Spirometry and lung volume answer for 20 marks
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
I now have all the content needed for a thorough 20-mark answer. Here is the complete, structured response:
Spirometry and Lung Volumes
1. Introduction
Spirometry is the most widely used pulmonary function test. It measures the volume and flow of air that a subject can inhale and exhale, providing objective data to assess lung function in health and disease. The spirometer records these values on a calibrated tracing (spirogram), from which both static lung volumes and dynamic flow measures are derived. - Costanzo Physiology 7th Edition
2. Static Lung Volumes and Capacities
Static lung volumes are measured with a spirometer. The subject breathes into and out of the spirometer, displacing a bell, and the displaced volume is recorded. Four primary volumes and four capacities are defined. - Costanzo Physiology 7th Edition
2.1 The Four Primary Lung Volumes
| Volume | Abbreviation | Normal Value | Description |
|---|---|---|---|
| Tidal Volume | VT | ~500 mL | Volume of air inspired or expired in a normal, quiet breath |
| Inspiratory Reserve Volume | IRV | ~3000 mL | Extra volume that can be inspired above tidal volume with maximal effort |
| Expiratory Reserve Volume | ERV | ~1200 mL | Extra volume that can be expired below tidal volume with maximal effort |
| Residual Volume | RV | ~1200 mL | Volume remaining in the lungs after maximal forced expiration; cannot be measured by spirometry |
Key point: RV cannot be measured by a simple spirometer because it is the air that remains even after full forced expiration.
2.2 The Four Lung Capacities
Each capacity is the sum of two or more volumes:
| Capacity | Abbreviation | Formula | Normal Value | Clinical Note |
|---|---|---|---|---|
| Inspiratory Capacity | IC | VT + IRV | ~3500 mL | Measurable by spirometry |
| Functional Residual Capacity | FRC | ERV + RV | ~2400 mL | Not measurable by spirometry (contains RV) |
| Vital Capacity | VC | IC + ERV (or TLC - RV) | ~4700 mL | Measurable by spirometry |
| Total Lung Capacity | TLC | VC + RV | ~5900 mL | Not measurable by spirometry (contains RV) |
Memory aid: Capacities containing RV (FRC and TLC) cannot be measured by spirometry.
2.3 Factors Affecting Lung Volumes
- Vital capacity increases with body size, male sex, and physical conditioning
- Vital capacity decreases with age
- With aging: RV increases, FRC increases, VC decreases; TLC remains relatively stable - Fishman's Pulmonary Diseases and Disorders
3. Measurement of FRC: Special Methods
Because FRC includes RV, two indirect methods are used:
3.1 Helium Dilution Method
The subject breathes a known amount of helium (which is insoluble in blood) added to the spirometer. After several breaths, helium concentration equilibrates between lungs and spirometer. Using the conservation of helium (C1 × V1 = C2 × [V1 + FRC]), the FRC is back-calculated.
3.2 Body Plethysmography (Plethysmograph)
The subject sits in a large airtight box (plethysmograph). After expiring a normal tidal volume, the mouthpiece is closed. The subject attempts to breathe, and Boyle's Law (P × V = constant) is applied to the changes in box pressure and mouth pressure to calculate FRC. This method measures all gas in the lungs (including trapped gas), making it superior to helium dilution in patients with airway obstruction. - Costanzo Physiology 7th Edition
4. Spirometry: Dynamic Lung Function
4.1 The FVC Maneuver
The Forced Vital Capacity (FVC) is the total volume of air exhaled with maximal force from a point of maximal inhalation (TLC) to the point of maximal exhalation (RV). From the FVC maneuver, two key measures are derived: - Goldman-Cecil Medicine
- FEV1 (Forced Expiratory Volume in 1 second): the volume exhaled in the first second of the FVC maneuver. This is the most standardized single index of airflow obstruction.
- FEV1/FVC ratio: the proportion of vital capacity expelled in the first second. A ratio <70% (below the lower limit of normal) indicates obstructive lung disease.
