Regulation of bloop pressure mbbs 1st year physiology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Regulation of bloop pressure mbbs 1st year physiology guyton
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from Guyton covering all major topics. Let me compile the full response:
Regulation of Blood Pressure
Guyton and Hall Textbook of Medical Physiology | MBBS 1st Year Physiology
The Basic Equation
Blood pressure is governed by:
Mean Arterial Pressure (MAP) = Cardiac Output (CO) × Total Peripheral Resistance (TPR)
This single equation is the foundation of all pressure-regulating mechanisms. Any mechanism that raises or lowers MAP does so by acting on CO, TPR, or both. Note that CO and TPR are not independent - when one changes, the other partially compensates, so doubling TPR does not double MAP.
Normal MAP ≈ 100 mm Hg. The body uses two broad systems to keep MAP at this set-point:
- Short-term (seconds to minutes): Neural mechanisms
- Long-term (days to weeks): Renal-body fluid + hormonal mechanisms
PART 1 - Short-Term Neural Regulation
1. The Vasomotor Center
Located bilaterally in the reticular substance of the medulla and lower pons, the vasomotor center is the master control hub of cardiovascular regulation.
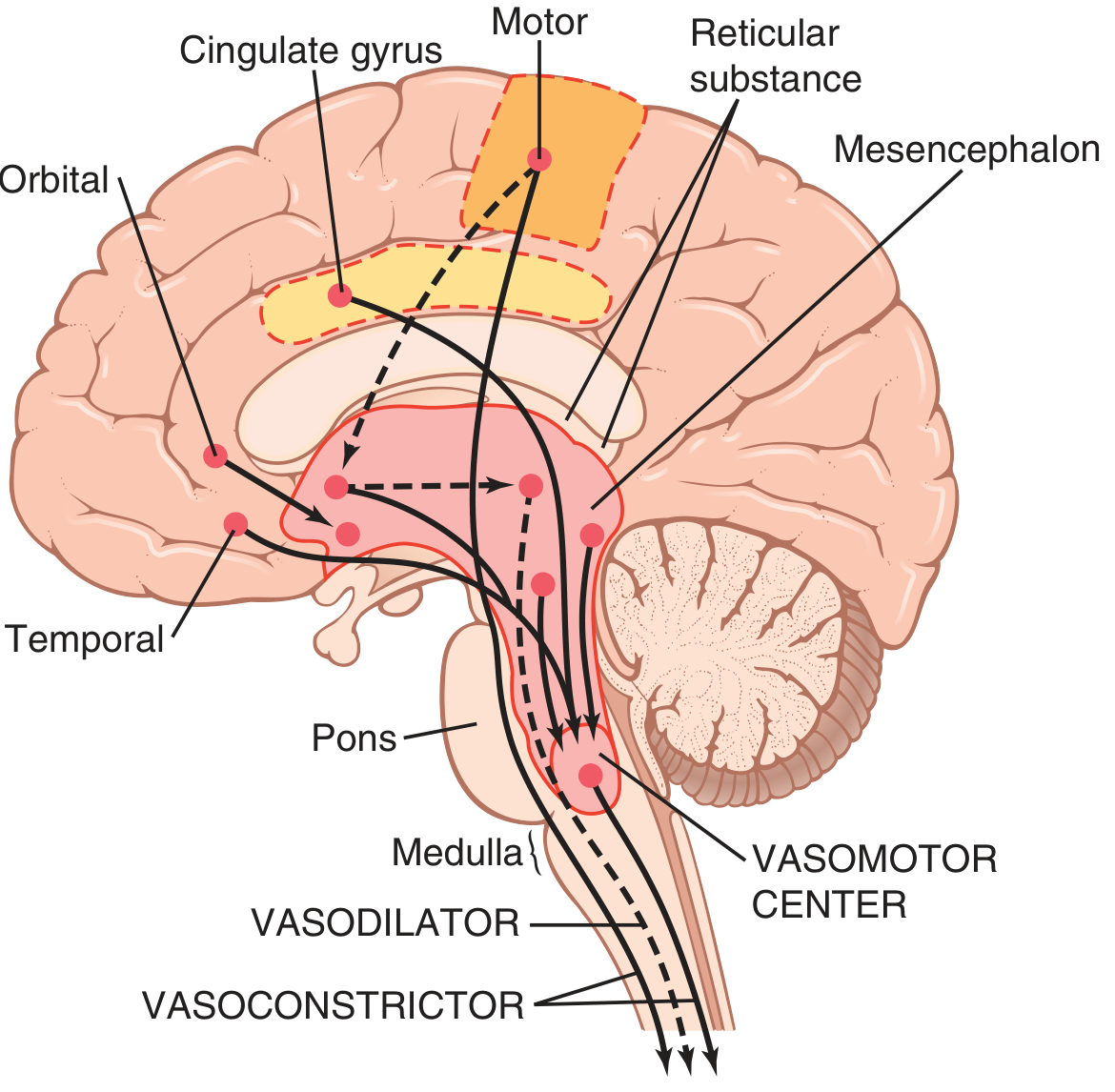
