Copd radiological findings Bronchitis vs emphysema
COPD radiology chest xray CT scan emphysema vs chronic bronchitis findings comparison
https://radiopaedia.org/articles/chronic-obstructive-pulmona…
COPD: Radiological Findings - Emphysema vs Chronic Bronchitis
Quick Reference: Classic Clinical Phenotypes
| Feature | Emphysema ("Pink Puffer") | Chronic Bronchitis ("Blue Bloater") |
|---|---|---|
| Body habitus | Thin, cachectic | Obese/stocky |
| Cyanosis | Absent/mild | Prominent |
| Productive cough | Absent | Present (defining feature) |
| Dyspnoea | Severe, at rest | Moderate |
| Cor pulmonale | Late | Early |
| CXR | Hyperinflation dominant | Increased markings dominant |
I. Emphysema
Definition & Pathology
Types (by anatomic distribution)
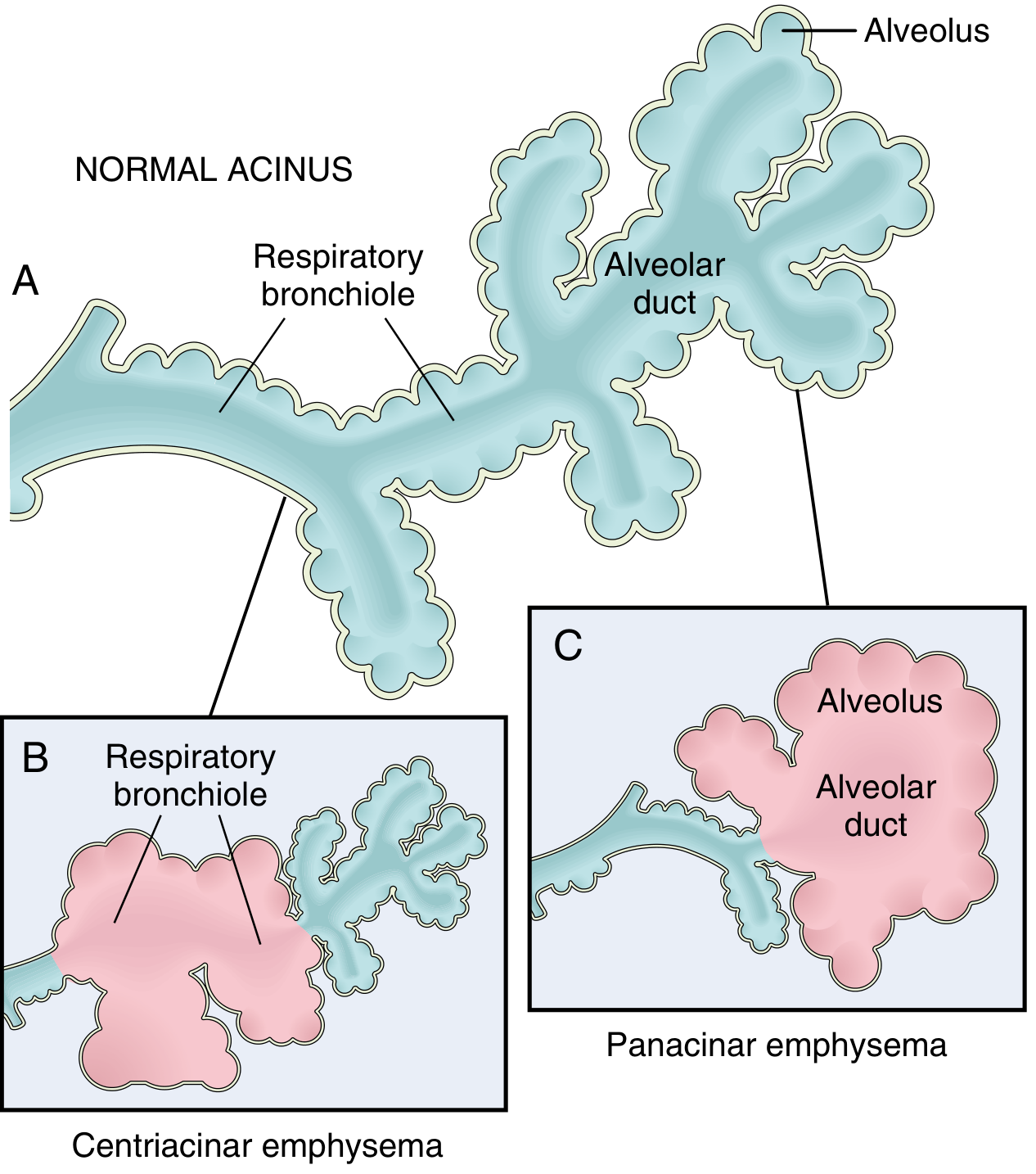
| Type | Distribution | Location | Association |
|---|---|---|---|
| Centriacinar (centrilobular) | Respiratory bronchioles (central acinus); distal alveoli spared | Upper lobes > lower lobes | Smoking (>95% of cases) |
| Panacinar (panlobular) | Entire acinus uniformly | Lower lobes > upper lobes | α1-antitrypsin deficiency |
| Paraseptal (distal acinar) | Distal acinus; adjacent to pleura/septa | Along pleura, fissures, mediastinum | Spontaneous pneumothorax in young adults |
| Irregular (paracicatricial) | Irregular, near scar tissue | Variable | Clinically insignificant |
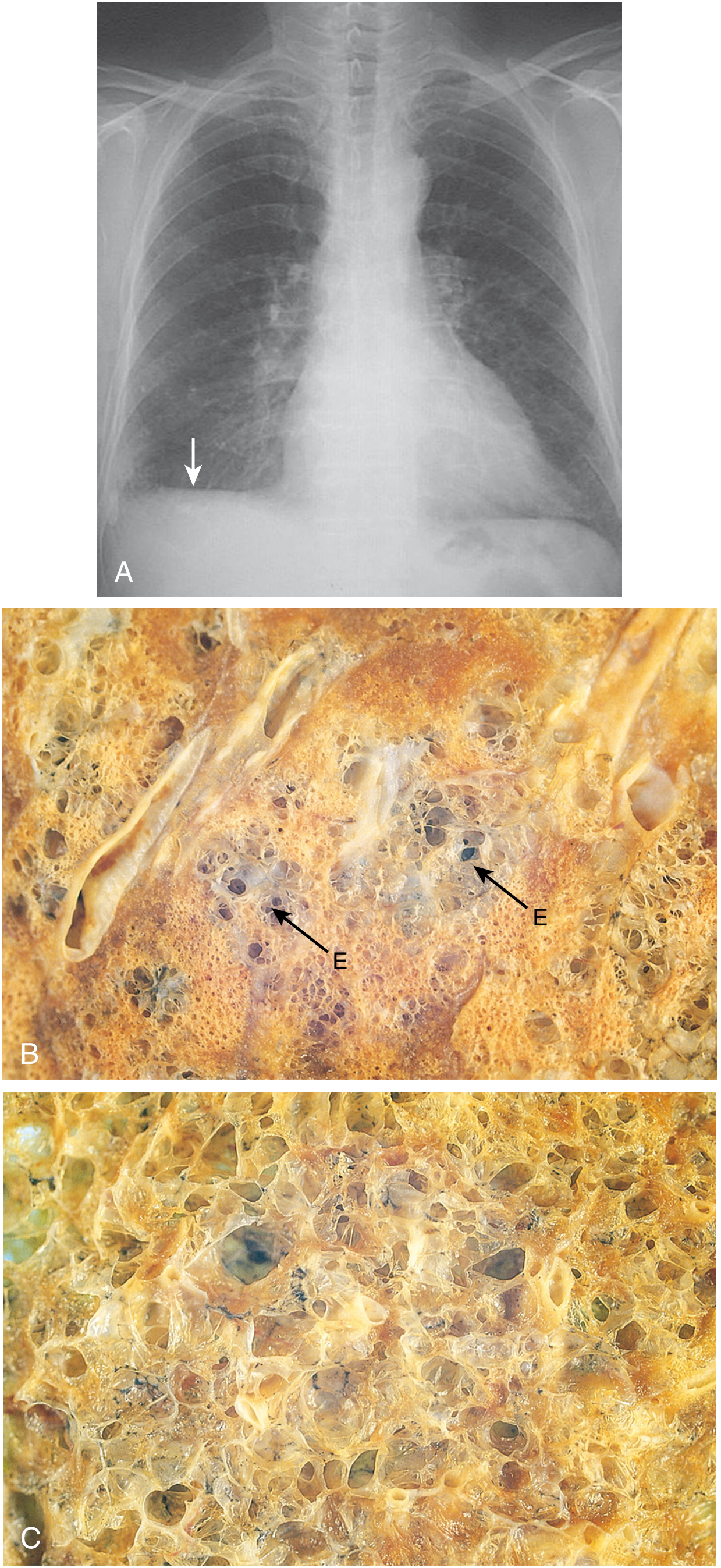
Chest X-Ray Findings in Emphysema
- Flattened hemidiaphragms (most reliable sign) - diaphragm at or below the level of the anterior 7th rib
- Barrel chest on lateral view - widened AP diameter, increased retrosternal airspace (>2.5 cm)
- Low, flat diaphragm with obtuse costophrenic angles
- Widened intercostal spaces - ribs appear more horizontal
- Hyperlucent lung fields - black, avascular-looking lungs
- Vascular pruning (oligaemia) - peripheral vascular markings absent or attenuated
- Bullae - well-defined avascular radiolucent areas (>1 cm), most prominent at apices
- Narrow, vertical ("tear-drop") heart - due to hyperinflation pushing mediastinum down
