Creatinine level is 1.0 . What is causes of slightly higher level of creatinine but in normal range. Physiological and pathological
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Here is a thorough, textbook-grounded answer:
Creatinine 1.0 mg/dL - Causes of High-Normal Levels
Understanding the Normal Range First
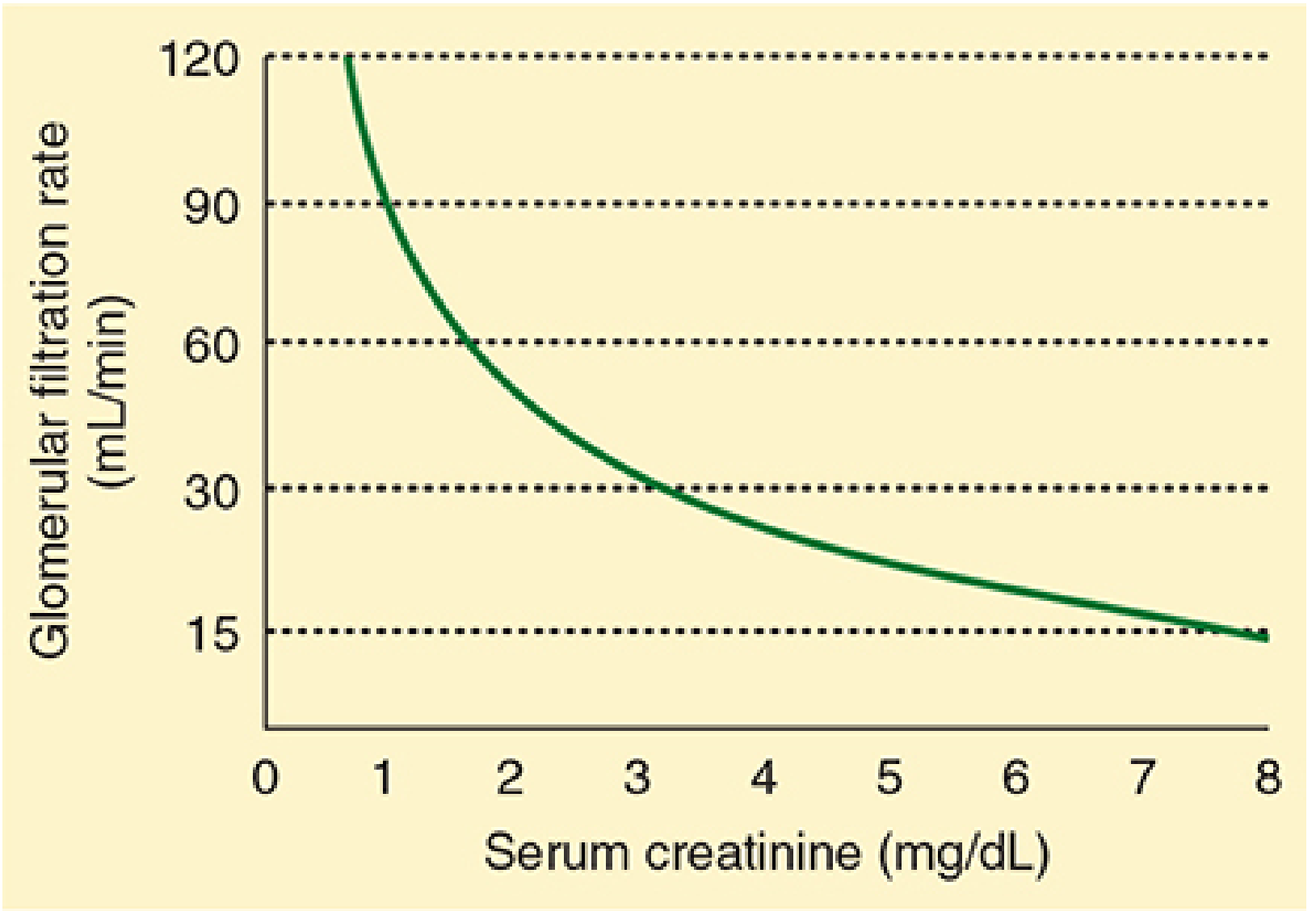
Serum creatinine normal range is approximately 0.8-1.3 mg/dL in men and 0.6-1.0 mg/dL in women (Morgan & Mikhail's Clinical Anesthesiology, 7e). A value of 1.0 mg/dL is upper-normal for a woman but mid-normal for a man. The key point is that creatinine is generated from the breakdown of creatine and phosphocreatine in skeletal muscle, freely filtered by the glomerulus, and to a lesser extent (10-30%) secreted by the proximal tubule.
The graph below illustrates the inverse, non-linear relationship between serum creatinine and GFR - a 1.0 mg/dL value corresponds to a GFR near the upper end of the normal physiological range:
PHYSIOLOGICAL CAUSES of High-Normal Creatinine
These are normal variants - not disease states - that push creatinine to the upper end of the normal range.
1. Higher Muscle Mass / Body Build
The most common physiological reason. Creatinine production averages 20-25 mg/kg/day in men and 15-20 mg/kg/day in women, directly proportional to muscle mass (Brenner & Rector's The Kidney). Athletes, bodybuilders, or physically well-built individuals naturally produce more creatinine. The normal range in Rosen's Emergency Medicine explicitly states it "extends from 0.5 mg/dL in thin people to 1.5 mg/dL in muscular persons."
