Skin flap physiology from Cummings
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Now I have all the essential content. Let me compile the comprehensive answer.
Skin Flap Physiology — Cummings Otolaryngology Head and Neck Surgery
Core Principle
The most important determinant of flap success is vascular supply. All flaps — pedicled or free tissue transfer — depend on maintaining adequate perfusion to meet the metabolic demands of mobilized tissue. The distal flap is both the most critical for defect coverage and the most likely to fail.
Physics of Flow
Flow (Q) in a vessel is governed by the Hagen-Poiseuille equation:
Q = πr⁴(ΔP) / 8ηl
- r⁴ = fourth power of vessel radius (dominant factor)
- ΔP = perfusion pressure = P_diastolic − P_tissue
- η = dynamic viscosity
- l = vessel/flap length
Perfusion pressure (PP) = Diastolic BP − Tissue pressure
All clinical efforts target two goals: maintain normal PP and minimize resistance to flow.
| Factor | Clinical Action |
|---|---|
| Systemic BP | Avoid hypotension and vasoconstriction |
| Tissue pressure | Avoid excess tension, edema, fluid overload |
| Vessel radius | Base flaps on large named vessels; use flap delay; free tissue transfer |
| Blood viscosity | Maintain hydration; target low-normal hematocrit |
| Flap length | Longer flaps = more resistance = greater risk of distal necrosis |
Critical Closing Pressure
Critical closing pressure is the point at which tissue pressure exceeds intracapillary pressure, causing capillary collapse and cessation of flow.
- In rigid tubes, flow rises linearly with pressure (Hagen-Poiseuille)
- In distensible blood vessels, flow rises exponentially with pressure (LaPlace's law)
- When tissue pressure rises above capillary pressure → vessels collapse → flow stops
LaPlace's law also explains why wider vessels dilate preferentially and how collateral flow develops over time (rationale for flap delay).
Effect of Flap Length on Viability
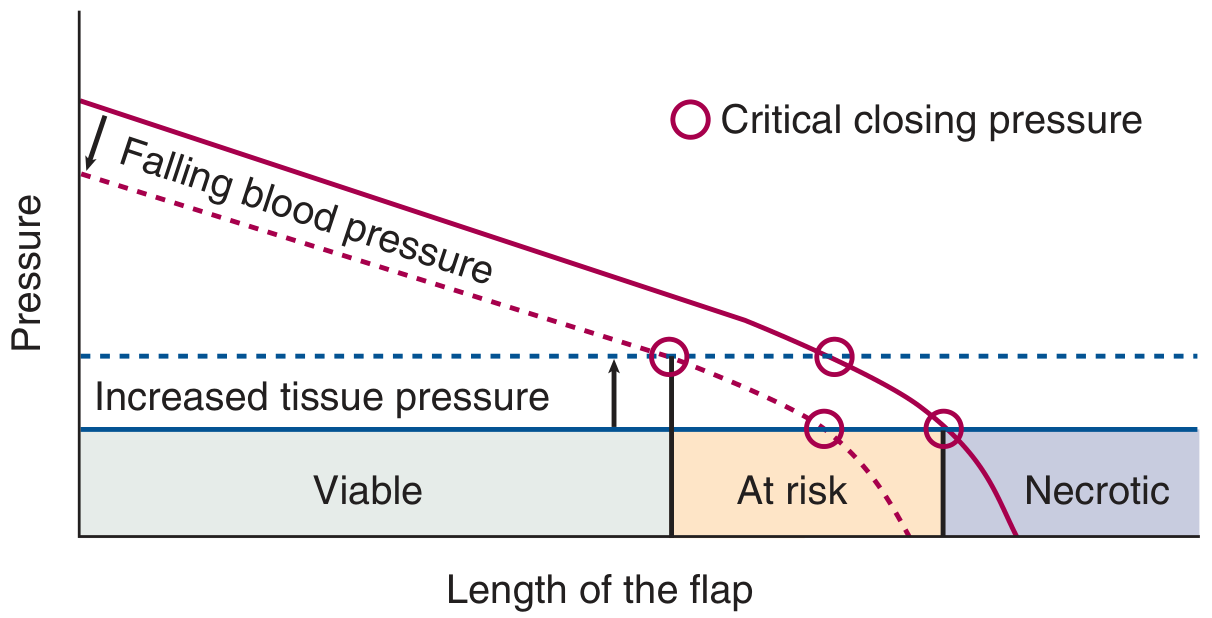
Fig. 77.1 — As flap length increases, perfusion pressure falls. Where it intersects the critical closing pressure threshold, the flap becomes "at risk," then "necrotic." Falling systemic BP or rising tissue pressure shifts this intersection proximally.
Key myth dispelled: A wider base in a random flap adds vessels with the same perfusion pressure — it does NOT change the relationship between perfusion pressure and critical closing pressure, and does NOT increase survival length.
Zones of Perfusion
Flap perfusion is conceptualized in three zones:
| Zone | Compartment | Key Determinants |
|---|---|---|
| Zone I — Macrocirculatory | Large vessels, pedicle, anastomosis | Systemic BP, vessel patency |
| Zone II — Microcirculatory | Arterioles, capillaries, venules | Tissue pressure, sphincter tone, A-V shunts |
| Zone III — Interstitial | Extracellular matrix, lymphatics | Starling forces, edema, diffusion distances |
Zone II — Microcirculation
- Terminal arterioles → metarterioles → precapillary sphincters → capillary beds
- Arteriovenous shunts allow direct arteriole→venule bypass (thermoregulation)
- Preshunt sphincters: regulate thermoregulation & systemic BP via vasoactive substances
- Precapillary sphincters: regulate nutritive (capillary) blood flow
- Elevated interstitial pressure compresses capillaries → decreased flow
- Autoregulation = normalization of capillary flow in response to pressure changes
- Lymphatics run parallel to blood capillaries; impaired by inflammation and loss of pulsation
Zone III — Interstitial System
- Filled with proteoglycans, collagen, hyaluronic acid filaments — high resistance to fluid movement in normal hydration
- Fluid movement occurs by two mechanisms:
- Diffusion — dominant for small molecules; distance increases with edema → ↓ nutrient delivery
- Convective flow (bulk flow) — fluid swept along microchannels; large molecules use this route
Starling equation governs transcapillary flow:
Jv/A = Lp[(Pi − Pi) − σ(πi − πi)]
Where Lp = membrane water permeability, P = hydrostatic pressures, π = osmotic pressures, σ = osmotic (reflection) coefficient.
