What about endotracheal intubation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
In thus what is use of guarde wire
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Here is a complete answer on the use of the guidewire (bougie) in endotracheal intubation:
Guidewire / Gum Elastic Bougie in Endotracheal Intubation
The illustration from the textbook shows exactly what you're asking about:
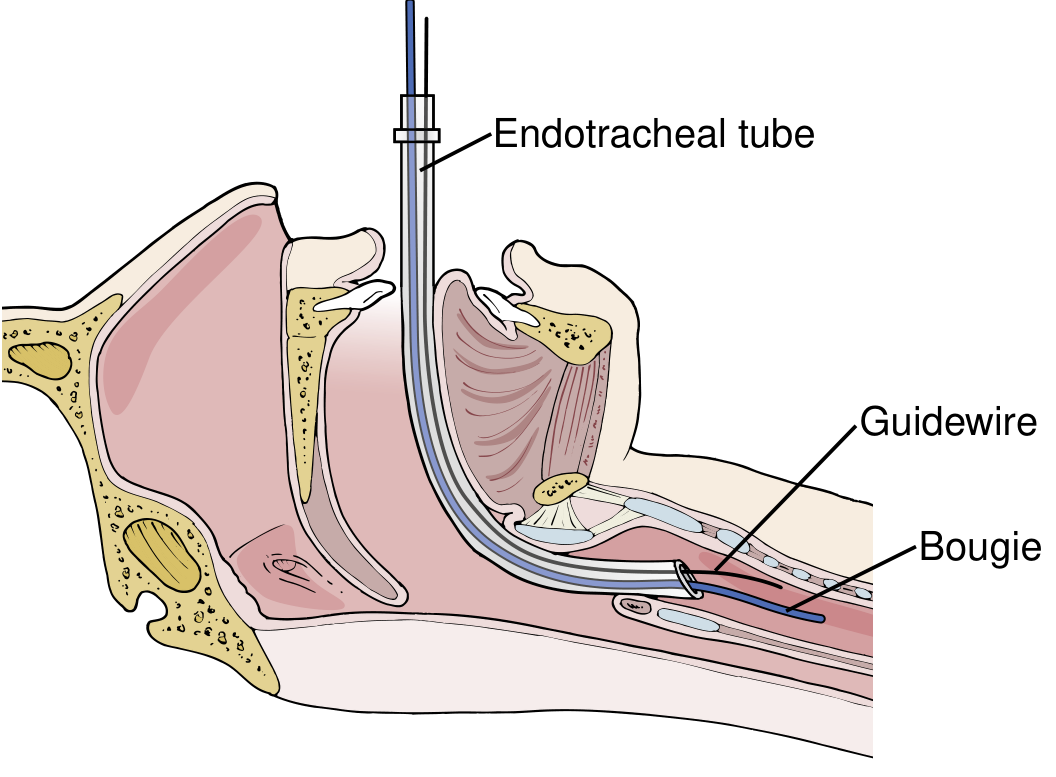
FIG. 5 - Gum elastic bougie insertion with the endotracheal tube being advanced over it into the trachea.
What is it?
In intubation, the "guidewire" refers to the gum elastic bougie (also called a tracheal tube introducer). It is:
- A flexible, 60 cm long, 15 French introducer
- Has a Coude tip - angled at 40 degrees, 3.5 cm from the distal end
- Made of a semi-rigid woven material coated in resin
Why is it Used? (Main Purpose)
The bougie is used specifically in difficult airways - when direct laryngoscopy gives a poor view. This is classified using the Cormack-Lehane grading system:
| Grade | View | Action |
|---|---|---|
| 1-2 | Full or partial cords visible | Direct intubation possible |
| 3-4 | Only arytenoids/epiglottis seen, or nothing | Bougie needed |
When you can only see the arytenoids or epiglottis (but NOT the vocal cords), you cannot safely pass the ET tube directly - so the bougie goes in first.
Step-by-Step Technique
- Lubricate the bougie
- Insert with the Coude tip directed anteriorly (toward the trachea, not the esophagus)
- Advance until it reaches the level of the tracheal rings
- Confirm tracheal placement - you feel "clicks" or tracheal ring clicks (vibrations/reverberation) as the tip passes over the tracheal cartilage rings. If it goes into the esophagus, no clicks are felt
- Hold the bougie in place - then advance the endotracheal tube over the bougie (like a rail) through the vocal cords and into the trachea
- Remove the bougie once the ET tube is in position
- Confirm placement as usual - end-tidal CO2, bilateral breath sounds, chest rise
Key Clinical Points
- It acts like a rail or track that guides the ET tube into a trachea you cannot directly see
- The Coude angled tip helps it "hook" anteriorly into the trachea
- Tracheal ring clicks = correct position in trachea
- No clicks + tube advances >40 cm without resistance = esophageal placement (stop immediately)
- It is especially valuable in trauma patients where in-line cervical stabilization limits the laryngoscopic view
- Studies show bougie use gives a higher first-attempt success rate compared to a stylet alone, particularly for less experienced operators
As noted in Current Surgical Therapy 14e, the bougie is the go-to rescue device for Cormack-Lehane grade 3 or 4 views, and in Fischer's Mastery of Surgery, it is described as a key part of the difficult airway algorithm before escalating to supraglottic devices or a surgical airway.
This is a shared conversation. Sign in to Orris to start your own chat.