Brrach presentarion obes and gyne
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive, authoritative content from multiple textbooks. Here is the complete guide to Breech Presentation in Obstetrics and Gynaecology:
Breech Presentation - Obstetrics & Gynaecology
1. Definition & Incidence
Breech presentation is when the fetal buttocks or lower extremities occupy the lower pole of the uterus, with the head at the fundus.
- Incidence is 3-4% of all deliveries at term
- Frequency decreases with advancing gestation:
- 24% at 18-22 weeks
- 8% at 28-30 weeks
- 7% at 34 weeks
- 2.8% at 38-40 weeks
- ~25-30% of all preterm infants (<28 weeks) present as breech
(Creasy & Resnik's Maternal-Fetal Medicine, p. 953)
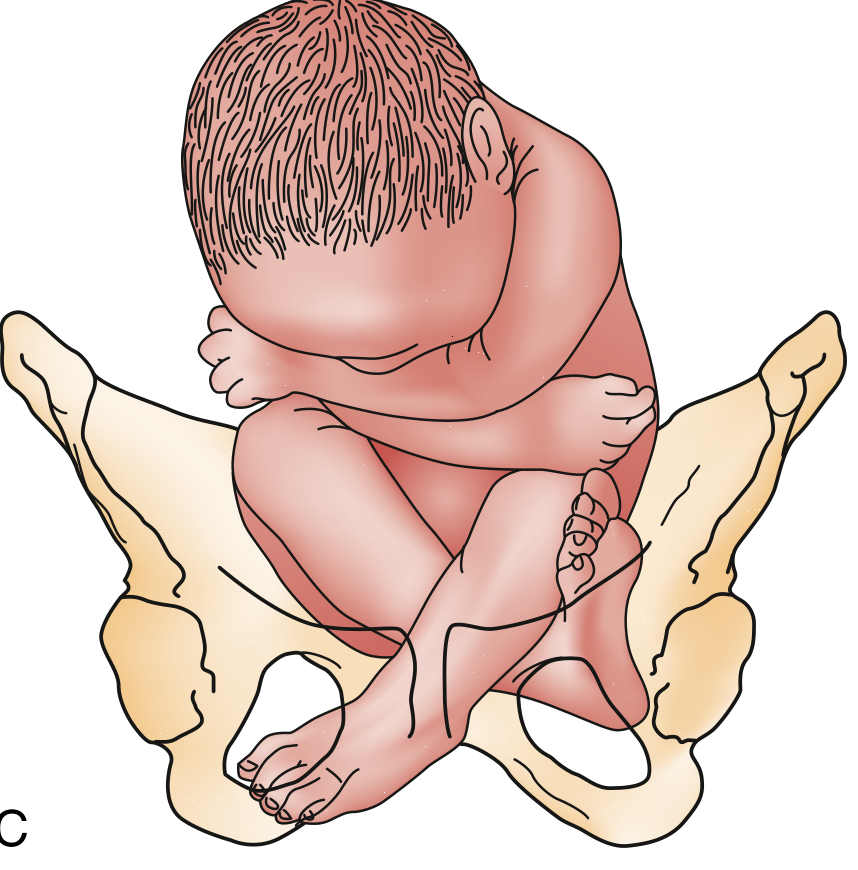
2. Types of Breech Presentation
A. Frank Breech (most common, ~65-70%)
Hips flexed, knees extended - legs lie alongside the trunk. The buttocks are the presenting part.
