Traumatic knee arthrotomy what's it explain etiology signs and symptoms and investigations and evaluation treatment explain in detail with appropriate illustrative diagrams and images and diagrams
Reading File
Finding Sources
Finding Sources
Searching the Web
traumatic knee arthrotomy etiology signs symptoms investigation treatment orthopedics
Reading File
Finding Sources
Reading Web Page
https://www.nuemblog.com/blog/traumatic-arthrotomy
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Searching PubMed
traumatic knee arthrotomy diagnosis treatment
Reading File
Searching the Web
traumatic knee arthrotomy saline load test CT scan pneumarthrosis diagnosis images
Loading Image
I now have all the content needed for a comprehensive, well-illustrated answer. Let me compose the full response.
Traumatic Knee Arthrotomy - A Comprehensive Review
1. Definition
Traumatic knee arthrotomy is a soft-tissue injury over the knee in which the wound penetrates through the skin, subcutaneous tissue, and the joint capsule into the sterile intra-articular space of the knee joint. It creates a direct communication between the external environment and the joint cavity.
The knee is by far the most commonly involved joint in open joint injuries, accounting for 53% to 91% of all open joint wounds.
Campbell's Operative Orthopaedics 15th Ed, p. 2772
2. Anatomy Relevant to the Injury
The knee joint capsule is a fibrous sleeve enclosing the distal femur, proximal tibia, and patella. It is reinforced by:
- Medial and lateral collateral ligaments
- Quadriceps/patellar tendon anteriorly
- Posterior capsule with oblique popliteal ligament
- Synovial membrane lining the inner capsule (produces synovial fluid)
When the capsule is breached, the normally sterile synovial space is exposed to environmental organisms, leading to the risk of septic arthritis - a potentially joint-destroying complication.
3. Etiology and Mechanisms
Traumatic arthrotomy results from any periarticular penetrating or laceration injury sufficient to breach the joint capsule:
| Mechanism | Details |
|---|---|
| Stab wounds | Knives, glass, sharp objects - most common in civilian settings |
| Gunshot wounds (GSW) | Low-velocity (handguns) and high-velocity (rifles); incidence rising with civilian gun injuries |
| Falls onto sharp objects | Occupational injuries - often with knee in flexed position |
| Lacerations from machinery | Industrial/farm accidents |
| Human/animal bites | Higher infection risk, polymicrobial organisms |
| Underwater injuries | Propeller blades, fish hooks; risk of unusual pathogens |
| Blast/shrapnel injuries | Military/explosive trauma |
| Iatrogenic | Rare; misplaced injections, failed arthrocentesis |
Important: Occupational knee injuries often occur with the knee flexed. The position of the knee at the time of injury alters the trajectory - a wound that appears remote from the joint in extension may have communicated with it when flexed. Always reconstruct the injury position. Tintinalli's Emergency Medicine, p. 1899
4. Pathophysiology
External wound breaches skin + capsule
↓
Environmental bacteria enter sterile joint space
↓
Synovial fluid provides excellent bacterial growth medium
↓
Inflammatory response → synovitis → effusion
↓
Untreated: Septic arthritis → cartilage destruction → joint failure
The high morbidity of septic arthritis (including permanent loss of joint function) makes a high index of suspicion mandatory for any periarticular wound.
5. Classification (Patzakis et al.)
Three injury types are recognized:
- Open joint injury with associated fracture - most complex, highest infection risk
- Open joint injury without fracture - isolated capsular breach
- Gunshot wounds - unique contamination profile, may have bullet fragments, lead toxicity risk
6. Signs and Symptoms
History
- Penetrating trauma or high-energy injury near the knee
- Wound over the anterior, medial, or lateral aspect of the knee
- Patients often present with a laceration and may not realize the joint is involved
Symptoms
- Knee pain - often disproportionate to wound size
- Swelling - rapid hemarthrosis/effusion if joint violated
- Restricted range of motion due to pain and effusion
- Wound discharge - straw-colored, oily fluid (synovial fluid) exuding from wound is pathognomonic
- Bubbles/crepitus at the wound base
Physical Examination Signs
| Sign | Significance |
|---|---|
| Visible synovial fluid (straw-colored, viscous, oily) from wound | Pathognomonic of joint violation |
| Air bubbles at wound base | Suggests intra-articular communication |
| Visible bone, cartilage, or tendon | Indicates deep penetration |
| Joint effusion/hemarthrosis | Suggests intra-articular injury |
| Reduced ROM/painful motion | Intra-articular pathology |
| Wound over joint line | High-suspicion location |
The absence of synovial fluid or bubbles does NOT rule out arthrotomy - the wound must be formally tested.