Classification of Flaps by Vascular Supply
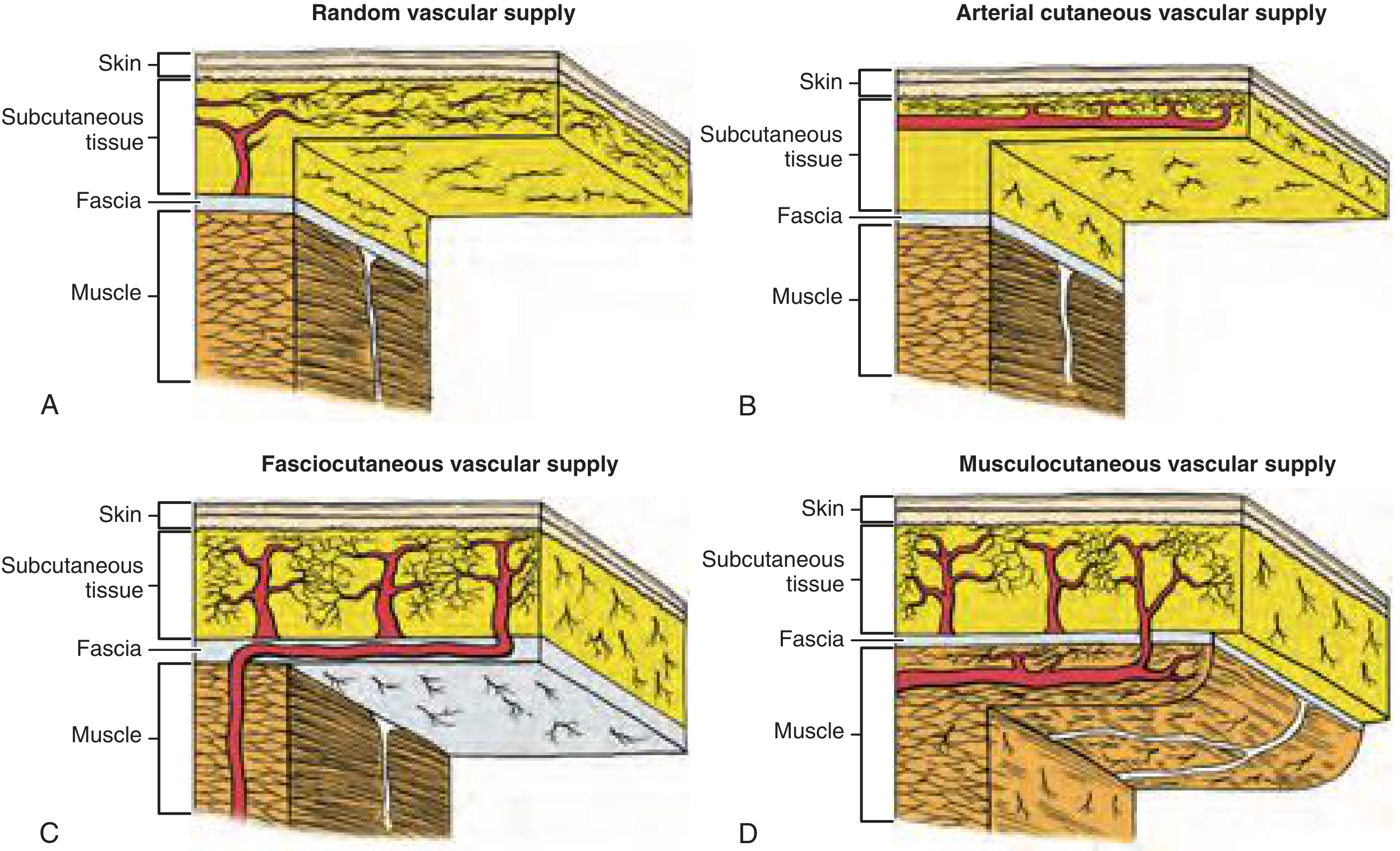
Fig. 77.5 — (A) Random, (B) Arterial cutaneous (axial), (C) Fasciocutaneous, (D) Musculocutaneous
| Flap Type | Blood Supply | Plane of Dissection | Notes |
|---|---|---|---|
| Random cutaneous | Subdermal plexus from unnamed musculocutaneous perforators | Subcutaneous fat | Survival = function of PP, NOT length:width ratio |
| Arterial (axial) cutaneous | Named septocutaneous artery along longitudinal axis | Must include septocutaneous vessel | Better survival than random; distal extension = random territory |
| Fasciocutaneous | Septocutaneous vessels → deep fascial plexus → subdermal plexus | Deep fascia included | Relies on skin vascular territories; 4 subtypes based on fascial supply pattern |
| Musculocutaneous / Myocutaneous | Segmental vessels to muscle → musculocutaneous perforators | Muscle incorporated | Best survival; leaves local perforators intact; named for donor muscle |
Examples in H&N:
- Deltopectoral flap — anterior perforators of internal mammary artery
- Paramedian forehead flap — supratrochlear vessels
- Pectoralis myocutaneous flap — pectoral branch of thoracoacromial artery
- Latissimus dorsi flap
Flap Failure
Failure is most detectable by the time it is irreversible — hence early monitoring is critical in at-risk cases.