4.2 Additional Flow Measures
| Parameter | Description | Clinical Use |
|---|---|---|
| FEF25-75% | Mean flow over the middle 50% of the FVC | Sensitive for small airway obstruction |
| PEF | Peak Expiratory Flow | Simple index; useful for monitoring asthma |
| MVV | Maximal Voluntary Ventilation (L/min) | Estimates ventilatory reserve; reduced by central obstruction or muscle weakness |
Note: FEF25-75% has poor reproducibility and many false positives/negatives, limiting its clinical utility on its own. - Murray & Nadel's Textbook of Respiratory Medicine
4.3 Bronchodilator Reversibility Testing
Spirometry is commonly performed before and after an inhaled bronchodilator (e.g., salbutamol). An improvement in FEV1 of >12% and >200 mL indicates reversible airflow obstruction, suggesting asthma rather than COPD. For testing: long-acting beta-2 agonists should be stopped for 12 hours, and short-acting bronchodilators for 6 hours before the test. - Murray & Nadel's Textbook of Respiratory Medicine
5. Spirogram and Flow-Volume Loop
5.1 Volume-Time Tracing (Spirogram)
Plots volume on the y-axis vs. time on the x-axis. FVC is the total height of the curve; FEV1 is read at the 1-second mark.
5.2 Flow-Volume Loop
Plots instantaneous flow (y-axis) vs. lung volume (x-axis) measured by a pneumotachograph. This is more sensitive for identifying the site of airway obstruction:
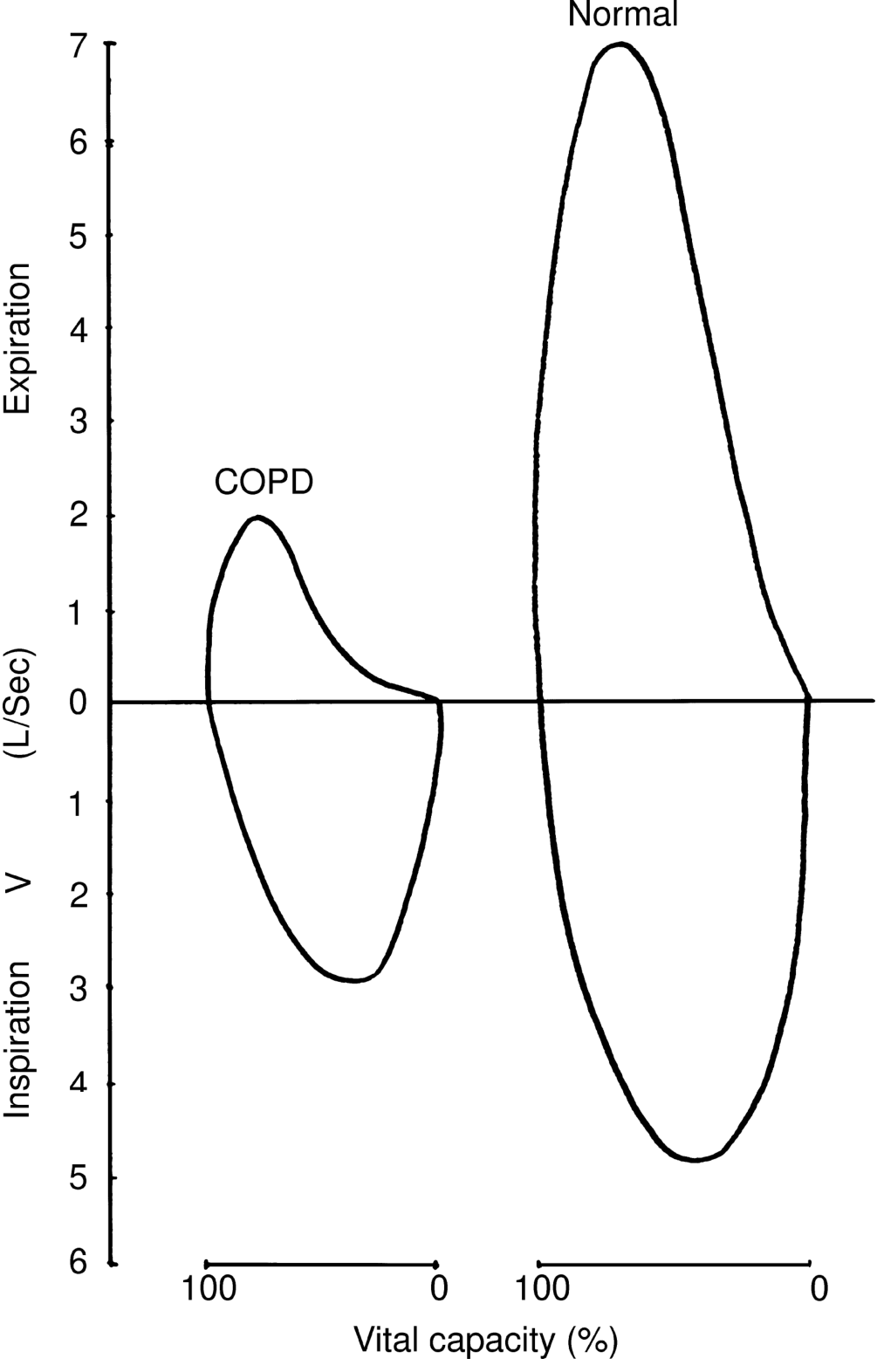
- Normal: Expiratory curve is convex (domed)
- Obstructive (COPD/asthma): Expiratory limb is concave (scooped inward), with reduced peak and mid-expiratory flows
- Restrictive: Loop is smaller but maintains normal shape; FEV1/FVC ratio is normal
- Fixed upper airway obstruction: Both inspiratory and expiratory limbs are flattened (plateau)
- Variable extrathoracic obstruction: Inspiratory limb is flattened
- Variable intrathoracic obstruction: Expiratory limb is flattened
6. Interpretation: Obstructive vs Restrictive Patterns
| Parameter | Obstructive (e.g., COPD, Asthma) | Restrictive (e.g., Fibrosis, Neuromuscular) |
|---|---|---|
| FEV1 | Decreased | Decreased |
| FVC | Normal or decreased | Decreased |
| FEV1/FVC | Decreased (<70%) | Normal or increased |
| TLC | Normal or increased | Decreased |
| RV | Increased (air trapping) | Decreased or normal |
| FRC | Increased | Decreased |
| DLCO | Decreased in emphysema; normal in asthma | Decreased in parenchymal disease |
Causes of Restrictive Pattern - Fishman's Pulmonary Diseases and Disorders
| Disease Process | Anatomic Location | Mechanism |
|---|---|---|
| Pulmonary fibrosis, ILD | Lung parenchyma | Loss/stiffening of lung tissue → reduced volumes |
| Pneumonectomy/lobectomy | Lung parenchyma | Reduced tissue → reduced volumes |