- Small heart apparent even if there is right heart enlargement
- Sabre-sheath trachea - coronal narrowing of intrathoracic trachea on PA view, with sagittal widening on lateral; ratio of coronal to sagittal tracheal diameter <0.67
CT Findings in Emphysema
- Low-attenuation areas (LAA) without visible walls - the hallmark
- Centrilobular emphysema: focal lucencies centred on the lobular core, scattered in upper lobes, often with a "dot" of the centrilobular artery visible centrally
- Panacinar emphysema: diffuse, uniform destruction - lower lobe predominant, no clear boundaries between lucencies; associated with α1-AT deficiency
- Paraseptal emphysema: subpleural lucencies arranged in rows along pleura and fissures
- Bullae (>1 cm): well-defined thin-walled airspaces; giant bullae can compress mediastinal structures
- Vascular attenuation: reduced calibre of peripheral vessels
- Gas trapping on expiratory CT: air trapping shown as mosaic attenuation pattern - areas of reduced density fail to increase in attenuation on expiration (normal lung does)
- Quantitative CT (QCT): emphysema index = % of lung voxels below -950 HU (threshold used in research/NETT trial)
II. Chronic Bronchitis
Definition & Pathology
- Mucus hypersecretion from enlarged mucus-secreting glands (Reid index >0.5)
- Goblet cell metaplasia extending into small airways
- Bronchiolar wall fibrosis and smooth muscle hyperplasia
- Chronic inflammation
Chest X-Ray Findings in Chronic Bronchitis
- Increased bronchovascular markings ("dirty chest") - thickened, irregular bronchovascular shadows; more prominent in lower zones
- Peribronchial cuffing - "tram-tracking" - parallel densities along bronchi seen end-on or en face
- Cardiomegaly - from cor pulmonale (right heart enlargement due to pulmonary hypertension)
- Mild hyperinflation (when co-existing emphysema is present)
- No significant hyperlucency or bullae (unless emphysema coexists)
CT Findings in Chronic Bronchitis
- Bronchial wall thickening (BWThick) - measured as wall area percentage (WA%): ratio of bronchial wall area to total bronchial area; WA% >60-65% considered abnormal
