Lung abscess full details for md exam answer 15 marks from fishman and Murray
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have more than enough detailed content from both Fishman's and Murray & Nadel to write a comprehensive 15-mark MD exam answer. Let me compose the full answer now.
Lung Abscess - Comprehensive MD Exam Answer (15 Marks)
Sources: Fishman's Pulmonary Diseases and Disorders (Chapter 127) & Murray & Nadel's Textbook of Respiratory Medicine (Chapter 50)
Definition and Classification
A lung abscess is a localized area of suppurative necrosis of the lung parenchyma resulting in a cavity containing pus and necrotic debris, usually with an air-fluid level on imaging. It most commonly arises from polymicrobial anaerobic infection originating in the oral cavity.
Classification (Fishman's, p. 2242):
| Category | Description |
|---|---|
| Acute | Symptoms < 4-6 weeks |
| Chronic | Symptoms > 4-6 weeks (often > 1 month before seeking care) |
| Primary | Aspiration or pneumonia in an immunocompetent host |
| Secondary | Pre-existing condition (obstruction, immunodeficiency, spread from extrapulmonary site, bronchiectasis) |
| Putrid abscess | Foul-smelling; caused by anaerobic organisms |
| Nonspecific | No pathogen identified on culture |
Pathophysiology and Predisposing Conditions
Most lung abscesses result from aspiration of anaerobic bacteria from the gingival crevices of the oral cavity (Murray & Nadel, Ch. 50). The sequence is:
- Aspiration of oropharyngeal contents
- Pneumonitis develops over 7-14 days
- Tissue necrosis follows, creating a cavity
- Cavity may become lined by regenerated epithelium; local obstruction can produce bronchiectasis or emphysema in surrounding lung
Key predisposing conditions:
- Periodontal disease / poor dentition (major risk factor)
- Altered consciousness: alcoholism, sedating drugs, head trauma, seizures, general anesthesia
- Dysphagia or pharyngeal dysfunction
- Defective cough reflex
- Obstruction (neoplasm, foreign body)
- Immunocompromise (HIV, chemotherapy, transplant)
- Pulmonary embolism, bronchiectasis
- Previous cavitary disease (emphysema, old TB) - infection may proceed without frank necrosis
Edentulous patients rarely develop primary lung abscess; its occurrence in them should prompt a search for bronchial obstruction, pulmonary embolus, or septic embolus (Fishman's, p. 2242).
Anatomical Location
Because aspiration is the dominant mechanism, abscesses preferentially involve the most dependent lung segments:
- Posterior segment of the right upper lobe (most common)
- Apical segments of the lower lobes
- Less commonly: posterior segment of the left upper lobe
The right lung is more often affected because the right main bronchus is shorter, wider, and more vertical than the left, favoring aspiration into the right side (Murray & Nadel, Ch. 50).
Microbiology
Anaerobes are recoverable in up to 93% of patients with lung abscess (Fishman's, p. 2242):
- 46% have only anaerobes isolated
- 43% have a mixed anaerobic + aerobic infection (Bartlett and Finegold data)
Common anaerobes: Fusobacterium nucleatum, Prevotella species (denticola, intermedia, oris, buccae), Bacteroides fragilis, Peptostreptococcus species, microaerophilic streptococci
Aerobic/facultative organisms also implicated:
- Staphylococcus aureus (classically post-influenza; also in IV drug users)
- Klebsiella pneumoniae (especially upper lobe, in alcoholics; "currant jelly" sputum)
- Pseudomonas aeruginosa, Streptococcus pyogenes
- Nocardia asteroides, Rhodococcus equi (immunocompromised)
- Actinomyces species
Nosocomial lung abscess: Gram-negative bacteria with hospital-acquired resistance patterns predominate.
Uncommon but important causes (Fishman's, p. 2242):
- Legionella species, Burkholderia pseudomallei (melioidosis), Burkholderia mallei (glanders)
- Entamoeba histolytica - basilar portion of right lower lobe (almost always)
- Mycobacteria: M. tuberculosis, MAC, M. kansasii
- Fungi: Aspergillus, zygomycetes (Mucoraceae), Histoplasma, Blastomyces, Coccidioides - in diabetic/immunocompromised hosts
Clinical Features
Symptoms are typically subacute and indolent when caused by anaerobes (Murray & Nadel, Ch. 50):
- Fever, cough, sputum production (develops over weeks to months)
- Night sweats and weight loss
- Pleuritic chest pain
- Hemoptysis (may be minor or life-threatening)
- Foul-smelling / putrid sputum - highly suggestive of anaerobic infection
- Bad breath (halitosis)
Note: Absence of foul odor does NOT exclude anaerobes - some organisms do not produce malodorous metabolic products.
Secondary lung abscesses (e.g., from septic pulmonary emboli) can evolve rapidly over 48-72 hours, unlike the typical indolent course of primary abscesses (Fishman's, p. 2243).
