flowchart on management of solitary thyroid nodule based on Cummings
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I have everything I need - the original Cummings flowchart image and all the surrounding text. Here is the complete answer:
Management of Solitary Thyroid Nodule - Cummings (Fig. 122.9)
Below is the original algorithm directly from Cummings Otolaryngology Head and Neck Surgery:
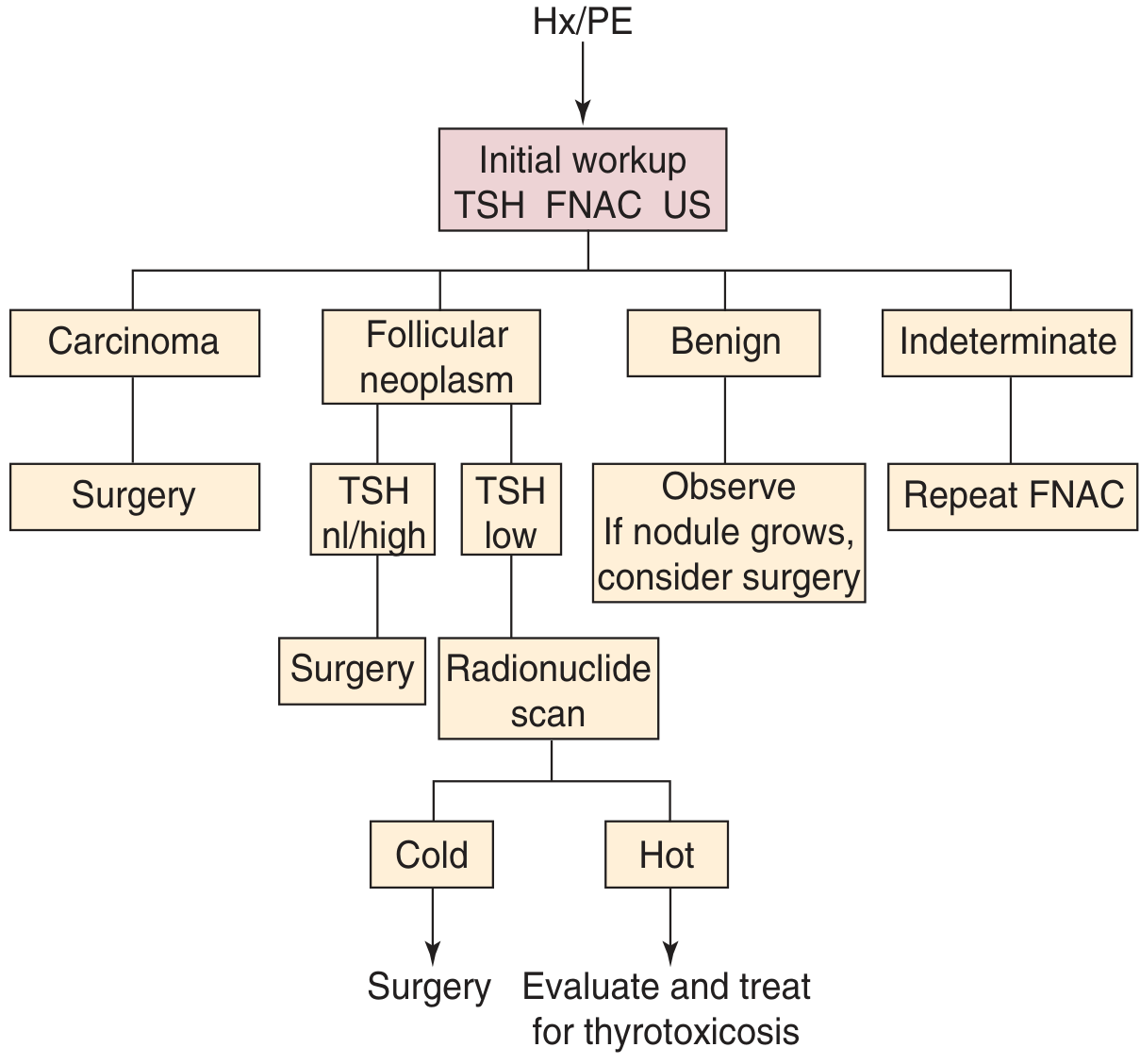
Fig. 122.9 - Cummings Otolaryngology Head and Neck Surgery
Step-by-Step Breakdown of the Algorithm
Step 1 - History & Physical Examination (Hx/PE)
Evaluate for high-risk features that may indicate surgery without further workup:
- Age < 20 years or elderly male
- History of head/neck radiation
- Rapid nodule growth
- Compressive/invasive symptoms: hoarseness, dysphagia, dyspnea
- Fixation of the nodule
- Family history of thyroid carcinoma, MEN syndrome
Step 2 - Initial Workup: TSH + FNAC + Ultrasound (US)
| Investigation | Purpose |
|---|---|
| TSH | Determines functional status (hyper/hypo/euthyroid) |
| FNAC | Primary diagnostic tool for cytology |
| Ultrasound | Characterizes nodule, guides FNAC, evaluates nodal basins |
Step 3 - Branch by TSH Status (before FNAC in certain cases)
| TSH Status | Action |
|---|---|
| Suppressed (low TSH) | Radionuclide scan to rule out toxic hot nodule |
| Elevated (high TSH) | Treat hypothyroidism first, then do FNAC |
| Normal TSH | Proceed directly to FNAC |
Step 4 - Branch by FNAC Result
A. Carcinoma (diagnostic/strongly suggestive)
- → Surgery (well-differentiated thyroid carcinoma)
- Anaplastic carcinoma and lymphoma require additional workup to determine treatment modality
B. Follicular Neoplasm
- Cannot distinguish adenoma from carcinoma on FNAC alone (capsular/vascular invasion needed)