It has three functional zones:
| Zone | Location | Function |
|---|---|---|
| Vasoconstrictor area | Anterolateral upper medulla | Sends excitatory fibers to sympathetic preganglionic neurons → vasoconstriction |
| Vasodilator area | Anterolateral lower medulla | Projects to vasoconstrictor area, inhibiting it → vasodilation |
| Cardioinhibitory area | Medulla | Sends parasympathetic (vagal) signals to slow heart rate |
Higher centers - cortex, hypothalamus, mesencephalon - can modify vasomotor center output (hence emotional stress raises BP).
2. Sympathetic Nervous Control
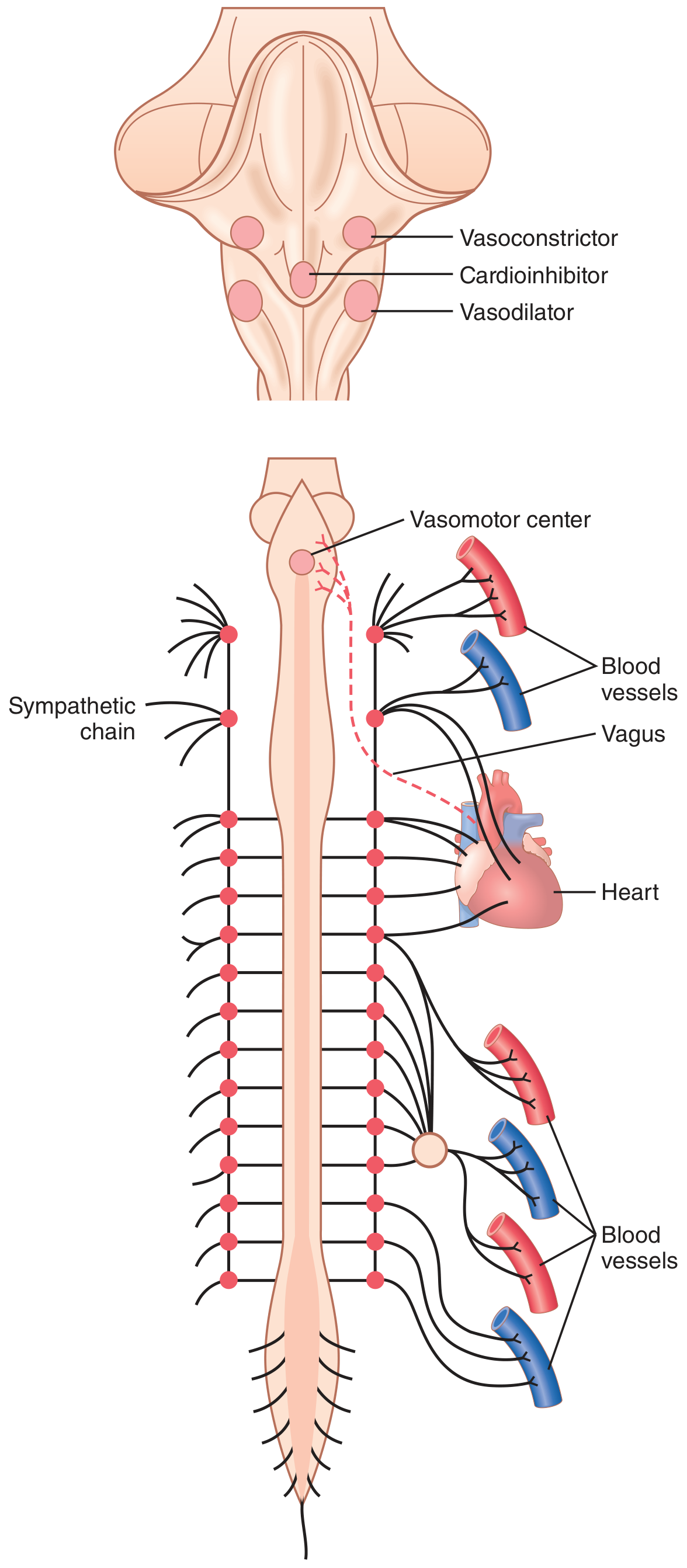
- Sympathetic vasomotor fibers exit via thoracic and L1-L2 spinal nerves → sympathetic chain → blood vessels
- Innervate all vessels except capillaries (especially arterioles, small arteries, veins)
- Effect on arterioles: ↑ resistance → ↑ TPR → ↑ MAP
- Effect on veins: ↓ venous capacitance → ↑ venous return → ↑ CO → ↑ MAP
- Direct cardiac sympathetic fibers: ↑ HR and contractility → ↑ CO
Parasympathetics (vagus) mainly slow the heart rate and have minimal effect on blood vessels.
3. The Baroreceptor Reflex (Most Important Short-Term Mechanism)
This is a negative-feedback reflex that operates within seconds.
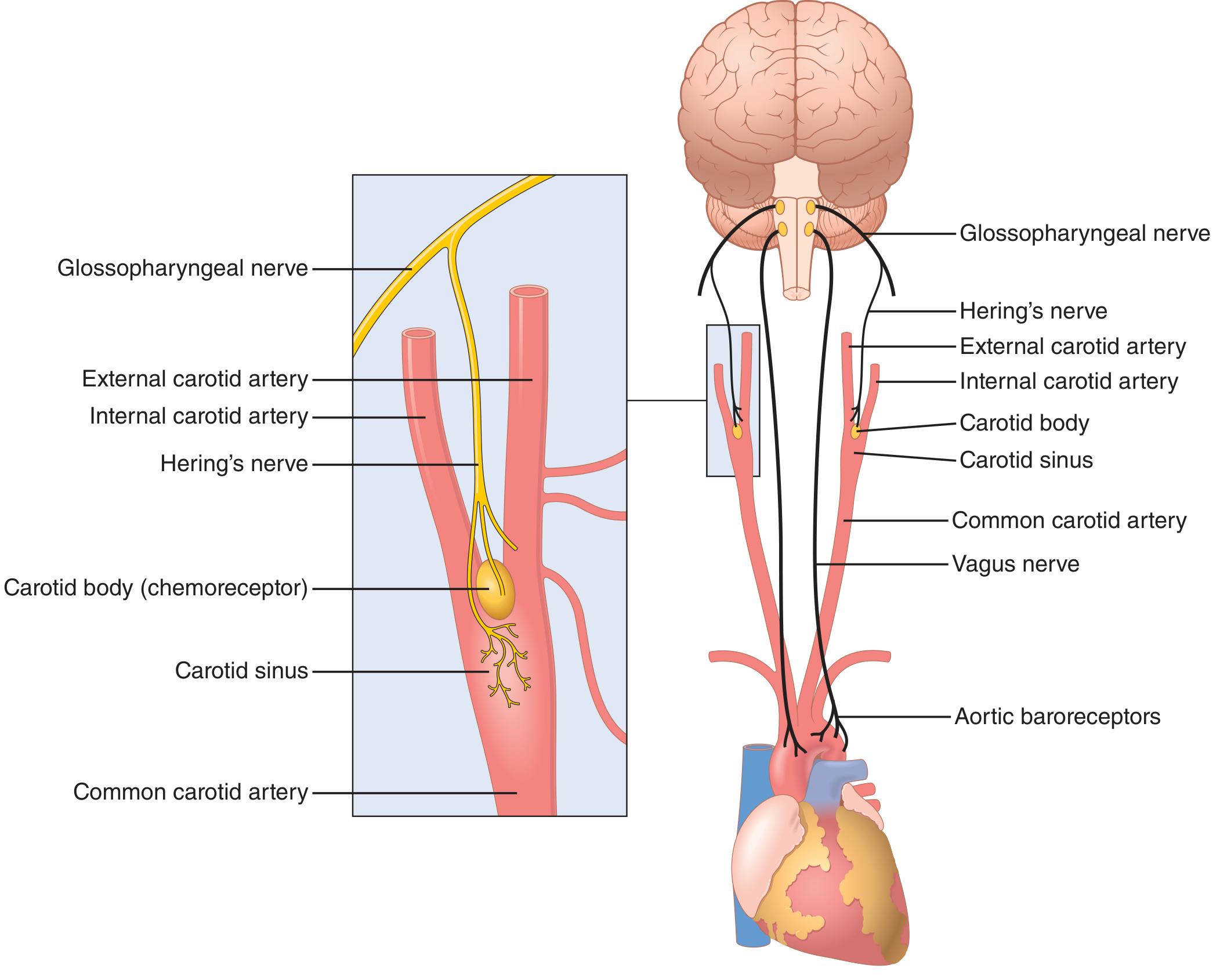