- "Signet ring" sign - bronchus appears larger than its accompanying artery (bronchoarterial ratio >1), opposite of normal
- Mucus plugging - bronchial luminal density filling; mucus plugs visible as hyperdense filling defects
- Bronchovascular irregularity and fibrosis from repeated inflammation
- Enlarged vessels (due to pulmonary hypertension with cor pulmonale)
- No low-attenuation areas (unless emphysema coexists)
Side-by-Side Radiological Comparison
| Sign | Emphysema | Chronic Bronchitis |
|---|---|---|
| Hyperinflation | Marked - flattened diaphragms, barrel chest | Mild or absent |
| Lung lucency | Increased (hyperlucent fields) | Normal or slightly increased |
| Vascular markings | Pruned (decreased, attenuated) | Increased/prominent ("dirty chest") |
| Bullae/blebs | Common | Absent (unless combined) |
| Cardiac silhouette | Small, narrow, vertical | Normal or enlarged (cor pulmonale) |
| Trachea | Sabre-sheath sign possible | Normal |
| CT: low attenuation areas | Present (LAAs without walls) | Absent |
| CT: bronchial walls | Normal or mildly thickened | Markedly thickened (WA% >65%) |
| CT: mucus plugging | Absent | Present |
| CT: signet ring sign | Absent | Present |
| CT: gas trapping | Mosaic pattern on expiration | Also present (air trapping in small airways) |
Combined COPD (Most Common Pattern)
- Emphysema-predominant (better DLCO loss, more hyperinflation)
- Airways-predominant (more exacerbations, productive cough)
- Mixed phenotype
Additional Radiological Features in Advanced COPD
- Pulmonary hypertension: enlarged main pulmonary artery (>29 mm on CT), right ventricular enlargement, right atrial dilatation
- Cor pulmonale: cardiomegaly with right-heart predominance on CXR, elevated pulmonary artery pressure
- ECG correlation (not imaging but related): poor R-wave progression, clockwise cardiac rotation from hyperinflation
- Complications: pneumothorax (from bullae/blebs rupturing), pneumonia, lung cancer (higher risk in emphysematous smokers)