Monitoring and salvage by zone:
| Zone | Monitoring | Salvage |
|---|---|---|
| Zone I (macrocirculatory) | Doppler, near-infrared spectroscopy, temperature | Explore pedicle/anastomosis; thrombosis treatment |
| Zone II (microcirculatory) | Doppler, tissue oxygenation, tissue pressure | Vascular washout; reduce edema |
| Zone III (interstitial) | Clinical assessment | Address Starling forces, reduce edema |
Risk factors for failure: diabetes, prior irradiation, hypotension, excess tension, edema.
Methods to Augment Flap Survival
Flap Delay
- Creates collateral flow by preliminary interruption of part of the blood supply
- Dilates remaining vessels via LaPlace's law over time
- Extends viable flap length
Hyperbaric Oxygen (HBO)
- Increases blood oxygen-carrying capacity by ~20% (oxygen dissolved in plasma)
- Greater benefit when hematocrit is low
- Also increases oxygen diffusion from perfused surrounding tissue into ischemic zones
- Beneficial effects: ↓ leukocyte adherence, ↓ edema (vasoconstriction effect), ↑ neovascularization in irradiated tissue
- Must be given early — little benefit if >24 hours after flap elevation
- HBO challenge test: transcutaneous O₂ rise ≥50 mmHg predicts successful outcome
- Not cost-effective for every flap; reserve for high-risk cases
Source: Cummings Otolaryngology Head and Neck Surgery, Chapter 77 — Skin Flap Physiology (pp. 1388–1395)
Make a ppt
Reading File
Reading File
Reading File
Running Command
ls /home/daytona/workspace/ 2>/dev/null || echo "workspace is empty"
Running Command
mkdir -p /home/daytona/workspace/skin-flap-ppt && node /home/daytona/skills/shar…
Writing File
~/skin-flap-ppt/generate.js
const pptxgen = require("pptxgenjs");
const { execSync } = require("child_process");
// Fetch images
const images = JSON.parse(execSync(
`node /home/daytona/skills/shared/scripts/fetch_images.js ` +
`"https://cdn.orris.care/cdss_images/d0a512d589cd28d792911d65f39b832f4c28f68db7b1f5c791afa3e2267bd9bc.png" ` +
`"https://cdn.orris.care/cdss_images/4849dcb2ef6c4152e12631aca3798c9760b67d2a3336332ed02be715a1ece884.png"`
).toString());
const imgFlap = images[0].base64;
const imgClass = images[1].base64;
// Color palette — deep surgical blue & warm anatomical tones
const C = {
bg: "0D1B2A", // deep navy
panel: "162436", // slightly lighter navy for cards
accent: "E63946", // surgical red accent
gold: "F4A261", // warm gold for highlights
teal: "2EC4B6", // teal for sub-accents
white: "FFFFFF",
offwhite: "E8EEF4",
grey: "8FA3B1",
lightblue: "A8DADC",
};
let pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.title = "Skin Flap Physiology";
pres.author = "Cummings Otolaryngology";
// ─── Helper: slide background ─────────────────────────────────────────────
function addBg(slide) {
slide.background = { color: C.bg };
}
// ─── Helper: accent bar top ───────────────────────────────────────────────
function addTopBar(slide, accent = C.accent) {
slide.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 10, h: 0.08,
fill: { color: accent }, line: { color: accent }
});
}
// ─── Helper: section label pill ──────────────────────────────────────────
function pill(slide, label, x, y, w = 2.5, color = C.accent) {
slide.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x, y, w, h: 0.32,
fill: { color }, line: { color }, rectRadius: 0.08
});
slide.addText(label, {
x, y, w, h: 0.32,
fontSize: 9, bold: true, color: C.white,
align: "center", valign: "middle", margin: 0
});
}
// ─── Helper: card box ─────────────────────────────────────────────────────
function card(slide, x, y, w, h, fillColor = C.panel) {
slide.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x, y, w, h,
fill: { color: fillColor },
line: { color: "1E3A50", width: 0.5 },
rectRadius: 0.1,
shadow: { type: "outer", color: "000000", blur: 8, offset: 2, angle: 135, opacity: 0.3 }
});
}
// ─── SLIDE 1: TITLE ──────────────────────────────────────────────────────
{
let s = pres.addSlide();
addBg(s);
// Bold red accent bar left
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 0.18, h: 5.625,
fill: { color: C.accent }, line: { color: C.accent }
});
// Subtle anatomy illustration background shape
s.addShape(pres.shapes.RECTANGLE, {
x: 5.5, y: 0, w: 4.5, h: 5.625,
fill: { color: "0A1520" }, line: { color: "0A1520" }
});
// Title
s.addText("Skin Flap", {
x: 0.6, y: 1.2, w: 5, h: 0.9,
fontSize: 52, bold: true, color: C.white,
fontFace: "Calibri", charSpacing: 2
});
s.addText("Physiology", {
x: 0.6, y: 2.05, w: 5, h: 0.9,
fontSize: 52, bold: true, color: C.accent,
fontFace: "Calibri", charSpacing: 2
});
s.addText("Vascular Supply · Perfusion Physics · Flap Classification · Failure & Salvage", {
x: 0.6, y: 3.1, w: 5, h: 0.5,
fontSize: 13, color: C.grey, italic: true, fontFace: "Calibri"
});
// Source badge
card(s, 0.6, 4.3, 4.5, 0.7);
s.addText("Source: Cummings Otolaryngology Head & Neck Surgery · Chapter 77", {
x: 0.6, y: 4.3, w: 4.5, h: 0.7,
fontSize: 10, color: C.lightblue, align: "center", valign: "middle"
});
// Right panel decorative lines
for (let i = 0; i < 6; i++) {
s.addShape(pres.shapes.RECTANGLE, {
x: 5.8, y: 0.6 + i * 0.72, w: 3.8, h: 0.04,
fill: { color: i === 0 ? C.accent : "1E3A50" },
line: { color: i === 0 ? C.accent : "1E3A50" }
});
}
s.addText("OTOLARYNGOLOGY\nHEAD & NECK SURGERY", {
x: 5.5, y: 1.5, w: 4.2, h: 1.2,
