Give me a full clinical case, prescription, diagnostic tests, its results etc for a collis fracture
Reading File
Finding Sources
Finding Sources
Searching the Web
Colles fracture clinical case management diagnosis treatment 2024
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
I now have comprehensive data from multiple authoritative textbooks. Let me compile the full clinical case.
Full Clinical Case: Colles' Fracture
Patient Presentation
Patient: Mrs. Amelia Hartley, 68-year-old right-handed retired schoolteacher
Setting: Emergency Department
Chief Complaint: Right wrist pain and deformity after a fall
History of Present Illness
Mrs. Hartley slipped on a wet floor at home and fell forward, instinctively extending her right hand to break the fall (FOOSH - Fall Onto OutStretched Hand) with the wrist in dorsiflexion. She felt immediate sharp pain in the right wrist, followed by rapidly developing swelling and visible deformity. She denies any neck pain, shoulder pain, or head injury. She is unable to move the wrist due to pain. She has no sensory changes in her fingers at this time.
PMH: Type 2 Diabetes (metformin-controlled), known osteoporosis (diagnosed 2 years ago, on alendronate), hypertension
Medications: Metformin 500 mg BD, Alendronate 70 mg weekly, Amlodipine 5 mg OD, Calcium + Vitamin D supplement
Allergies: Penicillin (rash)
Social History: Non-smoker, occasional alcohol, lives alone
Physical Examination
| System | Finding |
|---|---|
| General | Alert, in moderate distress, cradling right arm |
| Vitals | BP 145/88, HR 96, RR 16, SpO2 98% RA, Temp 36.8°C |
| Right wrist | "Dinner fork deformity" - dorsal prominence just proximal to the wrist with a step-off, volar depression; swelling and ecchymosis over the dorsal and lateral wrist |
| Tenderness | Maximal over distal radius, ~1.5 cm proximal to the articular surface; ulnar styloid also tender |
| ROM | Grossly limited - patient unable to flex, extend, or rotate wrist |
| Neurovascular | Radial pulse 2+, capillary refill < 2 sec in all digits; sensation intact in radial, ulnar, and median nerve distributions; grip strength reduced but present |
