
IMG_20260620_144503095_BURST0011.jpg
Explain benign epithlial proliferation and precursor leison (more focus on fibrocytic change)
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed for a thorough answer. Here is the complete explanation:
Benign Epithelial Proliferations and Precursor Lesions
Most benign epithelial lesions of the breast arise in the terminal duct lobular unit (TDLU) and are classified into three groups based on their risk for subsequent breast cancer development.
Overview: The Three Groups
| Category | Examples | Relative Risk of Invasive Cancer |
|---|---|---|
| Nonproliferative breast changes (fibrocystic changes) | Cysts, fibrosis, adenosis, apocrine metaplasia | 1.0 (~3% lifetime risk) |
| Proliferative disease without atypia | Usual ductal hyperplasia, sclerosing adenosis, radial scar, papilloma | 1.5-2x (~5-7%) |
| Proliferative disease with atypia | Atypical ductal hyperplasia (ADH), atypical lobular hyperplasia (ALH) | 4-5x (~13-17%) |
Most come to clinical attention as mammographic calcifications or densities, or as incidental findings.
1. Nonproliferative Breast Changes (Fibrocystic Changes) - MAIN FOCUS
These are common morphologic alterations occurring most often between 30 and 50 years of age, likely due to hormonal fluctuations during the menstrual cycle. The term "nonproliferative" denotes no increased risk of breast cancer, though this is somewhat misleading - some of these changes do involve increased proliferation and may harbor clonal genetic aberrations.
Three principal morphologic features define fibrocystic changes:
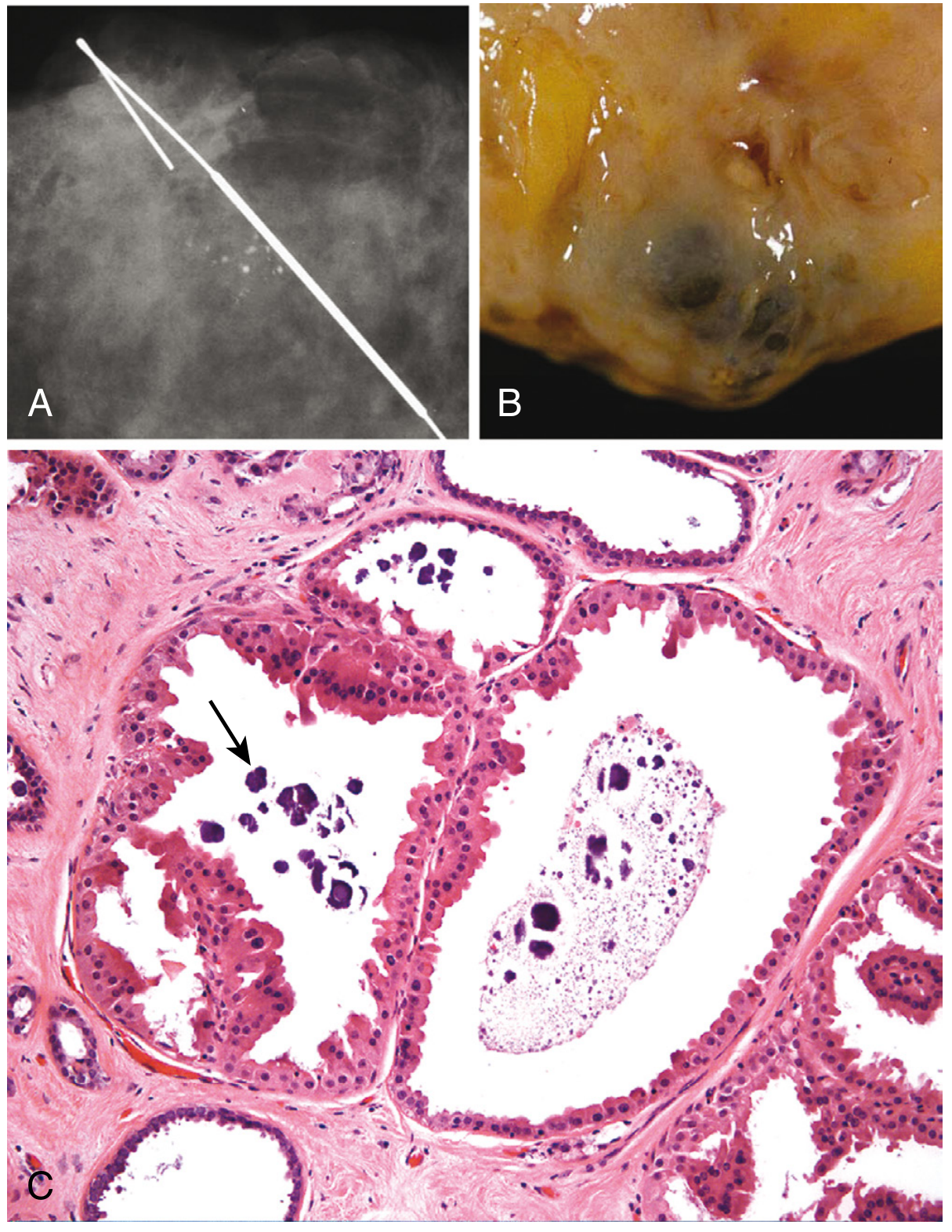
A. Cystic Change (with Apocrine Metaplasia)
- Small cysts form by dilation of lobules, which may coalesce into larger cysts
- Unopened cysts contain turbid, semitranslucent brown- or blue-colored fluid (called "blue-dome cysts")
- Cysts are lined by either flattened atrophic epithelium or metaplastic apocrine cells
- Apocrine cells have abundant granular eosinophilic cytoplasm resembling normal apocrine sweat gland epithelium
- Calcifications are common - they form on secretory debris and appear as clustered rounded densities on mammography
- Solitary, firm cysts may raise concern for malignancy; the diagnosis is confirmed by disappearance of the mass after fine-needle aspiration
B. Fibrosis
