Glucoma
Reading File
Finding Sources
Searching PubMed
glaucoma management treatment
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I have comprehensive content now. Let me compile a thorough, well-organized answer on glaucoma.
Glaucoma - Comprehensive Overview
Definition
Glaucoma is an optic neuropathy in which progressive damage to retinal ganglion cells and their axons results in characteristic loss of optic nerve tissue and visual field loss. The primary site of damage is at the lamina cribrosa, where optic nerve axons exit the eye. While elevated intraocular pressure (IOP) is the principal risk factor, some individuals develop glaucoma at normal IOP ("normal-tension glaucoma").
- Goldman-Cecil Medicine, p. 612
Aqueous Humor Dynamics (Pathophysiology)
The key to understanding glaucoma is aqueous humor flow:
- Aqueous is produced by the non-pigmented ciliary epithelium of the ciliary body (posterior chamber)
- It flows through the pupil into the anterior chamber
- It drains via the trabecular meshwork → Schlemm's canal → venous circulation (major pathway), plus the uveoscleral pathway (minor)
- If drainage fails to match production → IOP rises → retinal ganglion cell death → optic cup enlargement → visual field loss
Normal IOP: up to 21 mmHg (population mean + 2 SD). Above this = ocular hypertension, a major risk factor.
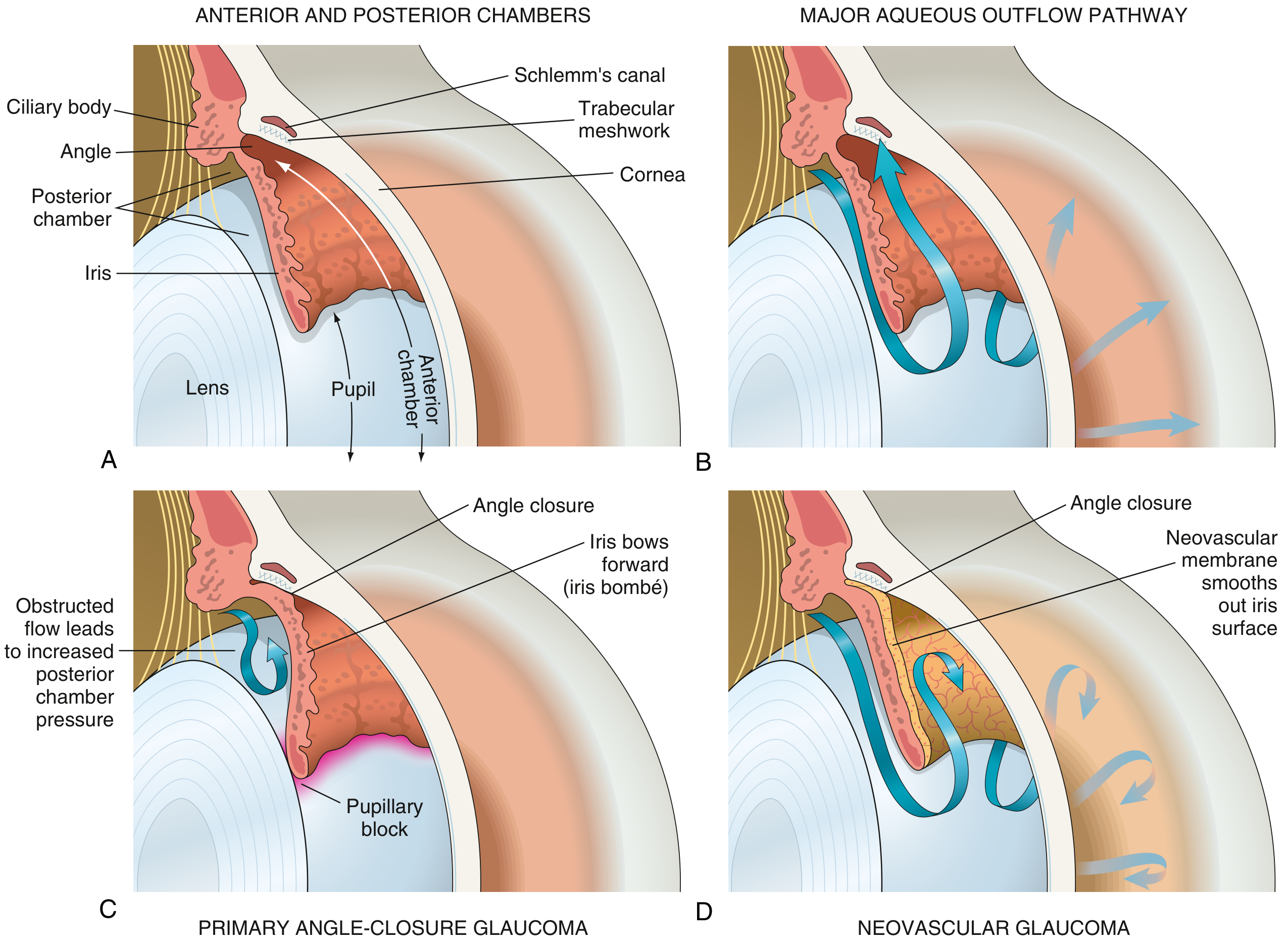
A: Normal eye anatomy. B: Normal aqueous outflow through trabecular meshwork. C: Primary angle-closure - iris bombé causing pupillary block. D: Neovascular glaucoma - fibrovascular membrane occluding angle. (Robbins & Kumar Basic Pathology)
Classification
1. Primary Open-Angle Glaucoma (POAG)
Most common type - especially in those of European and African ancestry.
- The anterior chamber angle is anatomically open, but outflow resistance is increased within the trabecular meshwork
- Chronic, insidious, asymptomatic until late stages
- Peripheral fields are lost first; central vision and acuity preserved until advanced disease
- Often detected during routine eye exam (high cup-to-disc ratio, elevated IOP)
Key features:
-
Retinal nerve fibre layer thinning
-
Optic nerve head cupping (elevated cup-to-disc ratio)
-
Characteristic arcuate visual field defects
-
Open anterior chamber angle on gonioscopy
-
IOP typically >21 mmHg (though normal in ~30% of cases)
-
Kanski's Clinical Ophthalmology 10e, p. 364
2. Primary Angle-Closure Glaucoma (PACG)
- Commonest in hyperopic (far-sighted), Asian, and older women
- The iris apposes the lens (pupillary block), blocking aqueous flow from posterior to anterior chamber
- Pressure builds in posterior chamber → iris bows forward (iris bombé) → angle physically closes
- Can be acute (ophthalmic emergency) or chronic/subacute
Acute angle-closure crisis:
- Sudden severe eye pain, blurred vision, halos around lights