| Pleural effusion, pneumothorax, pleural thickening | Pleura, chest wall | Limited chest expansion |
| Obesity, kyphoscoliosis | Chest wall | Mechanical restriction |
| Neuromuscular disease (MND, myasthenia) | Nerves/muscles | Reduced respiratory muscle force |
Mixed Obstructive-Restrictive Pattern
Some diseases (e.g., severe sarcoidosis, interstitial fibrosis with airway involvement) produce both a low FEV1/FVC ratio and a reduced TLC, reflecting combined obstructive and restrictive physiology. - Fishman's Pulmonary Diseases and Disorders
7. Diffusing Capacity (DLCO)
DLCO measures the transfer of carbon monoxide across the alveolar-capillary membrane and reflects gas exchange efficiency:
| Severity | DLCO (% Predicted) |
|---|---|
| Mild reduction | >60%, but below LLN |
| Moderate reduction | 40-60% |
| Severe reduction | <40% |
- Reduced DLCO: emphysema, interstitial lung disease, pulmonary vascular disease
- Normal or elevated DLCO: asthma (due to increased upper zone perfusion)
- Fishman's Pulmonary Diseases and Disorders
8. Indications for Spirometry - Goldman-Cecil Medicine
- Diagnosis and characterization of respiratory symptoms (dyspnoea, chronic cough, wheeze)
- Monitoring response to therapy (bronchodilators, corticosteroids)
- Objective quantification of physiologic impairment
- Preoperative risk assessment
- Disability evaluation and occupational health screening
- Monitoring drug toxicity (e.g., amiodarone, bleomycin)
9. Normal Values (Summary Table) - Costanzo Physiology 7th Edition
| Parameter | Approximate Normal Value |
|---|---|
| Tidal Volume (VT) | 500 mL |
| IRV | 3000 mL |
| ERV | 1200 mL |
| RV | 1200 mL |
| IC | 3500 mL |
| FRC | 2400 mL |
| VC | 4700 mL |
| TLC | 5900 mL |
| FEV1/FVC | ≥70% |
10. Key Clinical Points
- RV, FRC, and TLC cannot be measured by standard spirometry - they require helium dilution or body plethysmography
- Body plethysmography is preferred over helium dilution in obstructive diseases because trapped gas is included in the measurement
- FEV1 is the single most useful and standardized index of airflow obstruction
- A reversible fall in FEV1 (>12% + 200 mL) after bronchodilator favors asthma; a fixed fall favors COPD
- The flow-volume loop provides additional diagnostic information, especially for upper airway obstruction, beyond what volume-time spirograms can show
- Aging increases RV and FRC, decreases VC, while TLC changes minimally
Gudels stages of anesthesia
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
I have the core textbook content. Now let me compile the complete, detailed answer on Guedel's stages from my knowledge and the textbook sources.