- Cysts frequently rupture, releasing secretory material into the adjacent stroma
- This triggers chronic inflammation and resultant stromal fibrosis
- The fibrosis produces the palpable nodularity characteristic of fibrocystic disease
- This is the "fibro-" component of the term "fibrocystic"
C. Adenosis
- Defined as an increase in the number of acini per lobule
- Acini are lined by columnar epithelial cells
- Calcifications are occasionally present within the lumens
- This is a lobular enlargement without compression or distortion (distinguishing it from sclerosing adenosis, which is proliferative)
Additional Nonproliferative Change: Lactational Adenoma
- Presents as a palpable mass in pregnant or lactating females
- Consists of normal-appearing breast tissue with lactational changes
- Regresses after cessation of breastfeeding
- Thought to be an exaggerated local response to gestational hormones rather than a true neoplasm
2. Proliferative Breast Disease Without Atypia
These lesions have epithelial proliferation but no cytologic atypia. They carry a 1.5-2x increased risk of cancer - they are risk predictors, not direct precursors.
-
Usual ductal hyperplasia (UDH): Increased number of both luminal and myoepithelial cells filling and distending ducts and lobules. Irregular lumens often visible at the periphery of cellular masses. Typically an incidental finding.
-
Sclerosing adenosis: Glandular proliferation with increased acini, compressed and distorted by stromal fibrosis. The compression can create solid cords or double strands of cells in dense stroma - can mimic invasive carcinoma. May present as palpable mass, radiologic density, or calcifications.
-
Radial scar (radial sclerosing lesion): Small stellate lesion that closely mimics invasive carcinoma mammographically, grossly, and histologically. Has a fibroelastic core with radiating ducts/lobules that show hyperplastic changes.
-
Papillomas: Benign epithelial growths within ducts, often causing nipple discharge.
-
Fibroadenoma with complex features: Mixed stromal and epithelial proliferation.
3. Proliferative Breast Disease With Atypia (Atypical Hyperplasia)
This group carries a 4-5x increased risk (~13-17% lifetime). The "atypia" means the cells have begun to acquire features resembling carcinoma in situ, but do not fully meet the criteria.