Receptor Locations
- Carotid sinus - wall of internal carotid artery just above bifurcation (most sensitive)
- Aortic arch - wall of the aorta (operates ~30 mmHg higher than carotid)
- Also: thoracic arteries, right and left subclavian arteries
Afferent Pathway
- Carotid sinus → Hering's nerve → Glossopharyngeal nerve (CN IX) → Nucleus Tractus Solitarius (NTS) in medulla
- Aortic arch → Vagus nerve (CN X) → same NTS
Response Characteristics
- No firing below 50-60 mmHg; maximum firing at ~180 mmHg
- Most sensitive in the normal range (around 100 mmHg) - even a small pressure change causes strong reflex response
- Responds more strongly to rapidly changing pressure than to static pressure
Reflex Response: Rise in BP → Baroreceptors Stretched →
↑ Baroreceptor firing
→ NTS activated
→ Vasoconstrictor center inhibited + Cardioinhibitory center activated
→ ↓ Sympathetic outflow + ↑ Parasympathetic (vagal) outflow
→ ↓ HR, ↓ contractility (↓ CO) AND Vasodilation (↓ TPR)
→ BP returns toward normal
The reverse occurs with a fall in BP: ↓ baroreceptor firing → ↑ sympathetic outflow → vasoconstriction + tachycardia → BP rises.
Buffer Function