fontSize: 22, bold: true, color: "1E3A50",
align: "center", valign: "middle"
});
s.addText("SKIN FLAP\nPHYSIOLOGY", {
x: 5.5, y: 2.7, w: 4.2, h: 1.4,
fontSize: 36, bold: true, color: C.teal,
align: "center", valign: "middle", charSpacing: 3
});
}
// ─── SLIDE 2: OVERVIEW / AGENDA ──────────────────────────────────────────
{
let s = pres.addSlide();
addBg(s);
addTopBar(s, C.teal);
pill(s, "OVERVIEW", 0.4, 0.18, 1.8, C.teal);
s.addText("What We Will Cover", {
x: 0.4, y: 0.6, w: 9, h: 0.65,
fontSize: 30, bold: true, color: C.white, fontFace: "Calibri"
});
const topics = [
{ n: "01", title: "Physics of Flow", sub: "Hagen-Poiseuille · Perfusion Pressure · Resistance", col: C.accent },
{ n: "02", title: "Critical Closing Pressure", sub: "LaPlace's Law · Flap Length vs. Viability", col: C.gold },
{ n: "03", title: "Zones of Perfusion", sub: "Macrocirculation · Microcirculation · Interstitium", col: C.teal },
{ n: "04", title: "Flap Classification", sub: "Random · Axial · Fasciocutaneous · Myocutaneous", col: C.lightblue },
{ n: "05", title: "Flap Failure & Salvage", sub: "Risk Factors · Monitoring · HBO · Delay", col: C.accent },
];
topics.forEach((t, i) => {
const x = 0.3 + (i % 3) * 3.2;
const y = i < 3 ? 1.5 : 3.2;
const w = 2.9;
card(s, x, y, w, 1.4);
// number
s.addText(t.n, {
x: x + 0.15, y: y + 0.1, w: 0.5, h: 0.5,
fontSize: 22, bold: true, color: t.col, margin: 0
});
s.addText(t.title, {
x: x + 0.15, y: y + 0.55, w: w - 0.3, h: 0.4,
fontSize: 13, bold: true, color: C.white, margin: 0
});
s.addText(t.sub, {
x: x + 0.15, y: y + 0.95, w: w - 0.3, h: 0.38,
fontSize: 9, color: C.grey, margin: 0
});
});
}
// ─── SLIDE 3: PHYSICS OF FLOW ─────────────────────────────────────────────
{
let s = pres.addSlide();
addBg(s);
addTopBar(s, C.accent);
pill(s, "PHYSICS OF FLOW", 0.4, 0.18, 2.2, C.accent);
s.addText("Hagen-Poiseuille Equation", {
x: 0.4, y: 0.6, w: 9, h: 0.65,
fontSize: 28, bold: true, color: C.white
});
// Formula box
card(s, 0.4, 1.35, 9.2, 1.05, "0A1520");
s.addShape(pres.shapes.RECTANGLE, {
x: 0.4, y: 1.35, w: 0.06, h: 1.05,
fill: { color: C.accent }, line: { color: C.accent }
});
s.addText("Q = π r⁴ · ΔP / 8ηl", {
x: 0.8, y: 1.35, w: 4, h: 1.05,
fontSize: 30, bold: true, color: C.gold, align: "left", valign: "middle"
});
s.addText([
{ text: "Q", options: { bold: true, color: C.gold } },
{ text: " = Flow ", options: { color: C.offwhite } },
{ text: "r⁴", options: { bold: true, color: C.gold } },
{ text: " = Vessel radius (4th power)\n", options: { color: C.offwhite } },
{ text: "ΔP", options: { bold: true, color: C.gold } },
{ text: " = Perfusion pressure ", options: { color: C.offwhite } },
{ text: "η", options: { bold: true, color: C.gold } },
{ text: " = Viscosity ", options: { color: C.offwhite } },
{ text: "l", options: { bold: true, color: C.gold } },
{ text: " = Length", options: { color: C.offwhite } },
], { x: 4.5, y: 1.35, w: 5, h: 1.05, fontSize: 11, valign: "middle" });
// Perfusion pressure box
card(s, 0.4, 2.55, 4.3, 0.75, "0A1520");
s.addText("Perfusion Pressure = P_diastolic − P_tissue", {
x: 0.4, y: 2.55, w: 4.3, h: 0.75,
fontSize: 13, bold: true, color: C.teal, align: "center", valign: "middle"
});
// Clinical goals
const goals = [
{ icon: "↑", label: "Maintain systemic BP", detail: "Avoid hypotension & vasoconstriction" },
{ icon: "↓", label: "Minimize tissue pressure", detail: "No excess tension, edema or fluid overload" },
{ icon: "⊕", label: "Maximize vessel radius", detail: "Base on named vessels; use delay or free transfer" },
{ icon: "↓", label: "Lower blood viscosity", detail: "Hydration · Low-normal hematocrit" },
{ icon: "↓", label: "Minimize flap length", detail: "Longer flap = more resistance = distal risk" },
];
goals.forEach((g, i) => {
const x = 0.35 + (i % 3) * 3.1;
const y = i < 3 ? 3.42 : 4.52;
const yw = i >= 3 ? 3.4 : 3.1;
card(s, x, y, i >= 3 ? yw - 0.1 : 2.9, 0.85);
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: x + 0.1, y: y + 0.17, w: 0.38, h: 0.38,
fill: { color: C.accent }, line: { color: C.accent }, rectRadius: 0.05
});
s.addText(g.icon, {
x: x + 0.1, y: y + 0.17, w: 0.38, h: 0.38,
fontSize: 16, bold: true, color: C.white, align: "center", valign: "middle", margin: 0
});
s.addText(g.label, {
x: x + 0.55, y: y + 0.08, w: (i >= 3 ? yw - 0.1 : 2.9) - 0.65, h: 0.35,
fontSize: 11, bold: true, color: C.white, margin: 0
});
s.addText(g.detail, {
x: x + 0.55, y: y + 0.44, w: (i >= 3 ? yw - 0.1 : 2.9) - 0.65, h: 0.3,
fontSize: 9, color: C.grey, margin: 0
});
});
}
// ─── SLIDE 4: CRITICAL CLOSING PRESSURE ──────────────────────────────────
{
let s = pres.addSlide();
addBg(s);
addTopBar(s, C.gold);
pill(s, "CRITICAL CLOSING PRESSURE", 0.4, 0.18, 3.2, C.gold);
s.addText("Flap Length vs. Perfusion Pressure", {
x: 0.4, y: 0.6, w: 9, h: 0.65,
fontSize: 28, bold: true, color: C.white
});
// Chart image (left)
if (imgFlap) {
s.addImage({ data: imgFlap, x: 0.3, y: 1.35, w: 5.2, h: 3.6 });
}
// Concepts (right column)
const concepts = [
{
title: "LaPlace's Law",
body: "Surface tension on vessel walls ↑ with radius → explains vessel dilation and development of collateral flow (basis for flap delay)"
},
{
title: "Critical Closing Pressure",
body: "When tissue pressure exceeds intracapillary pressure → capillary collapse → flow ceases. This threshold defines the necrotic zone."