7. Investigations and Evaluation
Step 1 - Initial Assessment
Neurovascular examination is paramount - especially in GSW cases. Assess:
- Distal pulses (popliteal, dorsalis pedis, posterior tibial)
- Capillary refill
- Motor and sensory function (common peroneal nerve is at risk)
- Ankle-brachial index if vascular injury suspected
Step 2 - Wound Exploration
- Anesthetize the wound locally for comfort
- Irrigate with sterile saline
- Visualize the base of the wound thoroughly
- Use a hemostat or probe to detect tunneling
- Look for: synovial fluid, bubbles, visible bone/tendon/cartilage
Step 3 - Radiographic Investigations
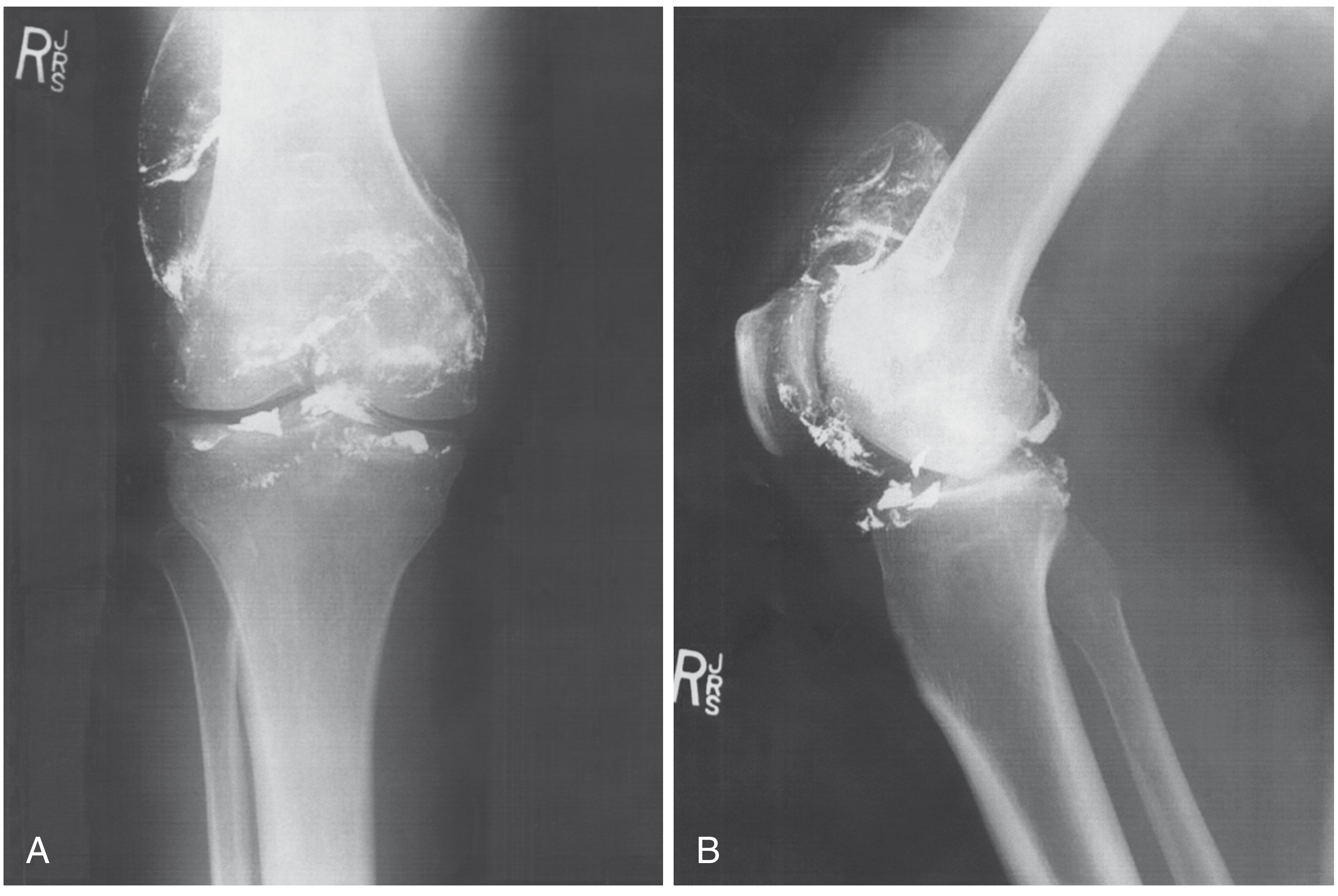
Plain Radiographs (X-ray) - First Line
- AP and lateral views of the knee
- Look for: intra-articular air (pneumarthrosis - highly specific), fractures, bullet fragments, osteochondral fragments, foreign bodies
- Radiopaque foreign bodies (metal, glass) are visible
- Pneumarthrosis on plain film is diagnostic of joint violation

CT Scan - Currently the Investigation of Choice
- Now the preferred imaging modality for traumatic arthrotomy
- Look for pneumarthrosis (intra-articular gas/air on CT)
- A 2013 study by Konda et al. found CT to be 100% sensitive and specific for diagnosing traumatic knee arthrotomy (using arthroscopy or septic arthritis as gold standard)
- Also helps assess fracture complexity and surgical planning
- CT scan can identify periarticular wounds that do NOT require surgical intervention - avoiding unnecessary OR trips
- Sensitivity reported at 60-100% across studies; CT is superior to clinical exam alone
MRI
- Not routinely used for acute assessment
- Useful for associated ligament/meniscus/osteochondral injuries in subacute/chronic settings
Step 4 - The Saline Load Test (SLT)
