
- Cancellous bone heals faster than cortical bone (more surface area, more osteoblasts)
- COX-2 inhibitors (NSAIDs) specifically block prostaglandin synthesis required for endochondral ossification - hence impair callus formation
- Compression plating = primary healing = NO callus
- IM nailing = secondary healing = callus present
- Amount of callus inversely proportional to extent of immobilization
Sources: Miller's Review of Orthopaedics 9th Ed. | Bailey & Love's Short Practice of Surgery 28th Ed. | Campbell's Operative Orthopaedics 15th Ed. 2026 | Rockwood & Green's Fractures in Adults 10th Ed. 2025 | Histology: A Text & Atlas (Eroschenko)
This is a shared conversation. Sign in to Orris to start your own chat.