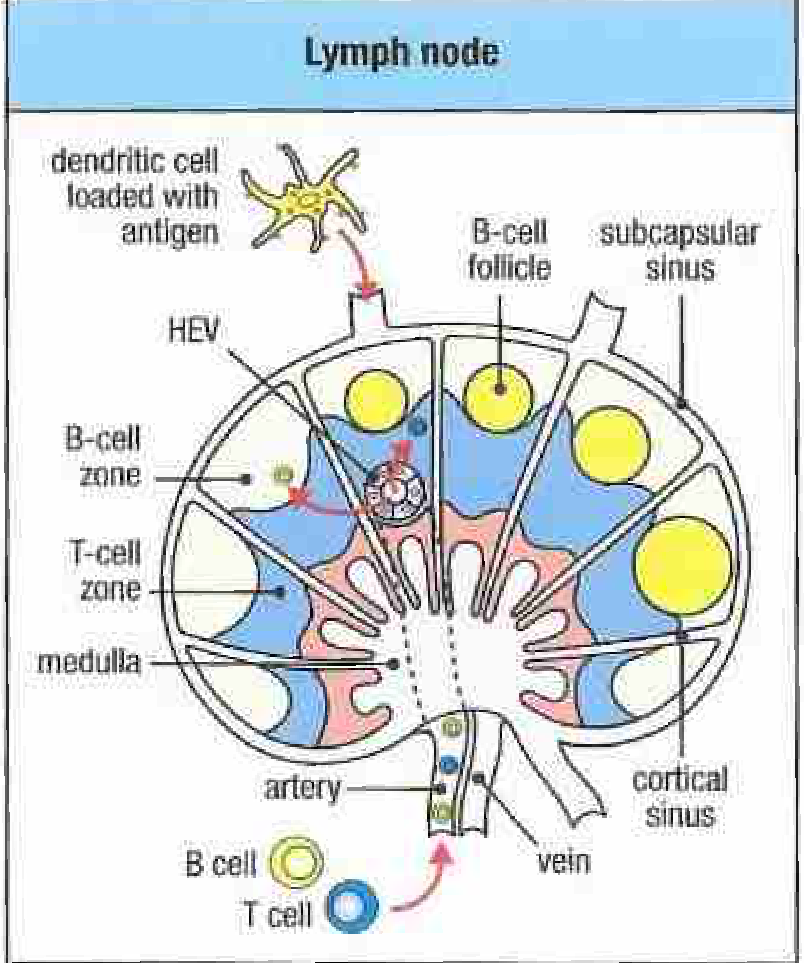
Lymph node
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple textbooks. Here is a thorough overview of the lymph node:
Lymph Node
A lymph node is a small, bean-shaped, encapsulated secondary lymphoid organ positioned at intervals along lymphatic vessels throughout the body. Hundreds are found in the body, concentrated in regions like the neck, axilla, groin, mediastinum, and abdomen. They serve as filtration checkpoints for lymph and as specialized sites where adaptive immune responses are initiated.
Gross Anatomy
- Shape and size: Bean-shaped, typically 1-25 mm in diameter.
- Afferent lymphatics: Multiple vessels enter at the convex surface, delivering lymph into the node.
- Hilum: A concave depression on one side where a single efferent lymphatic vessel exits, carrying filtered lymph onward. The artery, vein, and nerves also enter/exit here.
- Capsule: A dense connective tissue capsule surrounds the node and sends trabeculae inward, providing structural scaffolding through which blood vessels branch.
- Valves: Present in lymphatic vessels, ensuring one-way lymph flow.