Guedel's Stages of Anesthesia
Historical Background
Arthur E. Guedel (1883-1956) was an American anesthesiologist who first systematically described the four stages of general anesthesia based on his observations of patients receiving inhaled diethyl ether. He also introduced cuffed tracheal tubes and the technique of controlled respiration. His classification remains the foundational framework for understanding depth of anesthesia. - Morgan and Mikhail's Clinical Anesthesiology
Important note: Guedel's classification was derived from ether anesthesia, which has a slow onset and allows clear sequential progression through these stages. With modern intravenous and volatile agents (propofol, sevoflurane, etc.), induction is rapid and Stage II is typically brief or bypassed.
Overview of the Four Stages
Guedel described four stages (or levels) of increasing depth of CNS depression:
| Stage | Name | CNS Level Depressed |
|---|---|---|
| I | Analgesia | Cortex (partial) |
| II | Excitement / Delirium | Cortex (complete) |
| III | Surgical Anesthesia | Subcortical / Spinal cord |
| IV | Medullary Depression | Brainstem / Medulla |
- Katzung's Basic and Clinical Pharmacology, 16th Edition
Stage I - Analgesia
Also called: Induction stage / Amnesia-Analgesia stage
CNS: Cortical depression begins; subcortical centers intact.
Characteristics:
- Patient is conscious and cooperative
- Reduced pain perception (analgesia) - initially without amnesia; later both analgesia and amnesia are present
- Normal reflexes maintained
- Smell, hearing, and touch remain; hearing may actually become hypersensitive
- Breathing: normal, regular
- Pupils: normal size, react to light
- Eye movements: normal, voluntary
Clinical relevance: Minor procedures (e.g., dental analgesia with N₂O) may be performed in Stage I. The patient can respond to verbal commands.
Stage II - Excitement (Delirium)
Also called: Stage of delirium / Induction excitement
CNS: Complete cortical depression with loss of higher inhibitory control; subcortical centers now uninhibited.
Characteristics:
- Patient appears delirious and uncooperative; may vocalize, shout, or cry
- Complete amnesia - patient will have no recollection of this stage
- Irregular, jerky breathing - breath-holding may occur
- Heart rate and blood pressure increase (sympathetic stimulation)
- Reflexes are exaggerated - vomiting, coughing, laryngospasm, and bronchospasm can occur
- Pupils: dilated, active eye movements present
- May show involuntary motor activity; muscle tone increased
- Risk of aspiration is highest in this stage
Clinical relevance: This is the most dangerous stage. The duration and severity of Stage II are deliberately shortened by rapidly increasing the concentration of the anesthetic agent ("crash induction"). Modern practice with rapid IV induction (e.g., propofol) minimizes or bypasses this stage. No surgical procedures should be performed during Stage II.
Stage III - Surgical Anesthesia
Also called: Stage of operative anesthesia
This is the target stage for surgery. It begins with slowing of respiration and heart rate and extends to complete cessation of spontaneous breathing (apnea). Guedel subdivided Stage III into four planes based on progressive depression of reflexes, eye signs, and respiratory patterns.
