A 60 year old lady had a fall in bathroom. After that she had pain in her right hip. She had difficulty in putting weight on her right lower limb. On examination, there was external rotation and shortening if her right lower limb. What is most likely diagnosis? Describe classification, principles of management and complications of this fracture.
Reading File
Finding Sources
Finding Sources
Searching PubMed
"femoral neck fracture" AND management
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed to provide a comprehensive answer. Let me compile it:
Fractured Neck of Femur (Intracapsular Hip Fracture)
Diagnosis
The most likely diagnosis is a fracture of the neck of femur (subcapital/transcervical fracture), which is an intracapsular fracture.
Reasoning from the clinical triad:
- Elderly woman (60 years, likely osteoporotic)
- Low-energy fall (bathroom)
- Short, externally rotated limb + inability to weight-bear
The external rotation is explained by the psoas major, whose fulcrum is normally the femoral head in the acetabulum. When the neck is fractured, the psoas loses its fulcrum and its overriding action pulls the proximal femur upward and into external rotation. The adductor spasm worsens this deformity. Shortening occurs due to proximal displacement of the femoral shaft by the same muscle spasm. (Gray's Anatomy for Students, p. 784)
Classification
1. By Anatomical Location
The fracture line can be:
- Subcapital - just below the femoral head (most common, highest AVN risk)
- Transcervical - through the mid neck
- Basicervical - at the base of the neck (extracapsular, lower AVN risk)
2. Garden Classification (by Displacement) - Most Widely Used
| Grade | Description |
|---|---|
| Garden I | Incomplete fracture; valgus impacted (trabecular pattern intact) |
| Garden II | Complete fracture, non-displaced |
| Garden III | Complete fracture, partially displaced; trabecular patterns misaligned but neck-head contact maintained |
| Garden IV | Complete fracture, fully displaced; trabecular patterns paradoxically realigned |
Clinically, surgeons typically group these into two categories:
- Non-displaced: Garden I + II - can be treated with internal fixation
- Displaced: Garden III + IV - generally require arthroplasty in older patients
Limitation: Interobserver reliability between stages is low, and sagittal plane angulation is not captured. Fractures with ≥20 degrees of sagittal angulation should not be treated as Garden I/II.
3. Pauwels Classification (by Fracture Angle / Shear Force)
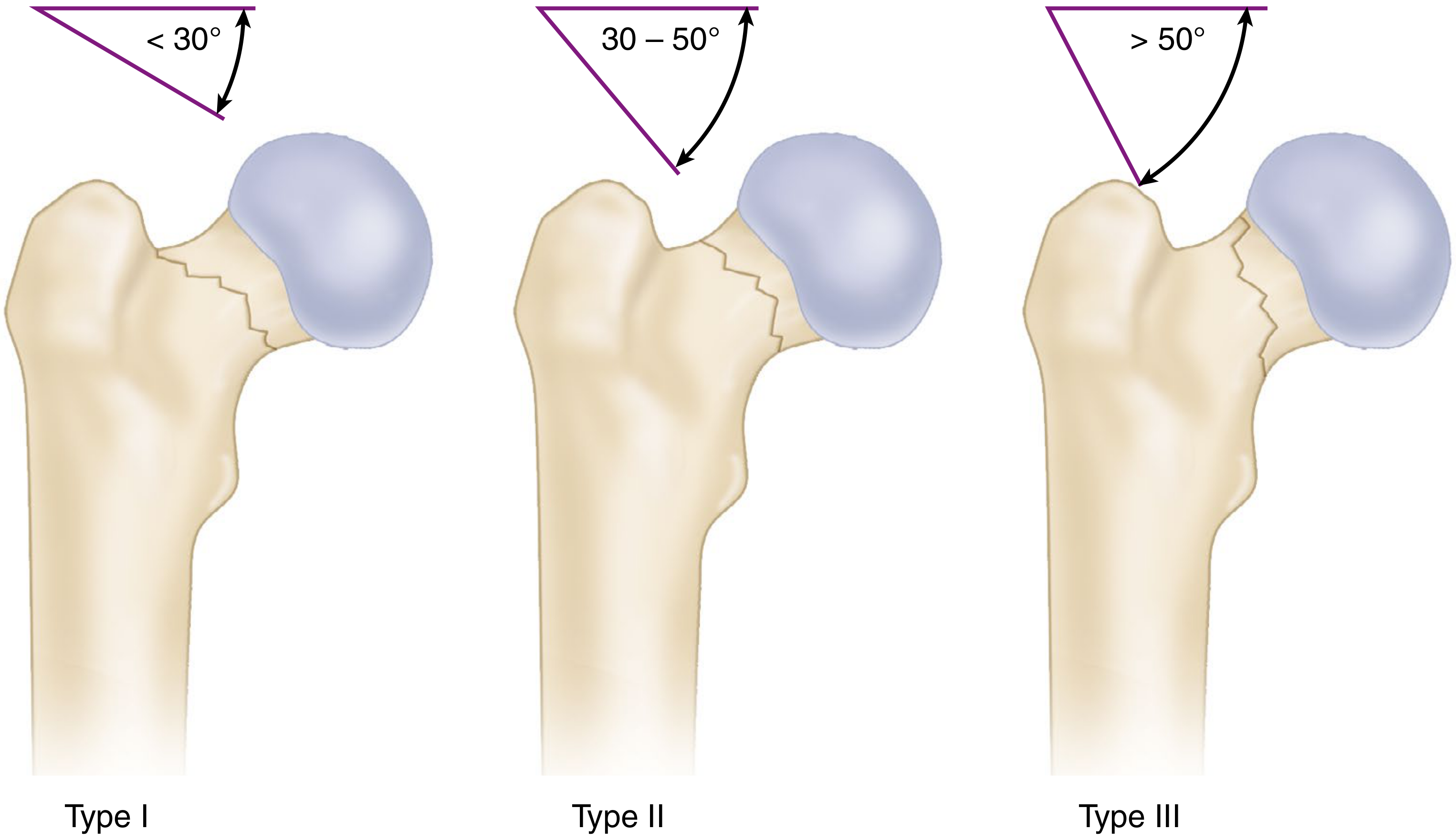
The angle is measured between the fracture line and the horizontal:
| Type | Angle | Biomechanics |
|---|---|---|
| Type I | <30° | Mostly compressive forces; stable |
| Type II | 30-50° | Mixed; intermediate stability |
| Type III | >50° | Predominantly shear; most unstable, high nonunion/AVN risk |
More vertical fractures = more shear at the fracture site = poorer prognosis with fixation alone. (Campbell's Operative Orthopaedics 15th Ed, 2026)
Blood Supply - The Core Problem
Three sources supply the femoral head:
- Retinacular vessels (deep to the capsule, in the retinacula fibers) - the most important
- Medullary vessels (attenuated in the elderly due to fatty marrow replacement)
- Ligamentum teres artery (also attenuated with age and atherosclerosis)
In an intracapsular fracture, the retinacular vessels are torn, leaving the femoral head ischemic. This is why avascular necrosis (AVN/osteonecrosis) is the hallmark complication of this fracture, and why arthroplasty is often required.