},
{
title: "Width ≠ Safety",
body: "Wider random flap base adds vessels with the SAME perfusion pressure — does NOT change survival length. PP:CCP ratio is unchanged."
},
];
concepts.forEach((c, i) => {
card(s, 5.7, 1.35 + i * 1.3, 4.05, 1.15);
s.addShape(pres.shapes.RECTANGLE, {
x: 5.7, y: 1.35 + i * 1.3, w: 0.06, h: 1.15,
fill: { color: C.gold }, line: { color: C.gold }
});
s.addText(c.title, {
x: 5.85, y: 1.4 + i * 1.3, w: 3.8, h: 0.35,
fontSize: 13, bold: true, color: C.gold, margin: 0
});
s.addText(c.body, {
x: 5.85, y: 1.75 + i * 1.3, w: 3.8, h: 0.65,
fontSize: 10, color: C.offwhite, margin: 0
});
});
s.addText("Fig. 77.1 — Viable, At-Risk, and Necrotic zones along flap length", {
x: 0.3, y: 4.95, w: 5.2, h: 0.3,
fontSize: 8, italic: true, color: C.grey, align: "center"
});
}
// ─── SLIDE 5: ZONES OF PERFUSION ─────────────────────────────────────────
{
let s = pres.addSlide();
addBg(s);
addTopBar(s, C.teal);
pill(s, "ZONES OF PERFUSION", 0.4, 0.18, 2.4, C.teal);
s.addText("Three-Zone Model of Flap Vascularity", {
x: 0.4, y: 0.6, w: 9, h: 0.65,
fontSize: 28, bold: true, color: C.white
});
const zones = [
{
num: "I",
label: "Macrocirculatory",
color: C.accent,
items: [
"Large vessels, pedicle, anastomosis",
"Governed by systemic BP & vessel patency",
"Monitor: Doppler, near-infrared spectroscopy, temperature",
"Salvage: Explore pedicle / re-anastomose / thrombectomy",
]
},
{
num: "II",
label: "Microcirculatory",
color: C.gold,
items: [
"Arterioles → metarterioles → precapillary sphincters",
"A-V shunts bypass nutritive capillary flow",
"Precapillary sphincters regulate nutritive blood flow",
"Monitor: tissue oxygenation, tissue pressure",
"Salvage: vascular washout, reduce edema",
]
},
{
num: "III",
label: "Interstitial",
color: C.teal,
items: [
"Proteoglycans, collagen, hyaluronic acid matrix",
"Starling forces govern transcapillary flow",
"Diffusion (small molecules) & convection (bulk flow)",
"Edema ↑ diffusion distances → ↓ nutrient delivery",
"Salvage: optimize Starling forces, reduce edema",
]
},
];
zones.forEach((z, i) => {
const x = 0.22 + i * 3.25;
card(s, x, 1.38, 3.1, 3.95);
// header
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x, y: 1.38, w: 3.1, h: 0.62,
fill: { color: z.color }, line: { color: z.color }, rectRadius: 0.1
});
s.addText(`Zone ${z.num}`, {
x: x + 0.12, y: 1.38, w: 0.65, h: 0.62,
fontSize: 22, bold: true, color: C.bg, valign: "middle", margin: 0
});
s.addText(z.label, {
x: x + 0.75, y: 1.38, w: 2.25, h: 0.62,
fontSize: 12, bold: true, color: C.bg, valign: "middle", margin: 0
});
// bullets
z.items.forEach((item, j) => {
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: x + 0.18, y: 2.12 + j * 0.56, w: 0.22, h: 0.22,
fill: { color: z.color }, line: { color: z.color }, rectRadius: 0.04
});
s.addText(item, {
x: x + 0.48, y: 2.08 + j * 0.56, w: 2.5, h: 0.48,
fontSize: 9.5, color: C.offwhite, valign: "top", margin: 0
});
});
});
}
// ─── SLIDE 6: STARLING EQUATION ──────────────────────────────────────────
{
let s = pres.addSlide();
addBg(s);
addTopBar(s, C.teal);
pill(s, "ZONE III — INTERSTITIUM", 0.4, 0.18, 2.6, C.teal);
s.addText("Starling Forces & Capillary Exchange", {
x: 0.4, y: 0.6, w: 9, h: 0.65,
fontSize: 28, bold: true, color: C.white
});
// Starling equation box
card(s, 0.4, 1.38, 9.2, 1.0, "0A1520");
s.addShape(pres.shapes.RECTANGLE, {
x: 0.4, y: 1.38, w: 0.06, h: 1.0,
fill: { color: C.teal }, line: { color: C.teal }
});
s.addText("Jv/A = Lp [ (Pc − Pi) − σ(πc − πi) ]", {
x: 0.7, y: 1.38, w: 9, h: 1.0,
fontSize: 22, bold: true, color: C.teal, valign: "middle"
});
// Legend table
const terms = [
{ sym: "Jv/A", def: "Plasma flow out of capillary per unit area" },
{ sym: "Lp", def: "Membrane water permeability" },
{ sym: "Pc − Pi", def: "Hydrostatic pressure gradient (capillary − interstitium)" },
{ sym: "πc − πi", def: "Osmotic pressure gradient (capillary − interstitium)" },
{ sym: "σ", def: "Osmotic reflection coefficient (membrane 'leakiness')" },
];
terms.forEach((t, i) => {
const x = i < 3 ? 0.4 : 5.1;
const y = i < 3 ? 2.55 + i * 0.62 : 2.55 + (i - 3) * 0.62;
const w = 4.4;
card(s, x, y, w, 0.52);
s.addText(t.sym, {
x: x + 0.15, y, w: 0.9, h: 0.52,