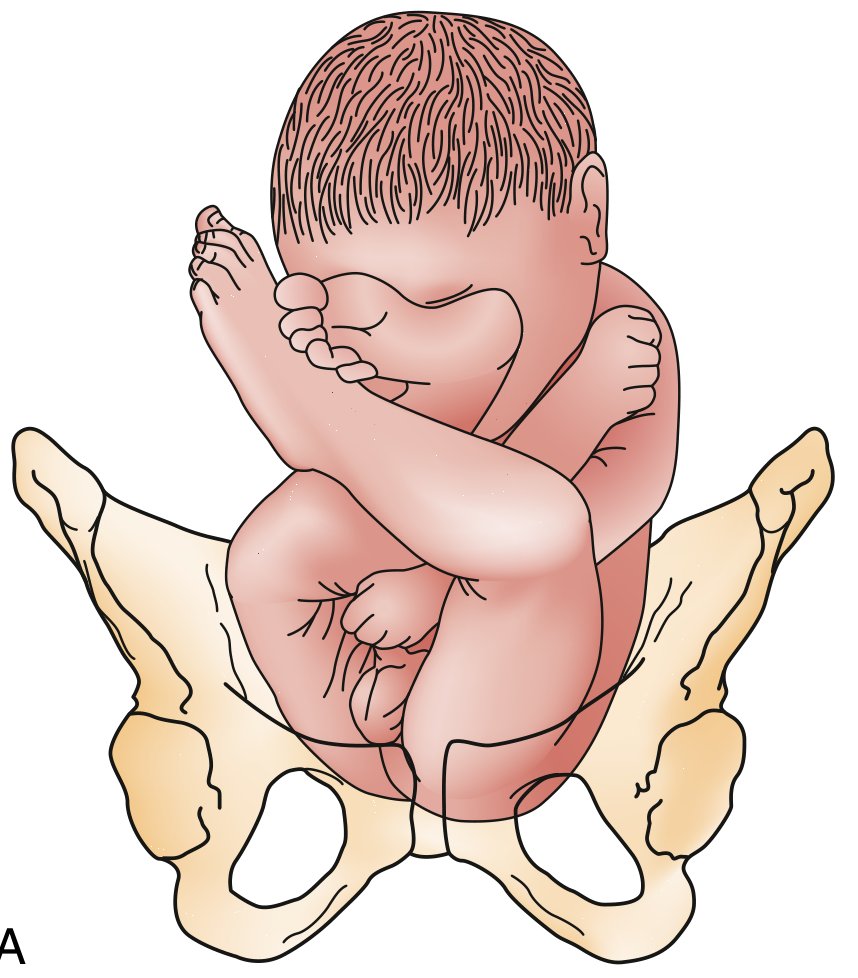
B. Complete Breech (~10%)
Both hips and knees flexed - fetus is in a "crossed-leg" or "tailor-sitting" position.
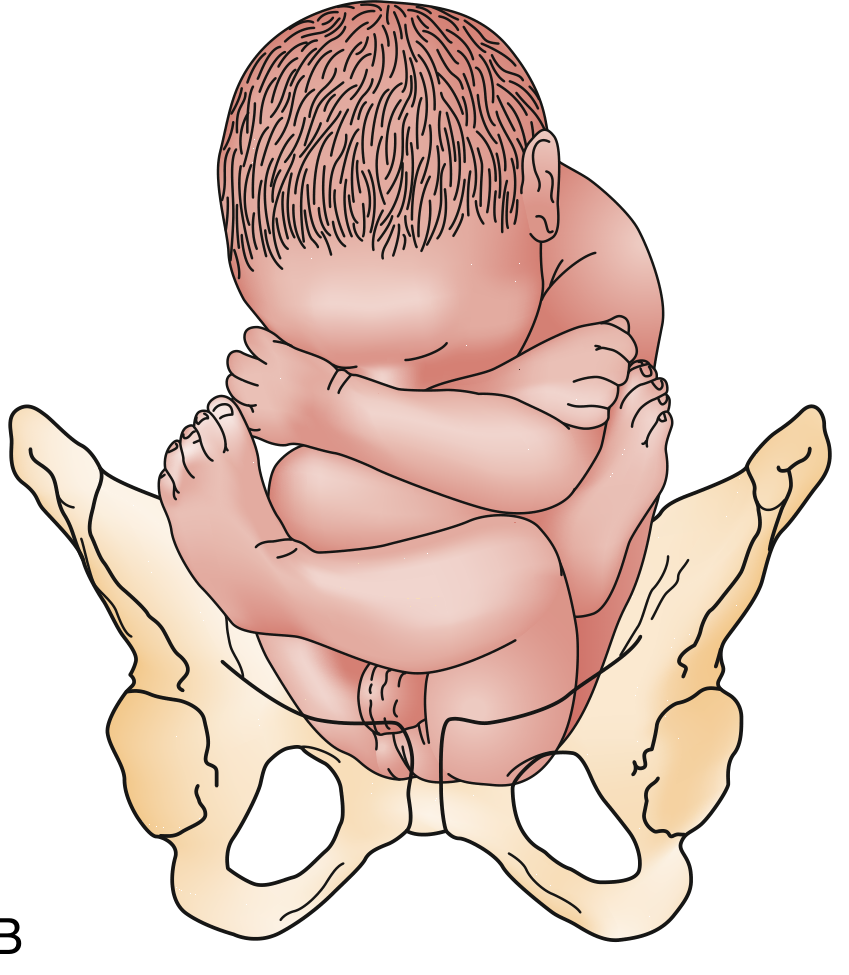
C. Incomplete / Footling Breech (~20-25%)
One or both feet are the presenting part, with the hip(s) partially or fully extended. This is the highest risk type due to cord prolapse.