Physical examination:
- Fever, possible decreased level of consciousness
- Poor dentition (important clue)
- Crackles, egophony, dullness to percussion (if pleural effusion present)
- Amphoric (cavernous) breath sounds over the cavity
Radiological Diagnosis
Chest X-ray classic appearance:
- Irregularly shaped cavity with an air-fluid level within a consolidation/infiltrate
- Location: posterior segments of upper lobes, superior segments of lower lobes
CT chest (preferred investigation) - Murray & Nadel, Ch. 50:
Features favoring lung abscess:
- Air-fluid level
- Surrounding parenchymal opacity (ground-glass or consolidation)
- Irregular ("shaggy") inner wall
- Round shape with similar dimensions on different views
- Does NOT compress adjacent lung
Features distinguishing from empyema:
- Empyema: oblong shape, smooth inner lining, compresses surrounding lung
- Abscess: round shape, ragged inner lining, no lung compression
Features suggesting malignancy:
- Nodular inner wall
- Wall thickness ≥ 16 mm
- Lymphadenopathy, pleural effusion
Septic emboli: Multiple distinct nodules (1-3 cm) with cavities in different stages, subpleural wedge-shaped infiltrates.
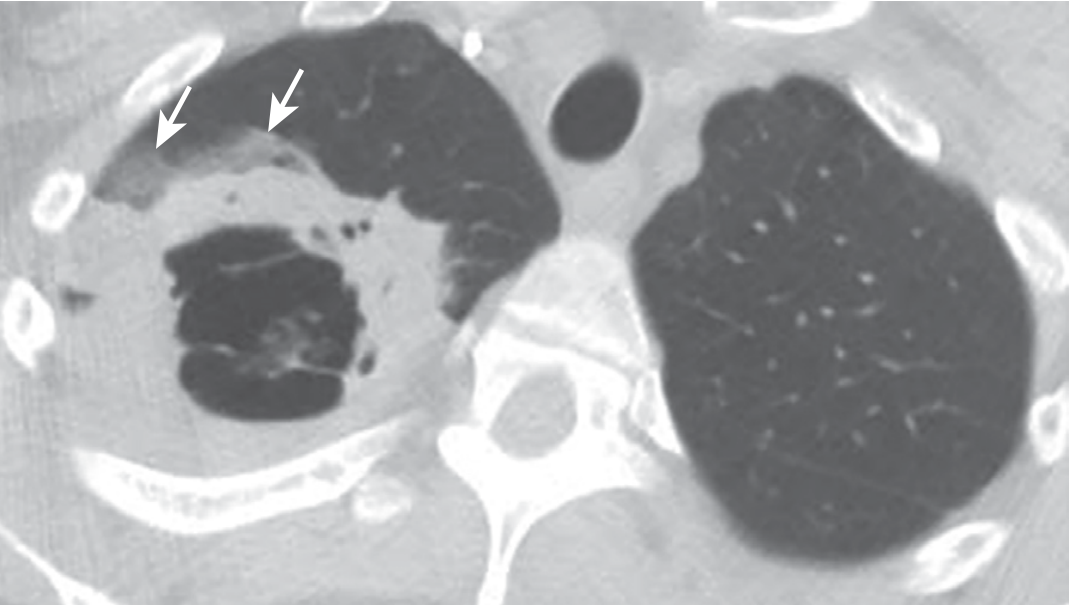
Figure: Axial CT showing a complex, thick-walled right apical cavity consistent with a pyogenic abscess; arrows indicate surrounding ground-glass opacity from hemorrhage (Murray & Nadel, Fig. 50.6)
Differential Diagnosis
Infectious cavities (Fishman's, Table 127-6):
- Bacterial: S. aureus, Enterobacteriaceae, Pseudomonas, Nocardia, Actinomyces
- Mycobacterial (often multifocal): TB, MAC, M. kansasii
- Fungal: Aspergillus, zygomycetes, Histoplasma, Coccidioides, Cryptococcus, PCP
- Parasitic: Entamoeba histolytica, Paragonimus westermani, Strongyloides
Non-infectious cavitating conditions:
- Bronchogenic carcinoma (cavitating squamous cell carcinoma)
- Septic embolism (endocarditis, IV drug use)
- Granulomatosis with polyangiitis (Wegener's)
- Pulmonary infarction
- Bronchiectasis, pulmonary sequestration
- Fluid-filled cysts (traumatic, hydatid)
Diagnostic Workup
- Chest X-ray - initial study; may need serial films to track evolution
- CT chest - preferred; defines extent, loculations, relationship to pleura, mediastinal structures; guides drainage
- Sputum - Gram stain and culture (aerobic, anaerobic, AFB, fungal); sputum anaerobic culture is often unreliable due to upper airway contamination
- Blood cultures - particularly in immunocompromised or septic patients
- Bronchoscopy - essential role when:
- Failure to respond to treatment
- Suspicion of obstruction (tumor, foreign body)
- Need for protected-brush specimen or BAL for culture
- To facilitate drainage (cautiously)
- Sputum cytology - to exclude malignancy
- Thoracentesis - if pleural effusion present (rule out empyema)
- CBC, ESR, CRP - markers of infection and response to treatment
- HIV testing - in appropriate clinical context
Treatment
1. Antimicrobial Therapy
Empirical therapy must cover strict anaerobes and facultative anaerobic streptococci (Murray & Nadel, Ch. 50):
| First-line options | Rationale |
|---|---|
| Beta-lactam + beta-lactamase inhibitor (amoxicillin-clavulanate, ampicillin-sulbactam, piperacillin-tazobactam) | Broad coverage; preferred first-line |
| Clindamycin (600 mg IV q8h, then 300 mg oral q6h) | Excellent anaerobic coverage; reserved for beta-lactam allergy due to C. difficile risk |
| Carbapenem (e.g., imipenem, meropenem + streptococcal coverage) | For resistant organisms; note meropenem monotherapy lacks streptococcal coverage |
Duration: Typically 4-6 weeks (or longer until cavity resolves). Clinical improvement expected within 3-4 days, defervescence within 7-10 days.