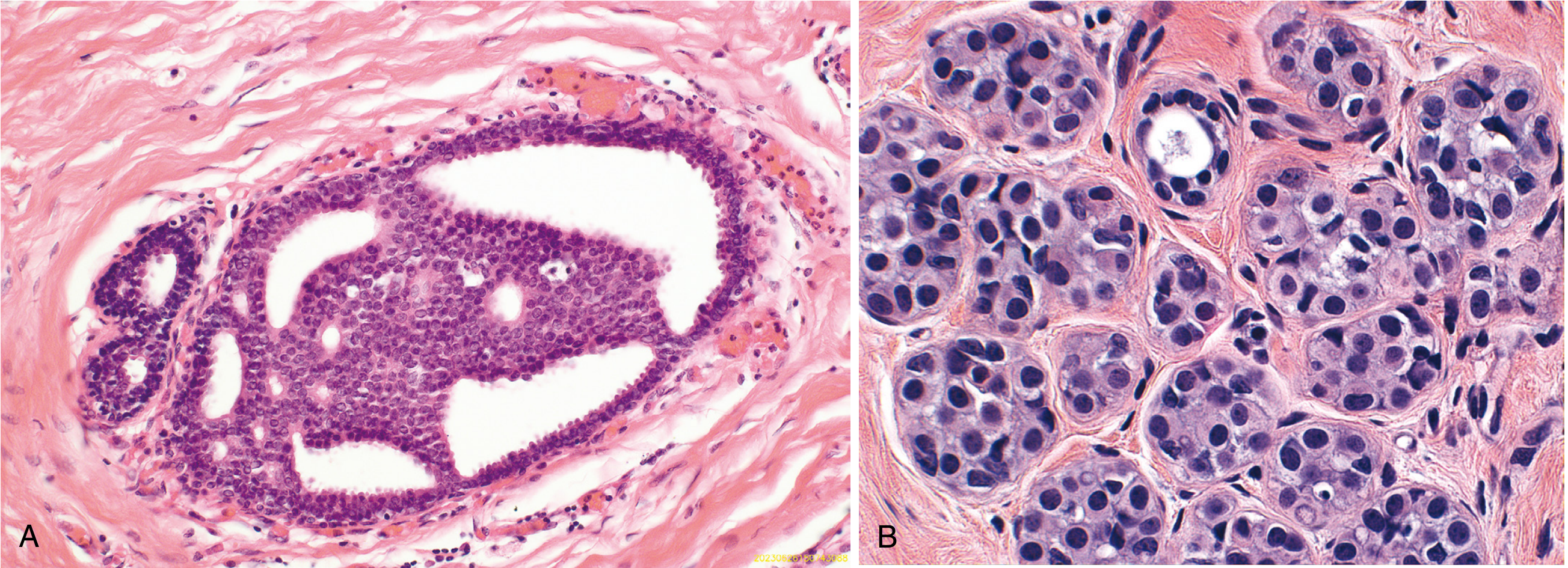
Atypical Ductal Hyperplasia (ADH):
- A duct is partially (not completely) involved by an atypical epithelial proliferation
- Comprises rounded, cytologically monotonous cells with interspersed cribriform spaces
- Shares features with low-grade DCIS but falls short of full criteria (too small, or only partial duct involvement)
Atypical Lobular Hyperplasia (ALH):
- A population of monomorphic small, round, loosely cohesive cells partially fills a lobule
- Shares cytologic features with lobular carcinoma in situ (LCIS) but does not completely fill/distend the lobule
Clinical Significance Summary
- Most benign epithelial proliferations do not cause symptoms - found as mammographic calcifications/densities or incidentally
- The majority are not precursors of cancer directly
- These lesions predict risk in either breast, not just the affected breast
- Risk reduction can be achieved by surgery or chemoprevention (e.g., tamoxifen for ADH/ALH), but most affected women undergo surveillance rather than surgery since most will not develop cancer
- Fibrocystic changes alone (nonproliferative) carry no excess cancer risk
Source: Robbins, Cotran & Kumar - Pathologic Basis of Disease, Chapter 23 (Breast), pp. 963-966
This is a shared conversation. Sign in to Orris to start your own chat.