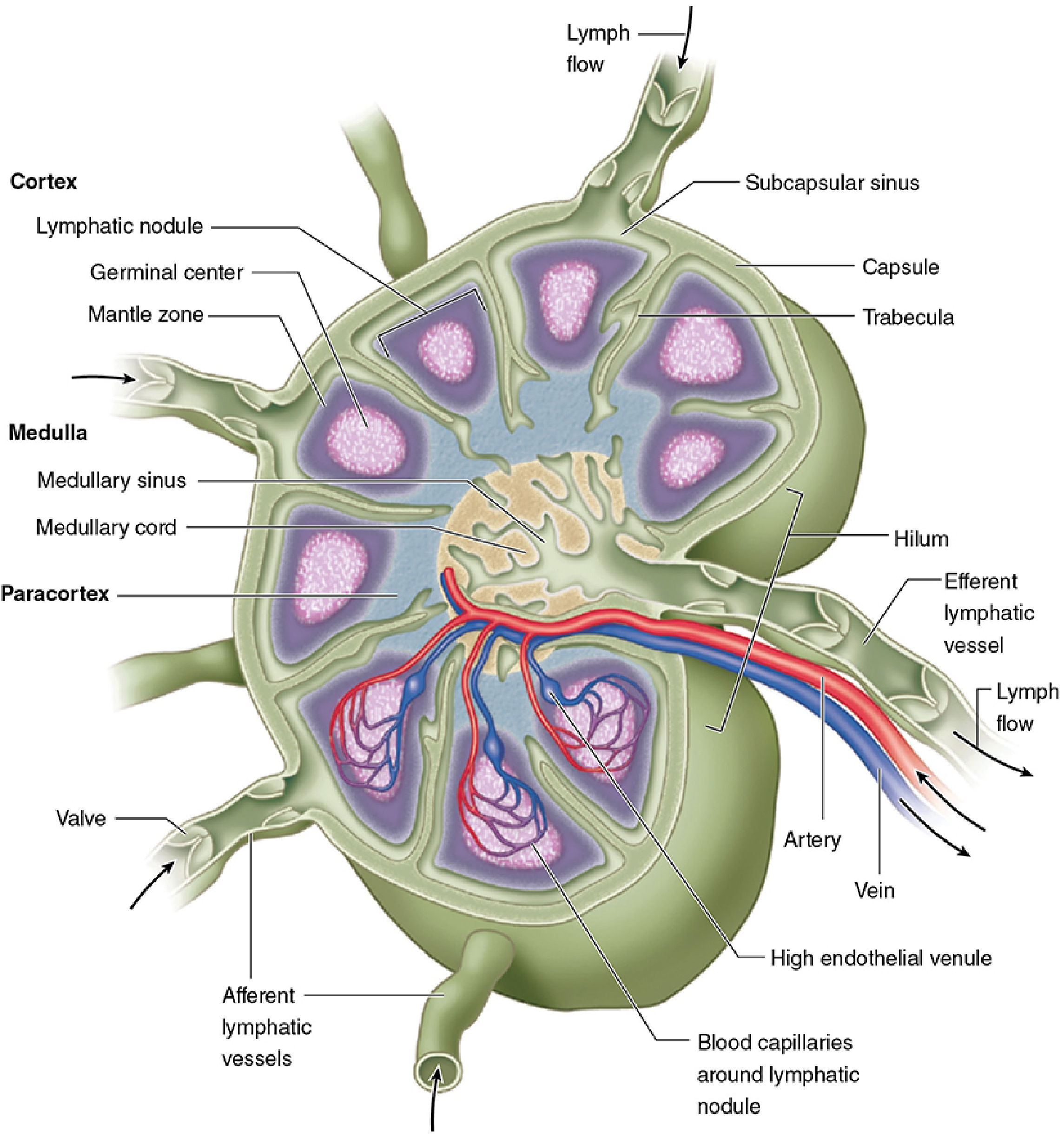
Internal Structure: Three Functional Regions
The lymph node is organized into three regions that are functionally distinct but not physically separated by epithelium (unlike the thymus):
1. Cortex (Outer Region - B-cell Zone)
- Receives lymph from the afferent lymphatics via the subcapsular sinus, a space immediately inside the capsule.
- From the subcapsular sinus, cortical (trabecular) sinuses branch inward, lined by a thin, discontinuous endothelium penetrated by reticulin fibers and dendritic cell processes. Antigen, lymphocytes, and APCs percolate easily into surrounding tissue.
- Contains lymphoid nodules (follicles), which are primarily composed of B lymphocytes:
- Primary follicles: Compact, resting B cells; no germinal center.