fontSize: 14, bold: true, color: C.gold, valign: "middle", margin: 0
});
s.addText(t.def, {
x: x + 1.05, y, w: w - 1.2, h: 0.52,
fontSize: 10, color: C.offwhite, valign: "middle", margin: 0
});
});
// Two mechanisms
const mechs = [
{ t: "Diffusion", d: "Dominant for SMALL molecules under normal conditions. Edema ↑ diffusion distances → ↓ nutrient delivery to cells." },
{ t: "Convective Flow", d: "Bulk flow sweeps molecules along microchannels regardless of concentration gradient. Important for LARGE molecules." },
];
mechs.forEach((m, i) => {
card(s, 0.4 + i * 4.8, 4.55, 4.6, 0.82);
s.addShape(pres.shapes.RECTANGLE, {
x: 0.4 + i * 4.8, y: 4.55, w: 0.06, h: 0.82,
fill: { color: i === 0 ? C.accent : C.gold },
line: { color: i === 0 ? C.accent : C.gold }
});
s.addText(m.t, {
x: 0.6 + i * 4.8, y: 4.58, w: 4.2, h: 0.3,
fontSize: 13, bold: true, color: i === 0 ? C.accent : C.gold, margin: 0
});
s.addText(m.d, {
x: 0.6 + i * 4.8, y: 4.88, w: 4.2, h: 0.44,
fontSize: 9.5, color: C.offwhite, margin: 0
});
});
}
// ─── SLIDE 7: FLAP CLASSIFICATION ────────────────────────────────────────
{
let s = pres.addSlide();
addBg(s);
addTopBar(s, C.lightblue);
pill(s, "FLAP CLASSIFICATION", 0.4, 0.18, 2.4, "2A7D8A");
s.addText("Classification by Vascular Supply", {
x: 0.4, y: 0.6, w: 9, h: 0.65,
fontSize: 28, bold: true, color: C.white
});
// Image right
if (imgClass) {
s.addImage({ data: imgClass, x: 5.2, y: 1.3, w: 4.5, h: 3.8 });
}
const flaps = [
{
type: "Random Cutaneous",
supply: "Subdermal plexus from unnamed musculocutaneous perforators",
plane: "Subcutaneous fat",
note: "Survival = perfusion pressure, NOT length:width ratio",
col: C.accent
},
{
type: "Arterial (Axial)",
supply: "Named septocutaneous artery along flap axis",
plane: "Must include septocutaneous vessel",
note: "Distal extension beyond named artery = random territory",
col: C.gold
},
{
type: "Fasciocutaneous",
supply: "Septocutaneous vessels → deep fascial plexus → subdermal plexus",
plane: "Deep fascia included",
note: "4 subtypes; relies on skin vascular territories",
col: C.teal
},
{
type: "Musculocutaneous",
supply: "Segmental vessels to muscle → musculocutaneous perforators",
plane: "Muscle incorporated",
note: "Best survival; leaves local perforators intact",
col: C.lightblue
},
];
flaps.forEach((f, i) => {
card(s, 0.25, 1.3 + i * 1.0, 4.75, 0.88);
s.addShape(pres.shapes.RECTANGLE, {
x: 0.25, y: 1.3 + i * 1.0, w: 0.06, h: 0.88,
fill: { color: f.col }, line: { color: f.col }
});
s.addText(f.type, {
x: 0.4, y: 1.33 + i * 1.0, w: 4.4, h: 0.28,
fontSize: 12, bold: true, color: f.col, margin: 0
});
s.addText(`Supply: ${f.supply}`, {
x: 0.4, y: 1.6 + i * 1.0, w: 4.4, h: 0.24,
fontSize: 8.5, color: C.offwhite, margin: 0
});
s.addText(`▶ ${f.note}`, {
x: 0.4, y: 1.84 + i * 1.0, w: 4.4, h: 0.24,
fontSize: 8.5, color: C.grey, italic: true, margin: 0
});
});
s.addText("Fig. 77.5 — Vascular supply patterns for each flap type", {
x: 5.2, y: 5.12, w: 4.5, h: 0.25,
fontSize: 8, italic: true, color: C.grey, align: "center"
});
}
// ─── SLIDE 8: HEAD & NECK EXAMPLES ───────────────────────────────────────
{
let s = pres.addSlide();
addBg(s);
addTopBar(s, C.gold);
pill(s, "H&N EXAMPLES", 0.4, 0.18, 1.8, C.gold);
s.addText("Common Head & Neck Flaps", {
x: 0.4, y: 0.6, w: 9, h: 0.65,
fontSize: 28, bold: true, color: C.white
});
const examples = [
{ flap: "Deltopectoral Flap", type: "Arterial (Axial)", vessel: "Anterior perforators of internal mammary artery", col: C.gold },
{ flap: "Paramedian Forehead Flap", type: "Arterial (Axial)", vessel: "Supratrochlear vessels", col: C.gold },
{ flap: "Pectoralis Major Myocutaneous", type: "Musculocutaneous", vessel: "Pectoral branch of thoracoacromial artery", col: C.lightblue },
{ flap: "Latissimus Dorsi Flap", type: "Musculocutaneous", vessel: "Thoracodorsal artery (segmental supply)", col: C.lightblue },
{ flap: "Radial Forearm Free Flap", type: "Free Tissue Transfer", vessel: "Radial artery", col: C.teal },
{ flap: "Fibula Free Flap", type: "Osteocutaneous Free Flap", vessel: "Peroneal artery", col: C.teal },
];
examples.forEach((e, i) => {
const col = i % 2 === 0 ? 0.3 : 5.1;
const row = Math.floor(i / 2);
card(s, col, 1.5 + row * 1.25, 4.55, 1.1);
s.addShape(pres.shapes.RECTANGLE, {