The Four Planes of Stage III
| Feature | Plane 1 | Plane 2 | Plane 3 | Plane 4 |
|---|---|---|---|---|
| Consciousness | Unconscious | Unconscious | Unconscious | Unconscious |
| Eye movements | Roving/rolling | Roving stops | Fixed, central | Fixed |
| Eyelid reflex | Present | Lost | Lost | Lost |
| Corneal reflex | Present | Present | Lost | Lost |
| Conjunctival reflex | Present | Present | Lost | Lost |
| Light reflex | Present | Present | Present | Lost |
| Pupil size | Normal/slightly miosed | Midsize | Dilating (moderate) | Maximally dilated |
| Lacrimation | Present | Present | Diminished | Absent |
| Respiration | Regular, thoracic | Regular, thoraco-abdominal | Abdominal only (intercostals paralysed) | Diaphragm paralysis → apnea |
| Pharyngeal reflex | Present | Lost | Lost | Lost |
| Laryngeal reflex | Present | Present | Lost | Lost |
| Peritoneal reflex | Present | Present | Present | Lost |
| Muscle tone | Light relaxation | Moderate relaxation | Good relaxation | Complete flaccidity |
| Bleeding | Oozing | Oozing | Moderate | Minimal (vasoconstriction) |
Plane-by-plane summary:
Plane 1 (Light anesthesia):
- Roving eye movements present; eyelid reflex lost
- Swallowing and vomiting reflexes disappear
- Regular, slightly deepened respiration
- Used for: minor, superficial procedures
Plane 2 (Medium anesthesia):
- Eye movements cease; eyes become fixed and central
- Corneal reflex still present; pharyngeal reflex lost
- Regular thoraco-abdominal breathing
- Muscle relaxation adequate for most intra-abdominal surgery
Plane 3 (Deep anesthesia):
- Corneal reflex lost; pupils begin to dilate
- Intercostal muscles paralysed - only diaphragmatic breathing (abdominal breathing)
- Laryngeal reflex lost - risk of aspiration if regurgitation occurs
- Muscle relaxation complete
- Used for: major abdominal surgery, but approaching dangerous depth
Plane 4 (Approaching overdose):
- Diaphragm progressively paralysed → apnea
- Pupils maximally dilated and unresponsive to light
- Complete muscular flaccidity
- Hypotension developing
- Surgery must never be prolonged at this depth
Stage IV - Medullary Depression
Also called: Stage of overdose / Bulbar paralysis
CNS: Depression of the medulla oblongata - the vital centers for respiration and vasomotor control.
Characteristics:
- Cessation of breathing (respiratory arrest)
- Circulatory collapse - profound hypotension, bradycardia progressing to cardiac arrest
- Fixed, maximally dilated pupils - no light reflex
- Complete muscular flaccidity
- Pale/cyanosed patient
Outcome: Without immediate circulatory and respiratory support (CPR, mechanical ventilation), death will rapidly ensue.
Summary Comparison Table
| Feature | Stage I | Stage II | Stage III (Surgical) | Stage IV |
|---|---|---|---|---|
| Consciousness | Conscious | Unconscious | Unconscious | Unconscious |
| Amnesia | Partial → Complete | Complete | Complete | Complete |
| Analgesia | Yes | Yes | Yes | Yes |
| Respiration | Normal | Irregular | Regular → Apnea | Arrested |
| Pupils | Normal | Dilated | Normal → Dilating | Max Dilated |
| Eye reflexes | Normal | Active | Diminishing | Absent |
| Muscle tone | Normal | Increased | Relaxing → Flaccid | Flaccid |
| BP/HR | Normal | Increased | Decreasing | Arrested |
| Vomiting risk | Low | Highest | Low | Absent |
Clinical Relevance of Guedel's Classification Today
- Historical importance: The classification remains the conceptual foundation for understanding depth of anesthesia.
- Modern inhalational agents (isoflurane, sevoflurane, desflurane) produce the same general pattern of CNS depression, though much more rapidly than ether.
- Intravenous induction (propofol, thiopental) bypasses Stage II almost entirely - patients go from Stage I directly into Stage III within seconds.
- Monitoring depth of anesthesia: Modern monitors (BIS - Bispectral Index, entropy monitoring) provide EEG-based depth of anesthesia monitoring, supplementing clinical signs.
- Practical signs still used: Pupil size, eye position, respiratory pattern, lacrimation, and response to stimuli are still assessed clinically.
- Premedication with opioids, benzodiazepines, and anticholinergics aims to smooth the transition through Stage II and reduce secretions and autonomic responses.
Key Points to Remember
- Guedel described 4 stages; Stage III has 4 planes
- Stage II is the most dangerous - vomiting, laryngospasm, aspiration risk
- Stage III Plane 3 is the target for most major surgeries
- Pupil dilation is a critical sign of deepening anesthesia; maximum dilation in Stage IV signals danger
- Respiration becomes abdominal in Stage III Plane 3 as intercostals are paralysed by increasing depth
- Loss of corneal reflex marks transition into Plane 3 - a clinical warning sign
Sources: Katzung's Basic and Clinical Pharmacology 16th Ed; Morgan and Mikhail's Clinical Anesthesiology 7th Ed
This is a shared conversation. Sign in to Orris to start your own chat.