MRSA abscess (post-influenza):
- MSSA: cefazolin, nafcillin, or oxacillin
- MRSA: linezolid (preferred for lung penetration) or vancomycin
- Avoid daptomycin - poor bioavailability in lungs
2. Postural Drainage and Physiotherapy
- Position patient to drain affected segment
- Chest physiotherapy to facilitate expectoration
- Standard conservative management for most abscesses
3. Percutaneous (CT-guided) Catheter Drainage
Indications (Murray & Nadel, Ch. 50):
- Abscesses not communicating with airway (no air-fluid level on imaging)
- Failure of antibiotic therapy
- Abscess > 4 cm (higher failure rate with antibiotics alone)
Technique:
- Seldinger technique with pigtail catheter (12-14 French)
- Position patient with affected side up to prevent spillage to unaffected lung
- Avoid decubitus position with unaffected side dependent
- Success rate ~84% across published series; complication rate ~16%
- Complications: pneumothorax, hemothorax, hemoptysis, catheter clogging, bronchopleural fistula
4. Bronchoscopic Drainage
- Limited role; risk of spilling pus to healthy lung
- Useful for diagnosing/relieving obstruction, sampling for culture
5. Surgical Resection
Indications (Fishman's, p. 2244):
- Failure to respond to antibiotic therapy (no improvement by 7-10 days)
- Large abscesses (> 5-6 cm)
- Ventilation-perfusion scans showing little residual function in necrotic region
- Airway obstruction (tumor, foreign body) limiting drainage
- Rapidly progressive necrotizing infection
- Infarcted lung
- Life-threatening hemoptysis
- Bronchopleural fistula or empyema not responding to drainage
Procedure: Lobectomy (most common), rarely pneumonectomy in extensive disease.
Patients poor surgical risks: Percutaneous drainage as bridge to surgery; avoid if pleural space not protected (risk of catastrophic empyema from abscess contents).
Complications
(Murray & Nadel, Ch. 50; Fishman's, p. 2244)
- Hemoptysis - bronchial arteries supply blood to the abscess wall; may range from minor to massive and life-threatening
- Bronchopleural fistula - abscess erodes into pleural space
- Empyema - spread of infection to pleural cavity; can also occur as surgical complication
- Mediastinitis - rare but life-threatening
- Metastatic abscess - bacteria/infected clots bypass the pulmonary filter to reach systemic circulation:
- Brain abscess: lung abscess/bronchiectasis is associated with brain abscess by adjusted OR of 8.2 (95% CI 3.6-18.5) in population-based studies (Murray & Nadel, Ch. 50)
- Stroke - paradoxical embolism via pulmonary venous drainage
Prognosis and Mortality
(Fishman's, p. 2244; Murray & Nadel, Ch. 50)
- Pre-antibiotic era: mortality 32-34% regardless of treatment modality
- With antibiotics: mortality reduced to 15-20%
- High-risk features carrying mortality up to 75% despite treatment:
- Immunocompromise
- Bronchial obstruction
- Large abscesses (> 6 cm)
- Aerobic organisms (especially K. pneumoniae, S. aureus, P. aeruginosa)
- Advanced age
- Malnutrition / systemic debility
- Major delay in seeking medical attention
- Progressive pulmonary necrosis
Summary Table: Primary vs. Secondary Lung Abscess
| Feature | Primary | Secondary |
|---|---|---|
| Host | Immunocompetent | Immunocompromised / structural lung disease |
| Cause | Aspiration, community-acquired pneumonia | Obstruction, bronchiectasis, hematogenous spread |
| Onset | Subacute (1-3 weeks) | Can be acute (48-72 h for septic emboli) |
| Organisms | Predominantly anaerobes | Mixed; aerobic organisms more common |
| Location | Dependent segments (right upper lobe posterior, lower lobe apical) | Variable |
| Prognosis | Better | Worse |
References: Fishman's Pulmonary Diseases and Disorders, Chapter 127 (pp. 2242-2244); Murray & Nadel's Textbook of Respiratory Medicine, Chapter 50 (pp. 1154-1157)
This is a shared conversation. Sign in to Orris to start your own chat.