Baroreceptors act as pressure buffers - they dampen fluctuations in BP during changes of posture, exercise, hemorrhage, etc. They are not the primary long-term regulators (they adapt/"reset" within 1-2 days if pressure is chronically elevated, as in hypertension).
4. Chemoreceptor Reflex (Secondary Neural Mechanism)
Peripheral chemoreceptors: Carotid and aortic bodies, located near their respective baroreceptors.
- Sensitive to ↓ PO₂, ↑ PCO₂, ↓ pH in blood
- Signals travel alongside baroreceptor afferents to NTS
- Stimulation → ↑ vasomotor center activity → vasoconstriction → ↑ MAP
Central chemoreceptors: In the medulla
- Respond to ↑ CO₂ / ↓ pH in CSF
Chemoreceptors primarily regulate respiration but secondarily regulate BP. They become important especially when MAP falls below 80 mmHg (when O₂ delivery to chemoreceptors decreases).
5. CNS Ischemic Response ("Last-Ditch Mechanism")
When blood flow to the vasomotor center itself is severely reduced (MAP < 60 mmHg):
- CO₂ and acid accumulate in medullary tissue
- This powerfully excites the vasoconstrictor and cardioaccelerator neurons
- Can raise MAP to as high as 250 mmHg for up to 10 minutes
- Does not operate under normal conditions - it is an emergency mechanism only
Cushing Reaction: A specific form where ↑ CSF pressure compresses cerebral arteries → brain ischemia → CNS ischemic response → ↑ MAP to restore cerebral perfusion.