The traditional gold standard for clinical diagnosis:
Technique:
- Prepare a distant injection site (away from the wound) using sterile technique
- Inject sterile normal saline into the joint space using a needle inserted through clean skin
- Observe the wound for extravasation of saline (positive = joint violated)
- Methylene blue dye may be added (some evidence of modest sensitivity improvement)
Volume Recommendations and Sensitivity:
| Saline Volume | Sensitivity |
|---|---|
| 50 mL | 46% (Keese, 2007) |
| 60 mL (traditional) | ~60% |
| 155 mL | ~90% |
| 194 mL | 95% |
The traditional 60 mL volume is insufficient - higher volumes (155-194 mL) are needed for adequate sensitivity. Failure to use adequate volume leads to false negatives. Tintinalli's Emergency Medicine, p. 1899; Core EM
Limitations of SLT:
- Volume-dependent sensitivity
- Does not identify the extent or complexity of the injury
- Negative SLT does not definitively rule out arthrotomy
- CT scan is now preferred over SLT at many centers
Step 5 - Laboratory Tests
- CBC, ESR, CRP (baseline; elevated in established infection)
- Blood cultures if septic arthritis suspected
- Synovial fluid analysis if joint is aspirated (WBC >2500/mm³ with >60% PMNs suggests infection)
- If GSW: blood lead level if intra-articular fragments present
- Tetanus immune status
8. Treatment
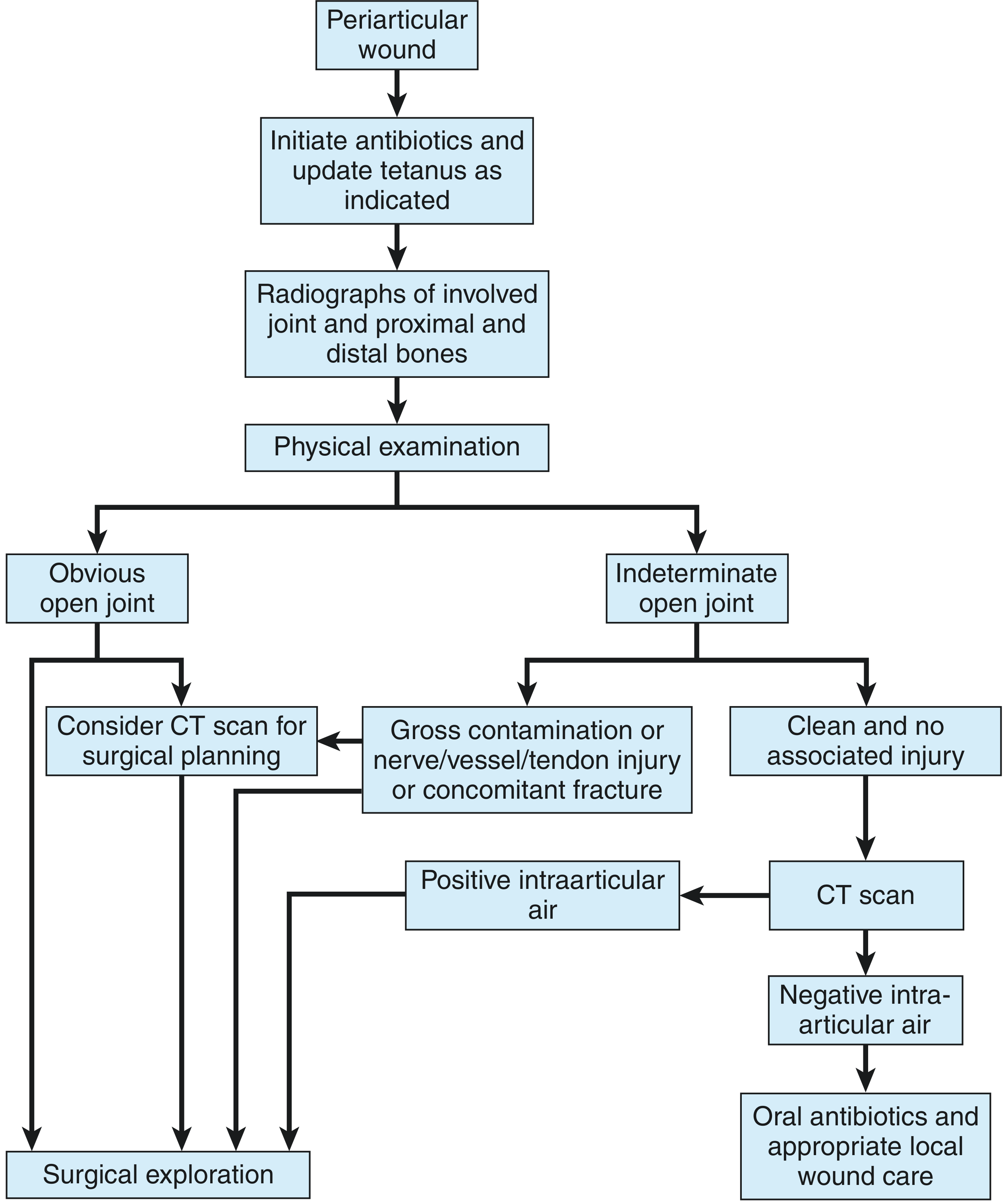
The treatment algorithm below summarizes the approach:
Initial/Emergency Management (All patients)
- Antibiotics - Start empirical IV antibiotics immediately
- First-generation cephalosporin (e.g., cefazolin) covers Staph and Strep - adequate for most wounds
- Broader coverage needed for: human/animal bites (add amoxicillin-clavulanate or piperacillin-tazobactam), underwater injuries, fecal contamination