(Rosen's Emergency Medicine, p. 3416)
3. Etiology / Predisposing Factors
| Category | Examples |
|---|---|
| Uterine factors | Fundal-cornual placental implantation (7% of all pregnancies), uterine anomalies (bicornuate, septate), fibroids |
| Fetal factors | Prematurity, multiple gestation, fetal neuromuscular disorders, hydrocephalus, anencephaly |
| Placental/fluid | Polyhydramnios, oligohydramnios, placenta previa |
| Pelvic factors | Contracted pelvis, pelvic tumors |
- Term breech is associated with fundal-cornual placental implantation - the fetus may adopt breech because it is more "comfortable" given limited space
- Infants with neuromuscular disorders have disproportionately high rates of breech presentation (reduced ability to spontaneously rotate)
- Importantly, 5-year motor skill scores in children born breech are lower regardless of delivery route, suggesting the breech position itself may reflect an underlying fetal issue
(Creasy & Resnik's, p. 953)
4. Risks / Complications
Fetal/Neonatal Risks
| Risk | Mechanism |
|---|---|
| Umbilical cord prolapse | Especially in footling breech - poorly fitting presenting part leaves space for cord |
| Head entrapment | After-coming head trapped by incompletely dilated cervix - especially in preterm <1500 g |
| Birth trauma | Extension of the head, nuchal arm position, brachial plexus injury |
| Asphyxia/hypoxia | Cord compression, delay in head delivery |
| Spinal cord injury | If fetal neck is hyperextended ("star-gazing fetus") |
| Perinatal mortality | Higher than vertex at all gestational ages and birth weights |
Maternal Risks
- Higher caesarean section rate
- Complications of operative delivery
5. Diagnosis
Leopold's Maneuvers
- 1st maneuver (fundal grip): Hard, round, ballotable head felt at the fundus
- 3rd maneuver (Pawlik's grip): Soft, irregular, non-ballotable buttocks in the lower pole
- 4th maneuver: Confirms presenting part above pelvic inlet
Vaginal Examination
- Feel soft irregular surface (buttocks), anal orifice (flanked by bone on only two sides - vs. fetal face with complete bony ring)
- If no fontanel is identified, suspect breech
Ultrasound (most reliable)
- Confirms type of breech, fetal position, estimated weight, degree of head flexion/extension, placental location, amniotic fluid volume, fetal anomalies
- Hyperextended fetal neck on USS = contraindication to vaginal delivery (high risk of spinal cord injury)
6. Management
Step 1: External Cephalic Version (ECV)
ECV is the first-line management for term breech (offered at 36 weeks gestation).
- Success rate: ~65% at 36 weeks
- Reduces caesarean risk by 50% overall for breech patients
- Technique: Tocolysis (e.g. terbutaline/ritodrine) is used to relax the uterus. The fetus is gently rotated to cephalic position through the maternal abdomen under continuous CTG and ultrasound monitoring.
- Epidural analgesia may improve success rate after a failed first attempt
Contraindications to ECV:
- Uterine anomalies
- Third-trimester bleeding
- Multiple gestation
- Oligohydramnios
- Uteroplacental insufficiency
- Nuchal cord on USS
- Previous caesarean or significant uterine surgery
- Obvious cephalopelvic disproportion (CPD)
(Creasy & Resnik's, p. 954)
Step 2: Mode of Delivery
ACOG Recommendation
If ECV fails or is contraindicated at term: planned caesarean section is recommended.