6. Low-Pressure Receptors (Atrial and Pulmonary Artery Stretch Receptors)
Located in the walls of atria and pulmonary arteries; detect volume changes (low-pressure side).
- When blood volume rises → atria stretched → reflex:
- ↓ Renal sympathetic activity
- ↓ ADH secretion from hypothalamus
- ↑ ANP (atrial natriuretic peptide) release
- → ↑ renal salt and water excretion → ↓ blood volume → ↓ MAP
Bainbridge Reflex: Atrial stretch → ↑ HR (when background HR is slow). This helps the heart keep up with increased venous return.
PART 2 - Long-Term Regulation: Renal-Body Fluid System
The renal mechanism is the most powerful and dominant regulator of long-term MAP. It operates over days to weeks and is the ultimate determinant of where MAP settles chronically.
Core Principle: Pressure Diuresis and Pressure Natriuresis
- ↑ MAP → ↑ urine output (pressure diuresis) + ↑ sodium excretion (pressure natriuresis)
- ↓ Blood volume → ↓ venous return → ↓ CO → ↓ MAP → back toward set-point
- At 50 mmHg: urine output ≈ 0; at 100 mmHg: normal; at 200 mmHg: 4-6× normal
- The chronic renal output curve is much steeper than the acute curve - small chronic pressure rises produce large increases in fluid excretion
Long-term MAP is determined by the intersection of:
- The renal output curve (salt/water excretion vs. MAP)
- The salt and water intake level
If either shifts, MAP settles at a new equilibrium. This is why kidney disease causes hypertension, and why a low-salt diet lowers BP.
Renin-Angiotensin-Aldosterone System (RAAS)
The most important hormonal modifier of the renal-body fluid system:
↓ Renal perfusion pressure / ↓ Na⁺ delivery to macula densa / ↑ sympathetic activity
→ Renin released from juxtaglomerular (JG) cells
→ Renin cleaves Angiotensinogen (liver) → Angiotensin I
→ ACE (lung) → Angiotensin II
Angiotensin II effects:
- Direct vasoconstriction (↑ TPR → ↑ MAP) - most potent endogenous vasoconstrictor
- Stimulates aldosterone secretion from adrenal cortex → ↑ Na⁺ and water retention → ↑ blood volume → ↑ MAP
- Stimulates ADH → ↑ water reabsorption
- Stimulates thirst center
In hypertension, RAAS blockers (ACE inhibitors, ARBs) are used precisely because they interrupt this volume-pressure loop.
Summary Table: Timeline of Regulation
| Mechanism | Speed | Primary Action |
|---|---|---|
| Baroreceptor reflex | Seconds | ↓ HR, vasodilation |
| Chemoreceptor reflex | Seconds-minutes | Vasoconstriction |
| CNS ischemic response | Seconds (emergency) | Massive vasoconstriction |
| Atrial/pulmonary reflexes | Minutes | ↑ Renal fluid excretion |
| RAAS | Minutes-hours | Vasoconstriction + fluid retention |
| Renal-body fluid system | Days-weeks | Pressure natriuresis/diuresis |
Key Points to Remember for MBBS Exams
- MAP = CO × TPR - all mechanisms work through CO, TPR, or both
- Baroreceptor reflex is the most important short-term mechanism; responds within seconds; fibers travel via CN IX and CN X to NTS in medulla
- Baroreceptors are located in the carotid sinus and aortic arch; most sensitive at ~100 mmHg
- Baroreceptors reset in chronic hypertension - they do not provide long-term control
- Renal-body fluid system is the ultimate long-term control; infinite gain - if working normally, can return MAP exactly to set-point
- RAAS amplifies renal control; Angiotensin II is the key vasoconstrictor hormone
- CNS ischemic response = last-ditch emergency, activates only when MAP < 60 mmHg
Sources: Guyton and Hall Textbook of Medical Physiology - Chapters 18 & 19
This is a shared conversation. Sign in to Orris to start your own chat.