- Tetanus prophylaxis - Update as indicated by immunization status
- Wound coverage - Moist sterile dressing; do not close before formal OR washout
- Splint/immobilize the joint
- Orthopaedic surgery consultation - Emergent for confirmed arthrotomy
Decision Pathway
If the joint violation is OBVIOUS (synovial fluid visible, gross contamination):
- Emergent surgical exploration in OR
- Consider CT for surgical planning and fracture assessment
If the joint violation is INDETERMINATE:
- Obtain CT scan
- If CT shows positive intra-articular air → surgical exploration
- If CT is negative (no intra-articular air) + no contamination/nerve/vessel injury → oral antibiotics + local wound care + close follow-up
Definitive Surgical Treatment
Formal surgical debridement and washout is the cornerstone of treatment for confirmed arthrotomy:
Open Surgical Approach:
- Formal arthrotomy incision (existing wound may be incorporated if alignment allows)
- Thorough joint irrigation with copious sterile saline (minimum 9-10 L recommended)
- Debridement of devitalized tissue, foreign material, bone fragments
- Repair of injured structures (ligaments, tendons) as anatomically feasible
- Primary closure of joint capsule and wound in most cases
- Suction drainage may be placed for severely contaminated wounds
Arthroscopic Approach:
- Preferred when open fracture reduction is NOT required
- Advantages: shorter hospital stay, less postoperative pain, better cosmetic result, can identify intra-articular injuries (meniscus, ligament, cartilage)
- Same debridement and irrigation principles apply
Closed Irrigation and Suction:
- NOT routinely recommended after arthrotomy
- Reserved only for severe contamination or when soft-tissue closure is desired
- These drainage tubes themselves may become a source of contamination (Patzakis et al.)