- Red eye, corneal oedema, mid-dilated fixed pupil
- Headache, nausea, vomiting
- IOP may exceed 50-70 mmHg
3. Secondary Glaucomas
- Secondary open-angle: debris in angle (red cells from trauma, pigment, pseudoexfoliation material, necrotic tumour cells)
- Secondary angle-closure: neovascular glaucoma (fibrovascular membrane from ischaemia in diabetic retinopathy or CRVO), anterior synechiae from uveitis
- Congenital/developmental: trabeculodysgenesis; associations include Sturge-Weber syndrome (~30% develop glaucoma), aniridia, neurofibromatosis type 1
- Drug-induced: prolonged corticosteroid use (topical > systemic) → steroid-induced open-angle glaucoma
4. Normal-Tension Glaucoma (NTG)
- All features of POAG but IOP consistently ≤21 mmHg
- Suggests vascular insufficiency or increased optic nerve susceptibility is the primary driver
- More common in Japanese populations
Risk Factors for POAG
| Risk Factor | Details |
|---|---|
| Elevated IOP | Strongest modifiable factor; asymmetry ≥4 mmHg is significant |
| Age | Prevalence ~6% in White, ~16% in Black populations over age 70 |
| Race | 4× more common and earlier onset in Black patients |
| Family history | 4× risk in siblings, 2× in offspring of POAG patients |
| Myopia | Increased incidence; eyes may be more susceptible to damage |
| Low ocular perfusion pressure | Systemic hypotension, cardiovascular disease |
| Anti-VEGF therapy | Recurrent injections raise IOP, especially bevacizumab |
| Thin central corneal thickness | Underestimates true IOP on tonometry |
| Large optic disc area | More vulnerable to damage |
- Kanski's Clinical Ophthalmology 10e
Diagnosis
1. Tonometry
- Goldmann applanation tonometry = gold standard for IOP measurement
- Results affected by central corneal thickness (CCT) - thick corneas overestimate, thin corneas underestimate IOP
2. Gonioscopy
- Direct visualisation of the anterior chamber angle to distinguish open vs. closed angle
- Essential for classification
3. Optic Disc Evaluation
- Cup-to-disc (C:D) ratio: normal ≤0.5; suspicious >0.6; any asymmetry between eyes is significant
- Focal rim notching, disc haemorrhages, RNFL defects
4. Visual Field Testing (Perimetry)
- Automated static perimetry (Humphrey Field Analyzer) is standard
- 24-2 pattern - most commonly used for glaucoma (tests central 24° + 2°); detects defects within 30° of fixation
- 10-2 pattern - for advanced glaucoma threatening central vision
- Classic defects: arcuate scotomas, nasal steps, paracentral scotomas
5. OCT (Optical Coherence Tomography)
- Measures retinal nerve fibre layer (RNFL) thickness and optic disc parameters objectively
- Can detect structural damage before visual field loss is apparent
Treatment
Medical (First-line)
| Drug Class | Examples | Mechanism |
|---|---|---|