- Secondary follicles: Have a pale germinal center surrounded by a darker mantle zone. Germinal centers form after antigen stimulation and are sites of intense B-cell proliferation, somatic hypermutation, affinity maturation, and class switching. Macrophages here phagocytose apoptotic B cells that fail selection.
- Follicular dendritic cells (FDCs) are embedded in follicles and present antigen to B cells.
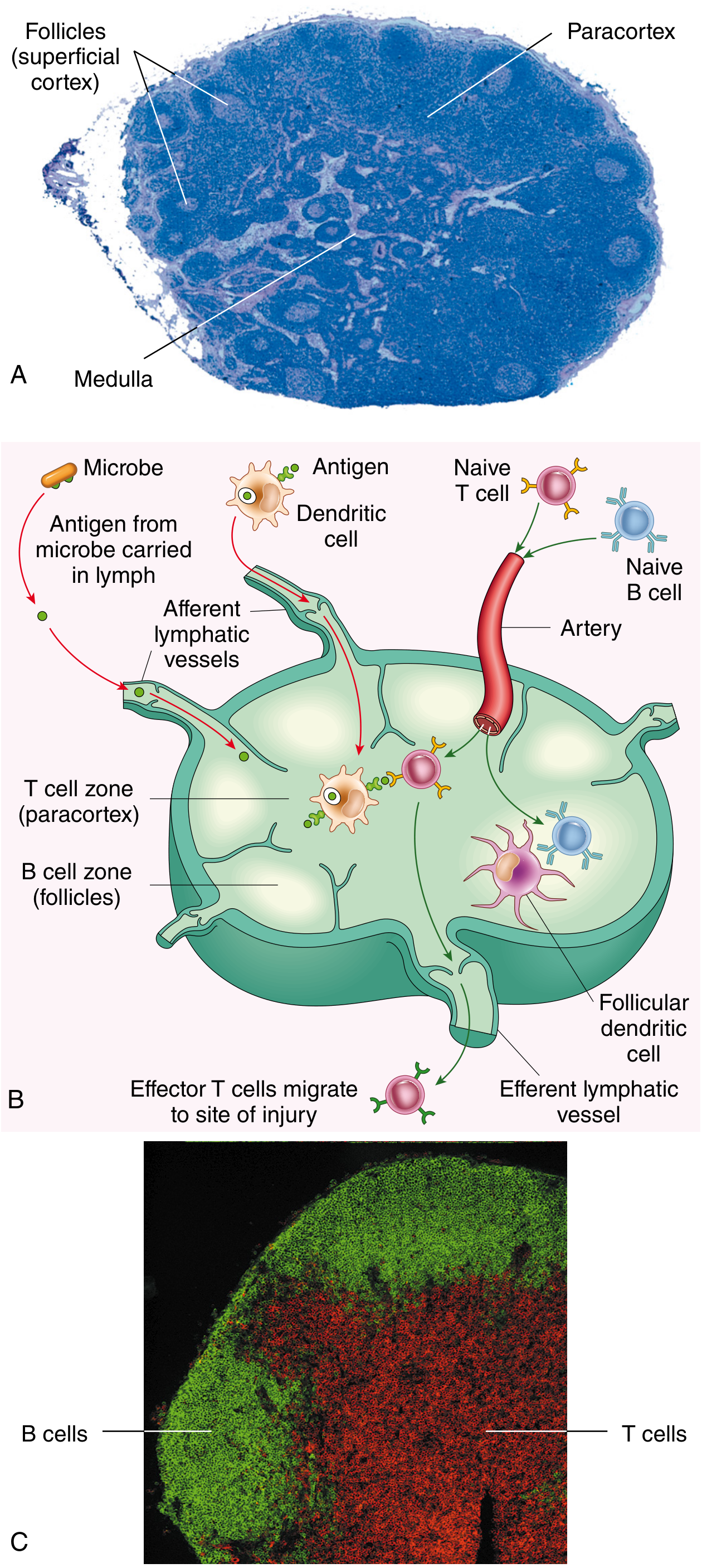
2. Paracortex (Deep Cortex - T-cell Zone)
- Lies between the cortex and medulla; lacks lymphoid nodules.