| Skin | Intact, no open wounds |
The classic "dinner fork deformity" occurs because the distal radial fragment is displaced dorsally and proximally, creating a visible step when viewed from the side.
Diagnostic Tests
1. Plain X-Ray Wrist (PA and Lateral Views) - PRIMARY INVESTIGATION
This is the definitive first-line test.
PA (Posteroanterior) View findings:
- Transverse fracture of the distal radial metaphysis, approximately 1.8 cm from the articular surface
- Shortening of the radius (radial shortening ~4 mm)
- Loss of radial inclination (normal: 22-23 degrees; reduced to ~14 degrees)
- Negative ulnar variance (ulna appearing relatively longer)
- Associated fracture of the ulnar styloid (present in ~60% of cases)
- No intraarticular extension on this view
Lateral View findings:
- Dorsal angulation of the distal radial articular surface: ~18 degrees (normal volar tilt is +11 degrees; the fragment has reversed to -18 degrees of dorsal tilt)
- Dorsal displacement and comminution of the dorsal cortex
- Classic "dinner fork" profile
Radiographic criteria confirming a Colles' fracture:
- Dorsal angulation of the plane of the distal radius
- Distal fragment displaced proximally and dorsally
- Radial displacement of the carpus
- Ulnar styloid fracture
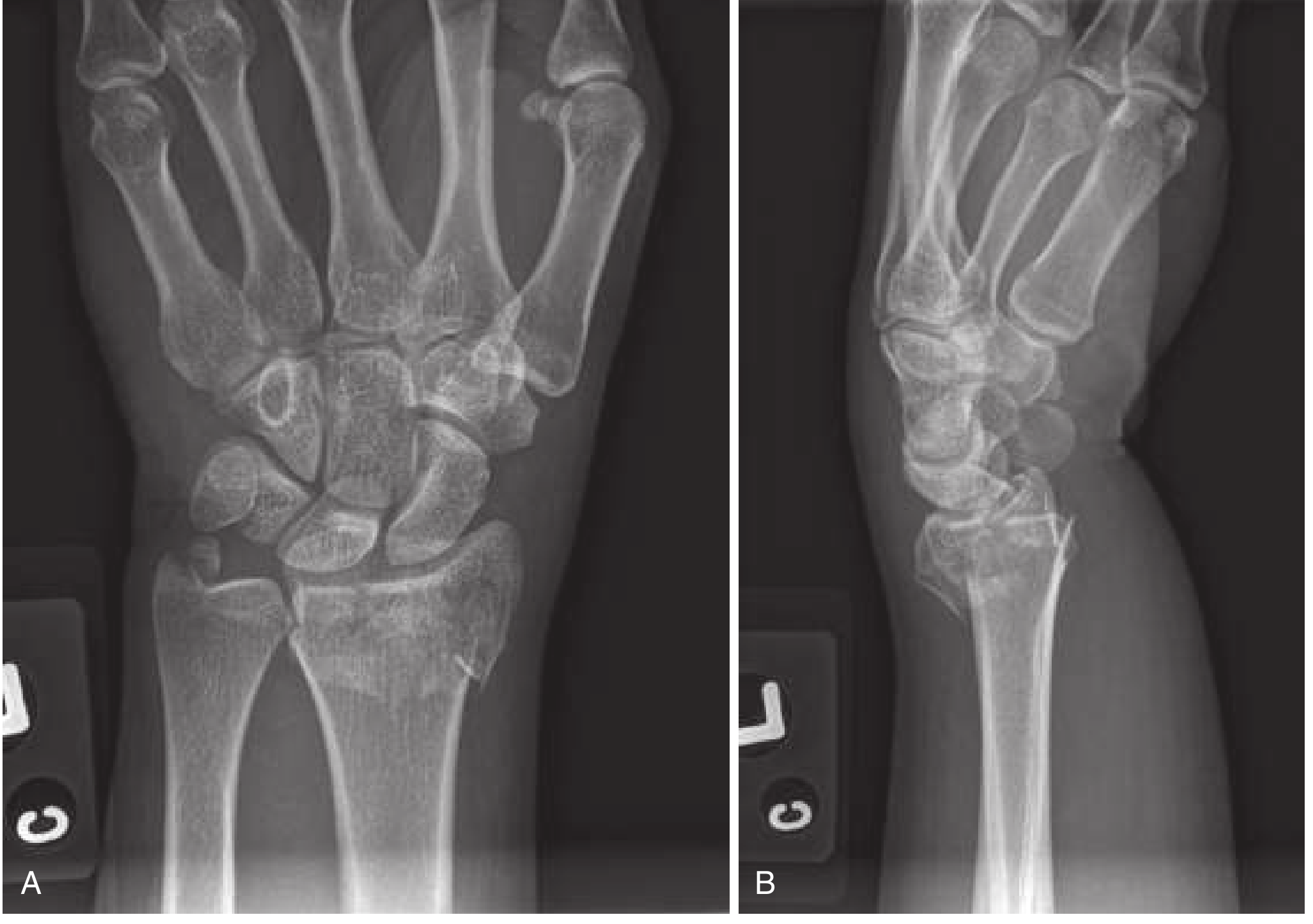
Rosen's Emergency Medicine, Fig. 43.24 - PA view shows fracture, radial shortening, intraarticular extension, and associated ulnar styloid fracture. Lateral view shows dorsal displacement and angulation.
2. CT Wrist (Ordered After X-Ray Review)
Ordered because lateral X-ray shows significant comminution and there is concern for intraarticular extension.
CT Findings:
- Extra-articular distal radius fracture confirmed; no intraarticular step-off
- Dorsal comminution of the cortex
- No radioulnar joint instability
- Ulnar styloid fracture confirmed - at the base (Type II, may affect TFCC stability)
- No carpal fractures
Per Tintinalli's: "If the fracture has significant intra-articular extension, or comminution, or if distal radioulnar joint instability is suspected, CT may provide important additional information for diagnosis and treatment."