- If TSH normal/high → Surgery
- If TSH low → Radionuclide scan:
- Cold nodule → Surgery
- Hot nodule → Evaluate and treat for thyrotoxicosis
C. Benign
- → Observe (close clinical and US monitoring)
- If nodule grows → consider surgery
D. Indeterminate (15-30% of FNA specimens)
- → Repeat FNAC (preferably US-guided)
- Molecular marker testing options:
- Afirma Gene Expression Classifier - high NPV (93%), best as "rule-out" test
- ThyroSeq - high NPV (~95%), also a "rule-out" test
- ThyGenX/ThyraMIR - highest PPV (~66%), used as "rule-in" test
- Atypia/follicular lesion of undetermined significance (AUS/FLUS): 5-10% malignancy risk
Key Points from Cummings
- Only ~5% of thyroid nodules are carcinoma; ~1 in 200 is lethal
- Palpable nodules ≥ 1 cm warrant full workup
- Radionuclide scanning is not routinely done; reserved for hyperthyroid patients or post-indeterminate FNAC
- Ultrasound guidance should be used for repeat FNAC after indeterminate results
- Surgery is indicated for well-differentiated thyroid carcinoma; anaplastic carcinoma and lymphoma need additional assessment
Source: Cummings Otolaryngology Head and Neck Surgery, Chapter 122, pp. 2374-2377
management of nodule with low ash
Reading File
Reading File
I have all the information needed from Cummings. Here is the focused answer:
Management of Thyroid Nodule with Low TSH (Suppressed TSH)
(Assuming "low ash" = low TSH - the suppressed TSH pathway in the Cummings algorithm)
Why TSH Matters First
A suppressed serum TSH indicates hyperthyroidism and shifts the workup away from FNAC as the first step. The low TSH signals that the nodule may be autonomously functioning (hot), which is almost never malignant. Proceeding directly to FNAC in this setting risks missing a toxic nodule and is not the preferred first step.