Principles of Management
Initial Management
- Analgesia and resuscitation
- AP pelvis radiograph (mandatory before any manipulation)
- Pre-operative optimization: treat coexisting diseases (cardiac, respiratory, anticoagulation)
- Skin/skeletal traction is NOT recommended as definitive treatment (high mortality)
Operative Treatment - Strongly Preferred
Non-operative management carries a 44.9% 30-day mortality vs 2.0% with operative treatment; operative management is considered mandatory except in extremely unusual circumstances (e.g., non-ambulatory, terminally ill). (Campbell's 2026)
Decision Algorithm: Internal Fixation vs. Arthroplasty
The key variables are: age, displacement, physiological fitness, and pre-injury function.
A. Non-displaced (Garden I/II) - in all age groups:
- Internal fixation with cannulated screws (3 partially-threaded screws in inverted triangle, or sliding hip screw)
- Femoral Neck System (FNS) is a newer option with lower AVN and shortening rates
- Capsulotomy should be considered in young patients to relieve intracapsular tamponade
B. Displaced (Garden III/IV) in older/physiologically elderly patients:
- Hemiarthroplasty - femoral head replaced; acetabulum preserved
- Bipolar heads preferred over monopolar (lower revision rates)
- Cemented stems favored over cementless
- Reserved for patients with: short life expectancy, significant comorbidities, cognitive impairment
- Total Hip Arthroplasty (THA) - both femoral and acetabular components replaced
- Preferred in: community ambulators with >5-year life expectancy, women <75 years, ASA I-II
- Benefits: superior function scores, less pain, better ambulation, lower reoperation rates
- Drawback: slightly higher dislocation rate (mitigated with direct anterior approach)
- Cost-effective from age 47 (with mild comorbidity) to 54+ years
C. Displaced fractures in young patients (<50 years):
- Emergency ORIF (open reduction and internal fixation)
- Anatomical reduction is the single most important factor in outcome
- Whitman technique for closed reduction (traction-abduction-internal rotation)
- Garden alignment index used to verify reduction quality (target: 160-180° on AP)
- Urgent surgery to restore blood supply and prevent AVN
Complications
Early Complications
| Complication | Notes |
|---|---|
| Deep Vein Thrombosis / Pulmonary Embolism | Most common early complication; prophylaxis mandatory |
| Chest infection / Pneumonia | From immobility, especially in elderly |
| Urinary tract infection | From catheterization and immobility |
| Pressure sores | Over sacrum, heels; preventable with nursing care |
| Fat embolism | Rare but serious |
Late Complications
| Complication | Notes |
|---|---|
| Avascular necrosis (Osteonecrosis) | 23% overall incidence in younger patients (meta-analysis of 18 studies). Due to disruption of retinacular vessels at time of fracture. May present months-years later with groin pain and collapse of femoral head |
| Non-union | 9% incidence in younger patients. Higher with Pauwels type III (11-16%). Related to poor reduction, inadequate fixation, or avascularity |
| Implant failure / Screw cut-out | Especially with varus malreduction |
| Acetabular erosion | After hemiarthroplasty (monopolar heads particularly) |
| Prosthetic dislocation | After THA (~2-3%); higher with posterior approach |
| Periprosthetic fracture | Around the prosthesis stem |
| Leg length discrepancy | From malreduction or shortening |
| Post-traumatic arthritis | Especially after femoral head fractures (53% at 10 years) |
| Mortality | 30-day mortality ~2% operative; 1-year mortality ~17.6% even with surgery in elderly |
Key Prognostic Factors for AVN and Non-union:
- Quality of reduction (the most modifiable factor)
- Displacement at time of injury
- Time to surgery (urgent in young patients)
- Age and pre-existing vascular disease
- Pauwels angle (higher angle = more shear = worse prognosis)
Sources:
- Campbell's Operative Orthopaedics 15th Ed 2026, Chapter 60 (Fractures of the Femoral Neck)
- Gray's Anatomy for Students, p. 784
- Recent meta-analysis (PMID 39581960): osteonecrosis incidence 23% in adolescents after surgery
This is a shared conversation. Sign in to Orris to start your own chat.