3. Neurovascular Check (Clinical Test - Pre and Post Reduction)
| Nerve | Test | Pre-Reduction | Post-Reduction |
|---|---|---|---|
| Median nerve | Sensation over thenar eminence, index/middle finger | Intact | Intact |
| Radial nerve | Sensation dorsum web space; wrist extension | Intact | Intact |
| Ulnar nerve | Sensation little finger; finger abduction | Intact | Intact |
| Vascular | Radial pulse, capillary refill | 2+, < 2 sec | 2+, < 2 sec |
4. Blood Tests
Ordered because of patient's age, osteoporosis history, and pre-operative consideration:
| Test | Result | Reference Range | Interpretation |
|---|---|---|---|
| FBC | Hb 12.1, WBC 7.4, Plt 210 | Normal | Normal pre-op baseline |
| BMP / U&E | Na 138, K 4.1, Cr 84, eGFR 68 | eGFR mildly reduced | Important for analgesia dosing |
| Blood glucose | 8.2 mmol/L | 4-7 fasting | Mild diabetic elevation |
| HbA1c (recent, 3 months ago) | 7.1% | < 7% | Suboptimal glycaemic control - affects healing |
| DEXA scan (prior) | T-score: -2.8 (hip), -3.1 (lumbar spine) | T-score < -2.5 = osteoporosis | Severe osteoporosis confirmed - risk factor |
| Vitamin D | 42 nmol/L | > 50 nmol/L | Mild deficiency - impacts fracture healing |
| PTH | 68 pg/mL | 15-65 pg/mL | Mildly elevated - secondary hyperparathyroidism |
| Coagulation (PT/INR, APTT) | Normal | Normal | Pre-procedural baseline |
Diagnosis
Right Colles' fracture - extra-articular, dorsally angulated (18 degrees), with dorsal comminution, radial shortening (4 mm), and associated ulnar styloid fracture (base).
Classification: AO/OTA 23-A3 (extra-articular, comminuted)
Background: Fragility fracture on a background of severe osteoporosis (T-score -3.1).
Management
Step 1 - Analgesia (Immediate)
- Morphine 2.5 mg IV titrated (reduced dose for eGFR 68)
- Elevate the limb; apply ice pack wrapped in cloth
Step 2 - Closed Reduction (Performed in ED)
Indicated because:
- Dorsal angulation >neutral position (18 degrees dorsally angulated)
- Radial shortening (4 mm)
- Active patient in dominant hand
Hematoma Block Technique:
A 22-gauge needle is inserted on the dorsum of the distal radius over the fracture site. The fracture hematoma is aspirated (blood confirms correct placement), then 8 mL of 1% lidocaine is injected slowly into the hematoma space.
Per Rosen's EM: "The hematoma block remains an easy and effective method of anesthesia and may be performed by placing a 22-gauge needle in the dorsum of the distal radius, withdrawing until a fracture hematoma is encountered and then instilling 5 to 10 mL of 1% or 2% lidocaine."
Reduction Manoeuvre:
- Finger traps applied to the index and middle fingers; countertraction via a cuff around the upper arm
- Traction applied for 5-10 minutes to relax forearm musculature and disengage the fracture
- The distal fragment is pushed distally and volarly (palmarly) while the forearm is stabilised
- Anatomic volar tilt is restored; goal is at least 0 degrees (neutral) or positive volar tilt
Post-Reduction X-ray Results:
- Dorsal angulation corrected to +4 degrees of volar tilt (restored to neutral/slightly volar)
- Radial length restored; ulnar variance now positive
- Acceptable reduction achieved
Step 3 - Immobilisation
Double Sugar-Tong Splint applied immediately after reduction (NOT a circumferential cast - to allow for swelling):
- First slab: from elbow to wrist (dorsal/volar)
- Second slab: extends from elbow to axilla over the first slab
- Wrist held in slight flexion and ulnar deviation
- Fingers free to move
Per Pfenninger & Fowler's: "If extra-articular and nondisplaced, it can be treated with a double sugar-tong splint for 3 to 5 days followed by a short-arm cast for 4 to 6 weeks."
Arm sling applied. Patient instructed to begin finger range-of-motion exercises immediately to reduce stiffness and oedema.