| Prostaglandin analogues | Latanoprost 0.005%, Travoprost 0.004% (once daily) | Increase uveoscleral outflow |
| Beta-blockers | Timolol 0.5% (twice daily) | Decrease aqueous production |
| Carbonic anhydrase inhibitors | Dorzolamide (3×/day topical), Acetazolamide (oral) | Decrease aqueous production |
| Alpha-2 agonists | Brimonidine (3×/day) | Decrease production, increase uveoscleral outflow |
| Rho-kinase inhibitors | Netarsudil 0.02% (once daily) | Increase trabecular outflow |
Generally required lifelong. Prostaglandin analogues are typically first-line due to efficacy and once-daily dosing.
Laser
- Laser trabeculoplasty (LTP/SLT): applies energy to trabecular meshwork, improves outflow. Can be considered first-line therapy - maintains IOP control for years without medications.
- Laser peripheral iridotomy (LPI): treatment for angle-closure/acute attack - creates a hole in peripheral iris to relieve pupillary block
- Diode laser cycloablation: destroys ciliary body; reserved for refractory cases
Surgery
- Trabeculectomy: creates a fistula between the anterior chamber and episcleral space (bleb filtration). Augmented with mitomycin C (antifibrotic) to reduce scarring
- Tube-shunt (glaucoma drainage device): synthetic tube drains aqueous to an equatorial reservoir; used in refractory cases or after failed trabeculectomy
- Minimally invasive glaucoma surgery (MIGS): e.g., iStent, Hydrus - lower risk but more modest IOP reduction
For acute angle-closure crisis:
- Immediate IOP lowering: IV acetazolamide, IV mannitol (hyperosmotic), topical beta-blocker + alpha agonist + pilocarpine (miotic to pull iris away)
- Definitive: Laser peripheral iridotomy to both eyes (prophylactic in the fellow eye)
Optic Nerve Changes (Key Exam Point)
Progressive optic nerve cupping is the hallmark:
- Normal C:D ratio: 0.3-0.5
- Glaucoma: focal notching (especially inferior > superior > nasal > temporal - "ISNT rule"), pallor, RNFL haemorrhages
- Baring of circumlinear vessels, bayoneting of vessels at disc margin
Prognosis
- Glaucoma is the second leading cause of blindness worldwide (after cataracts) and the leading cause of irreversible blindness
- Vision loss is permanent; treatment halts or slows progression but does not restore lost vision
- Early detection and sustained IOP reduction are the only proven strategies to preserve vision
Recent evidence (2025): A systematic review and meta-analysis (Ramji et al., Am J Ophthalmol 2025, PMID 40404077) found that trabeculectomy augmented with anti-VEGF improves surgical outcomes in glaucoma compared to trabeculectomy alone.
Sources:
- Goldman-Cecil Medicine, International Edition (p. 612-650)
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition
- Robbins & Kumar Basic Pathology (p. 868-869)
- Textbook of Family Medicine, 9th Edition
This is a shared conversation. Sign in to Orris to start your own chat.