Step-by-Step Management (Cummings Algorithm)
Thyroid Nodule + LOW TSH
↓
Radionuclide Scan
(¹²³I or ⁹⁹ᵐTc pertechnetate)
↓
┌─────────────────┐
↓ ↓
HOT nodule COLD nodule
(hyperfunctioning) (non-functioning)
↓ ↓
Evaluate and Surgery
treat for
thyrotoxicosis
HOT Nodule (Autonomously Hyperfunctioning)
- Concentrates tracer on scan; suppresses rest of gland
- Virtually never malignant - FNAC is not required
- Treat the thyrotoxicosis:
- Antithyroid drugs (carbimazole/methimazole) for symptom control
- Radioactive iodine (¹³¹I) - definitive therapy
- Surgery (thyroid lobectomy) - if large nodule, compressive symptoms, or patient preference
- Also called Marine-Lenhart syndrome when a functioning nodule coexists with Graves disease
COLD Nodule (Non-Functioning) in Low-TSH Patient
- Does not concentrate tracer
- Higher malignancy risk than hot nodule
- → Surgery is indicated (proceed as per follicular neoplasm pathway)
- FNAC may be performed pre-operatively to guide surgical extent
Additional Notes from Cummings
- ¹²³I is preferred over ⁹⁹ᵐTc because it provides a true measure of iodine uptake, not just trapping
- ⁹⁹ᵐTc is cheaper and faster (no 2-day wait) but does not confirm organification
- Radionuclide scanning is not part of routine nodule evaluation - it is reserved specifically for the low TSH scenario (or post-indeterminate FNAC)
- The combination of low TSH + FNAC results can be misleading if done in sequence incorrectly - always scan first in the hyperthyroid patient
Source: Cummings Otolaryngology Head and Neck Surgery, Chapter 122, pp. 2374-2376
does thyroid gland have true and false capsule
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Excellent - multiple authoritative sources confirm the answer clearly. Here is the complete response:
Does the Thyroid Gland Have a True and False Capsule?
Yes. The thyroid gland is surrounded by two distinct capsular layers - an inner true (fibrous) capsule and an outer false (surgical) capsule.
1. True Capsule (Internal / Fibrous Capsule)
- A thin, densely adherent fibrous layer that is derived from the stroma of the gland itself
- Closely applied to and inseparable from the thyroid parenchyma
- Sends vascularized connective tissue septa inward, dividing the gland into pseudolobules (larger and smaller lobules)
- At the posteromedial surface, it condenses to form Berry's ligament (posterior suspensory ligament), which attaches the gland firmly to the cricoid cartilage and upper 2-3 tracheal rings
- Because of this firm attachment via Berry's ligament, the thyroid moves with swallowing
2. False Capsule (External / Surgical Capsule)
- Formed by the pretracheal layer of the deep cervical fascia (middle layer of cervical fascia) - it is NOT a true capsular structure of the gland itself
- Tougher than the true capsule
- Also called the "surgical capsule" because it defines the plane of dissection during thyroidectomy
The Space Between the Two Capsules
This is the most surgically important zone:
| Contents |
|---|
| Loose connective tissue (surgical dissection plane) |
| Parathyroid glands (posterior portion) |
| Recurrent laryngeal nerve |
| Larger branches of thyroid vessels |
"The space between the loosely adherent capsular layers is filled with loose connective tissue and contains larger branches of vessels, as well as the parathyroid gland in its posterior portion."
- Color Atlas of Human Anatomy, Vol. 2
This is why during thyroidectomy, dissection within this inter-capsular plane (close to the true capsule) helps preserve the parathyroids and RLN, which lie outside the true capsule but inside the false capsule.
Clinical Significance
| Feature | True Capsule | False Capsule |
|---|---|---|
| Origin | Gland stroma | Pretracheal fascia |
| Adherence | Tightly adherent to gland | Loosely adherent |
| Septa | Yes - divides gland into lobules | No |
| Berry's ligament | Formed by it | Not involved |
| Surgical relevance | Defines extent of gland | Defines surgical plane |
| Contents between layers | - | Parathyroids, RLN, vessels |
- Extrathyroidal extension in thyroid cancer is defined as tumor breaching the true capsule
- T3b staging = invasion beyond the true capsule into strap muscles
- T4a = invasion through the false capsule into surrounding structures (larynx, trachea, esophagus, RLN)
Sources: Color Atlas of Human Anatomy Vol. 2 (p. 592); Schwartz's Principles of Surgery 11e (p. 1654); Fischer's Mastery of Surgery 8e (p. 1052)
give a detailed essay answer on ENT manifestations of thyroid disease
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.