Prescription
EMERGENCY DEPARTMENT PRESCRIPTION
Patient: Amelia Hartley | DOB: 12/03/1958 | MRN: 7842310
Allergies: Penicillin (rash)
Date: 12/07/2026
1. Paracetamol (Acetaminophen) 1 g PO every 6 hours
(Regular analgesia - first line)
2. Ibuprofen 400 mg PO TDS with food for 5 days
[NOTE: Use with caution given eGFR 68 - short course only;
monitor renal function; omit if GI upset develops]
3. Codeine Phosphate 30 mg PO every 4-6 hours PRN
(Breakthrough pain - max 240 mg/24 hrs; avoid if drowsy)
4. Omeprazole 20 mg PO OD
(Gastroprotection while on NSAID)
5. Baclofen 5 mg PO TDS PRN
(Muscle spasm relief if needed)
---
Osteoporosis / Fragility Fracture Management:
6. Continue: Alendronate 70 mg PO weekly (existing prescription)
[Note: Ensure taken on empty stomach with full glass of water;
remain upright for 30 mins]
7. Colecalciferol (Vitamin D3) 1000 IU PO OD
(Supplement - Vitamin D level 42 nmol/L; target >75 nmol/L)
8. Calcium Carbonate 1000 mg PO BD
(Bone health - ongoing)
---
Thromboprophylaxis:
9. Aspirin 75 mg PO OD for duration of immobilisation
(DVT prophylaxis; may upgrade to LMWH if mobility severely
reduced or if surgical fixation is required)
Prescriber: Dr. C. Rahman (ED Registrar)
Date: 12/07/2026
Follow-Up Plan
| Timeframe | Action |
|---|---|
| 24-48 hours | Urgent orthopaedic outpatient review; repeat X-ray in splint |
| Day 3-5 | Convert sugar-tong splint to short arm cast (once swelling reduces) |
| Week 1 | Repeat X-ray in cast - check no loss of reduction |
| Week 2 | Repeat X-ray - check alignment |
| Week 6 | X-ray after cast removal - assess union; refer to physiotherapy |
| 6-8 weeks | Begin supervised wrist physiotherapy (ROM, strengthening) |
| 3 months | Orthopaedic follow-up for full functional assessment |
| 6 months | Endocrinology/rheumatology referral for osteoporosis optimisation (consider denosumab or teriparatide given T-score -3.1 and fragility fracture) |
Indications for Surgery (Not Met in This Case, But Would Apply If:)
- Dorsal angulation > 20 degrees post-reduction
- Radial shortening > 5 mm
- Articular step-off > 2 mm (intraarticular fracture)
- Severely comminuted, unstable fracture
- Open fracture
- Neurovascular compromise not resolving
- Dominant hand in high-demand active patient with inadequate reduction
Surgical options include: percutaneous K-wires (Kirschner wires), volar locking plate (most common in active patients), or external fixation for open/severely comminuted fractures.
Complications to Monitor
| Complication | Timing | Notes |
|---|---|---|
| Carpal tunnel syndrome / Median nerve injury | Acute or delayed | Most common complication; assess with Tinel's / Phalen's tests at each visit |
| Malunion | Weeks | Risk if reduction is lost; follow X-ray series essential |
| TFCC injury | Acute | Ulnar styloid base fracture raises concern; consider MRI wrist at 6 weeks if ulnar-sided pain persists |
| Complex Regional Pain Syndrome (CRPS) | Weeks-months | Burning pain, allodynia, vasomotor changes; more common in women |
| Extensor pollicis longus (EPL) tendon rupture | Weeks-months | Late complication from tendon attrition on fracture callus |
| Distal radioulnar joint (DRUJ) instability | Late | Related to ulnar styloid fracture at base; may need repair |
| Stiffness | Weeks | Early finger ROM exercises, physiotherapy critical |
Per Tintinalli's EM: "A wide range of complications occur in 6% to 80% of cases... The most common complication is immediate or delayed carpal tunnel syndrome... Factors associated with long-term disability or instability include dorsal angulation ≥20 degrees and ≥5 mm of radial shortening."
Discharge Education
- Keep the splint dry at all times.
- Elevate the arm above heart level to reduce swelling (use a pillow when lying down).
- Move all fingers actively several times per hour to prevent stiffness.
- Return immediately if: increasing pain under the cast, numbness or tingling in fingers, skin colour changes (white/blue), inability to move fingers, fever, or splint feels too tight.
- Do not drive or lift anything with the right arm until cleared by the orthopaedic surgeon.
- Review osteoporosis management with your GP to prevent future fragility fractures.
Sources: Rosen's Emergency Medicine (9th Ed.) | Tintinalli's Emergency Medicine (9th Ed.) | Pfenninger & Fowler's Procedures for Primary Care (3rd Ed.) | Schwartz's Principles of Surgery (11th Ed.)
This is a shared conversation. Sign in to Orris to start your own chat.