Fracture Management (if present)
Depends on fracture stability and pattern:
- Casting or bracing (stable, non-displaced)
- Open reduction and internal fixation (displaced intra-articular fractures)
- External fixation (highly comminuted, soft tissue compromise)
- Arthroscopic fixation for osteochondral fragments
Soft-Tissue Coverage
- Skin grafts or flaps (rotational, free) for large defects
- Wound VAC (negative pressure wound therapy) for contaminated wounds requiring staged closure
Gunshot Wound Specifics
- Bullet fragments in the joint must be removed (cartilage damage, risk of lead toxicity)
- Arthroscopic removal preferred for small fragments
- Monitor blood lead levels for intra-articular fragments
- Lead poisoning signs: microcytic anemia, nausea, abdominal pain, weakness; treat with chelation + fragment removal
Postoperative Care
- Brace locked in extension initially
- Range-of-motion exercises started early
- Continuous passive motion (CPM) machine may be used
- Close monitoring for signs of infection (fever, wound breakdown, joint effusion)
- Repeat debridement if signs of infection develop
- Rehabilitation: progressive weight bearing and physiotherapy
9. Antibiotic Protocol Summary
| Wound Type | Antibiotic Choice |
|---|---|
| Clean laceration | Cefazolin (1st gen cephalosporin) |
| Contaminated wound | Add gentamicin or broader gram-negative coverage |
| Human/animal bite | Add amoxicillin-clavulanate or piperacillin-tazobactam |
| Underwater injury | Add ciprofloxacin (Aeromonas coverage) |
| Fecal contamination | Metronidazole added for anaerobic coverage |
Duration: Continue perioperative antibiotics 24-48 hours post-surgery in clean wounds; longer for contaminated cases.
10. Complications
| Complication | Details |
|---|---|
| Septic arthritis | Most feared - cartilage destruction, joint failure if untreated |
| Osteomyelitis | Secondary bone infection |
| Chronic synovitis | Persistent inflammation, reduced ROM |
| Wound dehiscence | Especially in contaminated wounds |
| Lead poisoning | From retained intra-articular bullet fragments (may present years later) |
| Post-traumatic arthritis | Long-term joint degeneration |
| Ligament/meniscus injury | Associated structural damage |
| Vascular injury | Popliteal artery injury in posterior wounds |
| Nerve injury | Common peroneal nerve at lateral knee |
11. Prognosis
When diagnosed and treated promptly with adequate surgical debridement and appropriate antibiotics, outcomes are generally good. Patzakis et al. reported only a 2.1% infection rate (3/140 patients) with aggressive treatment. Delayed diagnosis or treatment is the primary driver of poor outcomes. High-velocity GSW with comminuted fractures and severe soft-tissue damage carry the highest morbidity.
12. Key Take-Home Points
- Traumatic knee arthrotomy = any wound that breaches the joint capsule - requires emergent orthopedic consultation
- The knee is the most commonly involved joint (53-91% of open joint wounds)
- A seemingly small wound can communicate with the joint - never dismiss periarticular lacerations
- Visible synovial fluid is pathognomonic; its absence does not rule out arthrotomy
- CT scan is the current investigation of choice (100% sensitivity/specificity in key studies)
- Saline load test requires 194 mL for adequate (95%) sensitivity - traditional 60 mL is insufficient
- Definitive treatment is OR washout + debridement with IV antibiotics
- Arthroscopic washout is preferred when no fracture requires open reduction
- Intra-articular bullets must be removed to prevent cartilage damage and lead toxicity
Sources:
- Campbell's Operative Orthopaedics 15th Ed 2026, Chapter 50, pp. 2772-2774
- Tintinalli's Emergency Medicine - A Comprehensive Study Guide, Chapter 274, pp. 1899-1900
- Brubacher JW, Grote CW, Tilley MB. Traumatic arthrotomy. J Am Acad Orthop Surg. 2020;28:102
- Konda SR et al. CT scan to detect traumatic arthrotomies. J Orthop Trauma. 2013;27:498-504 (PMID: 23287770)
- Nord RM et al. Detection of traumatic arthrotomy of the knee using the saline solution load test. JBJS. 2009;91(1):65-70
This is a shared conversation. Sign in to Orris to start your own chat.