x: col, y: 1.5 + row * 1.25, w: 0.06, h: 1.1,
fill: { color: e.col }, line: { color: e.col }
});
s.addText(e.flap, {
x: col + 0.18, y: 1.54 + row * 1.25, w: 4.2, h: 0.32,
fontSize: 13, bold: true, color: C.white, margin: 0
});
s.addText(e.type, {
x: col + 0.18, y: 1.85 + row * 1.25, w: 4.2, h: 0.25,
fontSize: 10, color: e.col, italic: true, margin: 0
});
s.addText(`Vessel: ${e.vessel}`, {
x: col + 0.18, y: 2.1 + row * 1.25, w: 4.2, h: 0.38,
fontSize: 9.5, color: C.grey, margin: 0
});
});
}
// ─── SLIDE 9: FLAP FAILURE & MONITORING ──────────────────────────────────
{
let s = pres.addSlide();
addBg(s);
addTopBar(s, C.accent);
pill(s, "FLAP FAILURE & MONITORING", 0.4, 0.18, 2.8, C.accent);
s.addText("Recognition, Monitoring & Salvage", {
x: 0.4, y: 0.6, w: 9, h: 0.65,
fontSize: 28, bold: true, color: C.white
});
// Risk factors
card(s, 0.3, 1.35, 9.4, 0.72);
s.addText("⚠ Key Risk Factors:", {
x: 0.5, y: 1.38, w: 2, h: 0.35,
fontSize: 11, bold: true, color: C.accent, margin: 0
});
s.addText("Diabetes · Prior irradiation · Hypotension · Excess tension on closure · Tissue edema · High hematocrit · Vasoconstriction", {
x: 2.4, y: 1.38, w: 7.1, h: 0.6,
fontSize: 10, color: C.offwhite, valign: "middle", margin: 0
});
// Monitoring / salvage table
const rows = [
{ zone: "Zone I\n(Macro)", monitor: "Doppler · Near-infrared spectroscopy · Temperature", salvage: "Explore pedicle / anastomosis · Thrombectomy", col: C.accent },
{ zone: "Zone II\n(Micro)", monitor: "Doppler · Tissue oxygenation · Tissue pressure", salvage: "Vascular washout · Reduce edema", col: C.gold },
{ zone: "Zone III\n(Interstitium)", monitor: "Clinical assessment · Fluid balance", salvage: "Optimize Starling forces · Manage edema", col: C.teal },
];
// Table header
["Zone", "Monitoring Method", "Salvage Method"].forEach((h, i) => {
const xs = [0.3, 2.0, 6.0];
const ws = [1.55, 3.8, 3.75];
s.addShape(pres.shapes.RECTANGLE, {
x: xs[i], y: 2.18, w: ws[i], h: 0.4,
fill: { color: "1E3A50" }, line: { color: "1E3A50" }
});
s.addText(h, {
x: xs[i] + 0.1, y: 2.18, w: ws[i] - 0.1, h: 0.4,
fontSize: 11, bold: true, color: C.offwhite, valign: "middle", margin: 0
});
});
rows.forEach((r, i) => {
const y = 2.65 + i * 0.88;
card(s, 0.3, y, 1.55, 0.82, "0A1520");
s.addShape(pres.shapes.RECTANGLE, {
x: 0.3, y, w: 0.06, h: 0.82,
fill: { color: r.col }, line: { color: r.col }
});
s.addText(r.zone, {
x: 0.42, y: y + 0.04, w: 1.35, h: 0.74,
fontSize: 10, bold: true, color: r.col, valign: "middle", margin: 0
});
card(s, 2.0, y, 3.8, 0.82);
s.addText(r.monitor, {
x: 2.15, y: y + 0.08, w: 3.5, h: 0.66,
fontSize: 10, color: C.offwhite, valign: "middle", margin: 0
});
card(s, 6.0, y, 3.75, 0.82);
s.addText(r.salvage, {
x: 6.15, y: y + 0.08, w: 3.45, h: 0.66,
fontSize: 10, color: C.offwhite, valign: "middle", margin: 0
});
});
}
// ─── SLIDE 10: AUGMENTING FLAP SURVIVAL ──────────────────────────────────
{
let s = pres.addSlide();
addBg(s);
addTopBar(s, C.teal);
pill(s, "AUGMENTING SURVIVAL", 0.4, 0.18, 2.4, C.teal);
s.addText("Flap Delay & Hyperbaric Oxygen", {
x: 0.4, y: 0.6, w: 9, h: 0.65,
fontSize: 28, bold: true, color: C.white
});
// Flap Delay card
card(s, 0.3, 1.38, 4.6, 3.9);
s.addShape(pres.shapes.RECTANGLE, {
x: 0.3, y: 1.38, w: 4.6, h: 0.5,
fill: { color: C.teal }, line: { color: C.teal }
});
s.addText("FLAP DELAY", {
x: 0.3, y: 1.38, w: 4.6, h: 0.5,
fontSize: 15, bold: true, color: C.bg, align: "center", valign: "middle", margin: 0
});
const delayPts = [
"Preliminary interruption of part of flap's blood supply",
"Triggers collateral vessel dilation via LaPlace's Law",
"Allows time for neovascularization",
"Effectively extends safe flap length",
"Used when large or borderline flap is planned",
"Interval of 1–3 weeks typically required",
];
delayPts.forEach((p, i) => {
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 0.52, y: 2.02 + i * 0.52, w: 0.22, h: 0.22,
fill: { color: C.teal }, line: { color: C.teal }, rectRadius: 0.04
});
s.addText(p, {
x: 0.82, y: 1.98 + i * 0.52, w: 3.9, h: 0.44,
fontSize: 10, color: C.offwhite, margin: 0, valign: "middle"
});
});
// HBO card
card(s, 5.1, 1.38, 4.6, 3.9);
s.addShape(pres.shapes.RECTANGLE, {
x: 5.1, y: 1.38, w: 4.6, h: 0.5,