- Rich in T lymphocytes (distinguishable by immunohistochemistry).
- Contains dendritic cells that present processed peptide antigens to T cells, triggering T-cell activation.
- Houses high endothelial venules (HEVs): specialized postcapillary venules with unusually cuboidal endothelial cells that express surface glycoproteins. These are the main entry point for ~90% of circulating lymphocytes from blood into the lymph node. L-selectin on lymphocytes binds sugar-rich ligands on HEV endothelium; integrin-mediated adhesion follows, and lymphocytes undergo diapedesis into the paracortex.
- The paracortex expands dramatically (becomes very prominent) in T-cell-driven immune responses (e.g., viral infections).
3. Medulla (Inner Region)
- Two major components:
- Medullary cords: Branched masses of lymphoid tissue extending from the paracortex. Contain T cells, B cells, and many plasma cells (antibody-secreting).
- Medullary sinuses: Dilated spaces with discontinuous endothelium separating the cords. Contain a meshwork of reticular cell processes for final lymph filtration, plus macrophages and sometimes neutrophils (in infection). Sinuses converge at the hilum to form the efferent lymphatic.
Lymph Flow Through the Node
Afferent lymphatics → Subcapsular sinus → Cortical sinuses (along trabeculae) → Medullary sinuses → Efferent lymphatic at hilum
Lymph is slowed as it percolates through this reticular meshwork, giving macrophages, dendritic cells, and lymphocytes maximum opportunity to sample antigens.
Key Cells
| Cell Type | Location | Function |
|---|---|---|
| B lymphocytes | Cortex (follicles) | Antigen recognition, germinal center reactions, differentiation into plasma cells |
| T lymphocytes | Paracortex | Antigen recognition (via MHC-peptide), helper and cytotoxic effector functions |
| Plasma cells | Medullary cords | Antibody secretion |
| Follicular dendritic cells (FDCs) | Cortex (follicles) | Antigen presentation to B cells |
| Dendritic cells | Paracortex | Antigen presentation to T cells |
| Macrophages | Sinuses and medulla | Phagocytosis of particulate antigens, cellular debris, apoptotic cells |
| Reticular cells | Throughout | Structural framework (reticulin fibers) |
Functions
- Lymph filtration: Removes microbes, cellular debris, and foreign antigens from lymph before it returns to circulation.
- Immune surveillance: Concentrates rare antigen-specific T and B cells together with antigen-bearing dendritic cells, dramatically increasing the probability of a productive encounter despite the low frequency of any given naive clonal precursor (~1 in 10^6 T cells).
- Adaptive immune response initiation: Antigen-bearing dendritic cells arrive via afferent lymphatics; naive T cells arrive via HEVs. T-cell activation, clonal expansion, and differentiation into effector cells occur in the paracortex over several days.
- B-cell activation and antibody production: Germinal center reactions in follicles produce high-affinity, class-switched antibody-secreting plasma cells and long-lived memory B cells.
- Lymphocyte recirculation: Naive lymphocytes enter via HEVs, sample for antigen, then exit via efferent lymphatics if not activated (returning to blood); activated effector cells exit to reach sites of infection.
Clinical Relevance
- Lymphadenopathy (enlarged lymph nodes): Occurs with infection (reactive hyperplasia), malignancy (metastatic tumor cells seeding nodes), or primary lymphoid malignancies (lymphoma).
- Sentinel lymph node biopsy: The first draining lymph node from a tumor site; sampled to assess for metastatic spread (especially in breast cancer and melanoma).
- Germinal center expansion is seen in autoimmune conditions and certain infections.
- Paracortical expansion is characteristic of viral infections and T-cell lymphomas.
- Lymph node calcification can be a radiologic sign of prior infection (e.g., TB, histoplasmosis) or malignancy.
Sources: Junqueira's Basic Histology 17e, p. 704-711 | Robbins, Cotran & Kumar Pathologic Basis of Disease | Janeway's Immunobiology 10e, p. 368-369 | Cellular and Molecular Immunology
This is a shared conversation. Sign in to Orris to start your own chat.