2. Male Sex
Men have greater muscle mass than women. The reference range upper limit for men is ~1.2-1.3 mg/dL vs ~1.0 mg/dL in women. A value of 1.0 mg/dL in a woman is at the upper limit; the same value in a man is comfortably mid-range.
3. High Protein / Meat-Rich Diet
High protein meals - particularly cooked red meat - transiently increase serum creatinine. This is listed as a direct modifier in Goldman-Cecil Medicine's table of factors that alter creatinine production. Creatine in meat is converted to creatinine during cooking and after absorption.
4. Intense Exercise / Strenuous Physical Activity
Vigorous exercise increases creatinine release from muscle. This is a transient physiological elevation that normalizes after rest. In rhabdomyolysis (the extreme form), serum creatinine rises rapidly from preformed creatinine released by damaged muscle.
5. Mild Dehydration / Reduced Fluid Intake
Intravascular volume depletion leads to reduced renal blood flow and lower GFR, concentrating creatinine in the blood. Even mild dehydration can nudge creatinine toward the upper-normal range without any renal pathology.
6. Young Adult Age (Peak Muscle Mass)
Creatinine production peaks in early adulthood (mean ~23.8 mg/kg in men aged 20-29 years) and progressively falls with aging, reaching ~9.8 mg/kg in men aged 90-99 years (Brenner & Rector's The Kidney). So a 1.0 mg/dL in a young, muscular 25-year-old is much more physiological than in a 70-year-old.
7. Black/African Ethnicity
Higher average muscle mass in individuals of African ancestry is well-documented. As shown in the Table of Family Medicine reference values, African American men have higher creatinine values at every age bracket compared to European American men (Textbook of Family Medicine, 9e).
PATHOLOGICAL CAUSES (Mild / Early - still within "normal range")
A creatinine of 1.0 mg/dL can reflect silent early disease where GFR has already declined somewhat but the creatinine has not yet crossed the laboratory reference threshold. This is the key clinical trap.
1. Early/Subclinical Chronic Kidney Disease (CKD Stage 1-2)
"Slightly elevated (or even normal range) serum creatinine levels may correlate with impaired GFR, depending on factors such as age or race" (Textbook of Family Medicine, 9e). In an elderly woman or a person with low muscle mass, a creatinine of 1.0 mg/dL may correspond to a GFR <60 mL/min - the threshold for CKD. GFR calculation (CKD-EPI or MDRD) is mandatory alongside serum creatinine.
2. Early Diabetic Nephropathy
Diabetes is the most common cause of CKD. Before creatinine rises above normal, patients may have microalbuminuria and early glomerular damage. A creatinine trending upward from 0.7 to 1.0 over years is clinically significant even within normal range.
3. Early Hypertensive Nephrosclerosis
Hypertension causes progressive arteriolar sclerosis and glomerular ischemia. Early renal impairment may present with a creatinine at the high-normal end before crossing threshold.
4. Drugs Inhibiting Tubular Creatinine Secretion
Certain medications raise serum creatinine WITHOUT affecting actual GFR by blocking its tubular secretion:
- Trimethoprim (antibiotic)
- Cimetidine (H2 blocker)
- PARP inhibitors and tyrosine kinase inhibitors (Goldman-Cecil Medicine) This is a pharmacological, not pathological, false elevation.
5. Early Glomerulonephritis or Nephrotic Syndrome
Glomerular inflammation can modestly reduce filtration while creatinine remains in the "normal" range. Nephrotic syndrome actually increases creatinine secretion, partially masking a rise. The creatinine value alone may be deceptively reassuring.
6. Prerenal States (Mild)
Mild heart failure, mild volume depletion from GI illness, or early NSAID-induced renal vasoconstriction can marginally reduce GFR and push creatinine to high-normal without frank renal injury (Brenner & Rector's The Kidney).
7. Assay Interference (Pseudo-elevation)
The Jaffe method (colorimetric assay for creatinine) is susceptible to false elevation by:
- Acetoacetate (in diabetic ketoacidosis - can spuriously raise creatinine up to 2 mg/dL, Rosen's Emergency Medicine)
- Hyperbilirubinemia
- Certain drugs
Key Clinical Takeaway
A single creatinine value of 1.0 mg/dL cannot be interpreted in isolation. The same number means very different things in a 25-year-old male athlete versus a 70-year-old woman with diabetes and hypertension. Always calculate eGFR using the CKD-EPI equation and compare it with baseline values over time.
| Factor | Effect on Creatinine |
|---|---|
| High muscle mass | Increases (physiological) |
| Male sex | Higher baseline (physiological) |
| High protein/meat diet | Transient increase |
| Intense exercise | Transient increase |
| Dehydration | Mild increase |
| Trimethoprim/cimetidine | Blocks secretion (pharmacological) |
| Early CKD, DM nephropathy | Mildly elevated (pathological) |
| DKA/hyperbilirubinemia | Assay interference |
Sources: Morgan & Mikhail's Clinical Anesthesiology, 7e | Brenner & Rector's The Kidney, 2-Vol Set | Goldman-Cecil Medicine International Edition | Textbook of Family Medicine, 9e | Rosen's Emergency Medicine | Comprehensive Clinical Nephrology, 7th Ed
This is a shared conversation. Sign in to Orris to start your own chat.