This is supported by the Term Breech Trial (Hannah et al., 2000) - a large multicentre RCT of 2,088 subjects showing:
- Significantly greater perinatal morbidity and mortality with planned vaginal delivery
- No significant difference in maternal mortality or serious morbidity
- Led to a worldwide shift toward elective CS for term breech
(Creasy & Resnik's, p. 953-954)
Criteria for Allowing Vaginal Breech Delivery (selected cases only)
When an experienced obstetrician is present, vaginal delivery may be considered if all of the following are met:
| Criterion | Detail |
|---|---|
| Presentation | Frank or complete breech only (NOT footling) |
| Estimated fetal weight | 2000 - 3800 g |
| Pelvis | Normal gynecoid pelvis with adequate measurements |
| Fetal head | Flexed (not hyperextended) |
| Gestational age | Term |
| Operator | Skilled, experienced obstetrician available |
| Setting | Full theatre/CS capability immediately available |
- Oxytocin use is controversial in breech labor; 64% of perinatal deaths in the Hannah trial's vaginal arm occurred in induced/augmented labors
7. Mechanism of Labor in Breech (Vaginal Delivery)
- Engagement - Bitrochanteric diameter engages in an oblique diameter of the pelvic inlet
- Descent - Anterior hip descends more rapidly
- Internal rotation - Bitrochanteric diameter assumes the AP position
- Lateral flexion - Anterior hip catches beneath symphysis pubis; posterior hip born first
- Shoulder engagement - Shoulders engage in an oblique orientation; rotate to AP diameter at outlet; anterior shoulder appears beneath symphysis, posterior shoulder delivered first
- Head delivery - Head engages in same diameter as shoulders; flexion, descent, and rotation bring posterior neck under symphysis; head is born in flexion
(Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 1352)
8. Types of Breech Delivery
| Type | Description |
|---|---|
| Spontaneous | Delivered without manipulation/traction; rare at term |
| Partial (Assisted) Breech Extraction | Spontaneous to umbilicus, then clinician extracts remainder - most common for assisted vaginal breech |
| Total Breech Extraction | Entire body extracted by clinician; higher risk |
9. Delivery Technique (Emergency / Assisted Vaginal Breech)
- Do NOT apply traction until the infant delivers to the umbilicus spontaneously
- Once umbilicus is visible: thumbs on sacrum, grasp fetal pelvis; keep trunk at ≤45° to horizontal
- Maintain sacrum anterior; allow arms to deliver with slight oblique rotation
- For the after-coming head:
- Mauriceau maneuver: One hand on occiput/shoulders applying flexing pressure; fingers of other hand on maxillae to maintain cervical flexion. Assistant applies suprapubic pressure.
- Only attempt once fetal elbows and chin have entered the pelvic inlet (to avoid Moro reflex)
- Piper forceps may be applied to the after-coming head if there is difficulty (reduces neonatal mortality from breech)
- Episiotomy may be needed for full-term infant
(Tintinalli's Emergency Medicine; Rosen's Emergency Medicine, p. 3416)
10. Special Situations
| Situation | Management |
|---|---|
| Preterm breech (<28 wks) | CS may reduce neonatal mortality vs. vaginal delivery at 24-32 weeks; individual assessment required |
| Second twin in breech | ACOG recommendation for CS does NOT apply - vaginal delivery of a breech second twin is acceptable |
| Footling/incomplete breech | NOT safe for vaginal delivery - high cord prolapse risk; immediate obstetric consultation, consider tocolysis (terbutaline SC) to buy time for CS |
| Hyperextended head | Vaginal delivery contraindicated - very high spinal cord injury risk |
| Emergency (no time for CS) | Allow delivery to proceed spontaneously to umbilicus; use Mauriceau maneuver for head; call senior help immediately |
11. Prognosis / Long-term Outcome
- Long-term developmental outcome at 5 years does not differ significantly between infants delivered vaginally vs. by CS for breech presentation
- Higher rates of instrumental delivery and emergency CS occur even after successful ECV - the underlying breech etiology may persist as a risk factor
- Neonatal mortality risk: ~3/1000 with planned vaginal delivery; neurological injury ~7/1000; birth trauma ~7/1000 (meta-analysis data)
(Creasy & Resnik's, p. 954)
Quick Summary Table
| Feature | Detail |
|---|---|
| Incidence at term | 3-4% |
| Most common type | Frank breech (65-70%) |
| Highest risk type | Footling/incomplete |
| Key complication | Cord prolapse, head entrapment |
| First-line management | ECV at 36 weeks |
| ECV success rate | ~65% |
| Delivery of choice (term breech) | Planned caesarean section (ACOG) |
| Vaginal delivery allowed if | Frank/complete, 2000-3800g, normal pelvis, flexed head, skilled operator |
| Key maneuver for after-coming head | Mauriceau maneuver + Piper forceps |
Sources: Creasy & Resnik's Maternal-Fetal Medicine (Principles and Practice); Tintinalli's Emergency Medicine; Rosen's Emergency Medicine; Roberts and Hedges' Clinical Procedures in Emergency Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.