As per the new guidelines to classify heart failure to say improved ef echo has to repeated at an intrrval of
HFimpEF heart failure improved ejection fraction classification echocardiogram interval 2021 ESC guidelines criteria
ACC AHA 2022 heart failure guidelines HFimpEF definition echocardiogram repeated interval months criteria
Bozkurt 2021 universal definition heart failure HFimpEF "3 months" OR "minimum interval" echocardiogram repeat criteria
https://heartfailure.ca/sites/default/files/papers/Universal…
HFimpEF "at least 3 months" OR "minimum 3 months" echocardiogram repeat guideline classification interval source
HFimpEF: Classification Criteria and Echo Interval
The Key Point
Official Criteria for HFimpEF
| Criterion | Requirement |
|---|---|
| Baseline LVEF | ≤40% (documented HFrEF) |
| Absolute increase | ≥10 percentage points from baseline |
| Second (follow-up) LVEF | >40% |
| Minimum echo interval | Not specified in guidelines |
Why "3 Months" Is Commonly Cited
- GDMT optimisation: Most guideline-directed medical therapy (beta-blockers, ACEi/ARBi/ARNI, MRA, SGLT2i) takes 3-6 months to show maximal EF improvement. Repeating echo too early may underestimate recovery.
- TRED-HF trial (referenced in 2022 ACC/AHA guidelines): Demonstrated 44% relapse within 6 months of stopping GDMT in dilated cardiomyopathy patients with apparent recovery - supporting the recommendation to continue GDMT in HFimpEF and monitor over months.
- Practical monitoring: The 2022 ACC/AHA guidelines recommend echo reassessment 3-6 months after initiating/optimising GDMT in HFrEF to assess response - this is the source of the "3 months" teaching point.
ESC 2021 Position
Bottom Line for Exams
HFimpEF (per 2021 Universal Definition / 2022 ACC/AHA/HFSA): Prior LVEF ≤40%, follow-up LVEF >40%, with ≥10-point absolute increase. No specific echo time interval is mandated. In practice, echo is typically repeated after 3-6 months of optimised GDMT. The commonly tested answer is "3 months" when a number is asked, reflecting standard GDMT re-evaluation timing.