fill: { color: C.gold }, line: { color: C.gold }
});
s.addText("HYPERBARIC OXYGEN (HBO)", {
x: 5.1, y: 1.38, w: 4.6, h: 0.5,
fontSize: 15, bold: true, color: C.bg, align: "center", valign: "middle", margin: 0
});
const hboPts = [
"↑ O₂ carrying capacity by ~20% (plasma-dissolved O₂)",
"Greater effect with low hematocrit",
"↑ O₂ diffusion from perfused → ischemic zone",
"↓ Leukocyte adherence · ↓ Edema · ↑ Neovascularization",
"Must be given EARLY — little benefit after 24h",
"Challenge test: TcO₂ rise ≥50 mmHg = favorable",
"Reserve for high-risk flaps (not cost-effective for all)",
];
hboPts.forEach((p, i) => {
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 5.32, y: 2.02 + i * 0.44, w: 0.22, h: 0.22,
fill: { color: C.gold }, line: { color: C.gold }, rectRadius: 0.04
});
s.addText(p, {
x: 5.62, y: 1.98 + i * 0.44, w: 3.9, h: 0.38,
fontSize: 9.5, color: C.offwhite, margin: 0, valign: "middle"
});
});
}
// ─── SLIDE 11: SUMMARY ───────────────────────────────────────────────────
{
let s = pres.addSlide();
addBg(s);
addTopBar(s, C.accent);
// Background accent block
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 0.18, h: 5.625,
fill: { color: C.accent }, line: { color: C.accent }
});
s.addText("Key Takeaways", {
x: 0.5, y: 0.25, w: 9, h: 0.65,
fontSize: 30, bold: true, color: C.white
});
const takeaways = [
{ n: "1", text: "Vascular supply is THE most critical factor in flap planning — perfusion pressure (DBP − tissue pressure) drives all zones.", col: C.accent },
{ n: "2", text: "Hagen-Poiseuille: vessel radius (r⁴) dominates flow. Choose large named vessels, minimize length, and maintain BP.", col: C.gold },
{ n: "3", text: "Critical closing pressure determines viable vs. at-risk vs. necrotic zones. Wider base does NOT increase survival length.", col: C.teal },
{ n: "4", text: "Three zones of perfusion (macro → micro → interstitial) each have distinct monitoring and salvage strategies.", col: C.lightblue },
{ n: "5", text: "Flap type dictates vascular anatomy: Random < Axial < Fasciocutaneous < Musculocutaneous in terms of reliability.", col: C.gold },
{ n: "6", text: "Flap delay (collateral development) and HBO (early, high-risk cases only) are the main methods to augment survival.", col: C.accent },
];
takeaways.forEach((t, i) => {
const y = 1.05 + i * 0.72;
card(s, 0.5, y, 9.2, 0.62);
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 0.62, y: y + 0.1, w: 0.38, h: 0.38,
fill: { color: t.col }, line: { color: t.col }, rectRadius: 0.06
});
s.addText(t.n, {
x: 0.62, y: y + 0.1, w: 0.38, h: 0.38,
fontSize: 14, bold: true, color: C.bg, align: "center", valign: "middle", margin: 0
});
s.addText(t.text, {
x: 1.12, y: y + 0.06, w: 8.4, h: 0.5,
fontSize: 10.5, color: C.offwhite, valign: "middle", margin: 0
});
});
s.addText("Cummings Otolaryngology Head & Neck Surgery · Chapter 77: Skin Flap Physiology", {
x: 0.5, y: 5.3, w: 9.2, h: 0.25,
fontSize: 8.5, italic: true, color: C.grey, align: "center"
});
}
// ─── WRITE FILE ───────────────────────────────────────────────────────────
pres.writeFile({ fileName: "/home/daytona/workspace/skin-flap-ppt/Skin_Flap_Physiology.pptx" })
.then(() => console.log("✅ Done: /home/daytona/workspace/skin-flap-ppt/Skin_Flap_Physiology.pptx"))
.catch(e => { console.error("❌ Error:", e); process.exit(1); });
Running Command
cd /home/daytona/workspace/skin-flap-ppt && node generate.js 2>&1
Your presentation is ready:
Skin Flap Physiology
Presentation · PPTX
11 slides with a deep navy + surgical red palette:
| Slide | Content |
|---|---|
| 1 | Title |
| 2 | Overview / Agenda |
| 3 | Physics of Flow — Hagen-Poiseuille, clinical goals |
| 4 | Critical Closing Pressure — flap length graph (Fig. 77.1) |
| 5 | Three Zones of Perfusion (macro/micro/interstitial) |
| 6 | Starling Forces & Capillary Exchange (Zone III) |
| 7 | Flap Classification — with the 4-type vascular diagram (Fig. 77.5) |
| 8 | H&N Flap Examples (deltopectoral, forehead, pec major, LD, radial forearm, fibula) |
| 9 | Flap Failure — risk factors, monitoring & salvage table by zone |
| 10 | Augmenting Survival — Flap Delay vs. HBO side-by-side |
| 11 | Key Takeaways + source citation |
This is a shared conversation. Sign in to Orris to start your own chat.