Describe human pappiloma virus and its role in pathogenesis of cervical carcinoma. Give answer as per gynecological oncologist. Give tables, flowchart, images
Reading File
Finding Sources
Finding Sources
Searching PubMed
"human papillomavirus" AND "cervical carcinoma" AND pathogenesis
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Searching the Web
HPV cervical carcinoma pathogenesis FIGO staging 2023 2024 gynecologic oncology
I now have all the information needed for a comprehensive gynecologic oncologist-level answer. Let me compile it.
Human Papillomavirus (HPV) and Its Role in the Pathogenesis of Cervical Carcinoma
As per Gynecological Oncology perspective - Berek & Novak's Gynecology, Robbins Pathology, Goldman-Cecil Medicine, Henry's Clinical Diagnosis
1. HPV: The Virus
Virology and Classification
HPV is an epitheliotropic, double-stranded, circular DNA virus belonging to the Papillomaviridae family, with more than 170 distinct genotypes identified. It targets the stratified squamous epithelium of the anogenital tract and mucous membranes. The viral life cycle is strictly dependent on the cellular differentiation program of the keratinocyte - viral oncogene expression is coordinated with cellular division and stratification.
Genome Organization:
| Gene Class | Genes | Function |
|---|---|---|
| Early (E) genes | E1, E2 | DNA replication, transcription regulation |
| Early (E) genes | E4 | Viral particle maturation |
| Early (E) genes | E6 | Binds/degrades p53 tumor suppressor - KEY ONCOPROTEIN |
| Early (E) genes | E7 | Binds/inactivates Rb (retinoblastoma protein) - KEY ONCOPROTEIN |
| Late (L) genes | L1 | Major capsid protein (target of vaccines) |
| Late (L) genes | L2 | Minor capsid protein |
HPV Risk Classification
| Oncogenic Risk | HPV Genotypes | Clinical Association |
|---|---|---|
| High-risk (HR-HPV) | 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68 | CIN 2/3, HSIL, invasive carcinoma |
| Low-risk (LR-HPV) | 6, 11 | Condylomata acuminata (genital warts), CIN 1/LSIL |
Key Fact: HPV-16 and HPV-18 together account for approximately 70% of all cervical cancers worldwide. HPV-16 predominates in squamous cell carcinoma; HPV-18 has a greater propensity for adenocarcinoma of the endocervix.
- Berek & Novak's Gynecology, p. 842; Henry's Clinical Diagnosis, p. 1844
2. The Anatomical Target: Transformation Zone
The cervical transformation zone (TZ) is the critical site where CIN and invasive cancer arise. It is the area between the original squamocolumnar junction (SCJ) and the physiologically active SCJ.
- At menarche, estrogen stimulates lactobacilli-mediated glycogenolysis, lowering vaginal pH and triggering squamous metaplasia of subcolumnar reserve cells
- Metaplasia advances from the original SCJ inward toward the external os - this process establishes the transformation zone
- CIN typically originates at the advancing SCJ within the transformation zone
- The anterior lip of the cervix is twice as likely to develop CIN as the posterior lip
- Proximally, CIN involves the cervical clefts, which harbor the most severe lesions
Berek & Novak's Gynecology, p. 834
3. Pathogenesis of Cervical Carcinoma - Step-by-Step Flowchart
SEXUAL TRANSMISSION OF HR-HPV (types 16, 18, 31, 33...)
│
▼
INITIAL HPV INFECTION
(Infects basal/parabasal cells of transformation zone)
│
┌─────────┴─────────┐
▼ ▼
VIRAL CLEARANCE PERSISTENT INFECTION
(80-90% of cases) (10-20% - high risk, older age, smokers)
→ No disease → CIN progression
│
▼
EPISOMAL HPV (early infection)
E6 & E7 expressed at low levels
→ Koilocytic changes → CIN 1 / LSIL
│
▼
INTEGRATION INTO HOST GENOME
(disrupts E2 → loss of E6/E7 regulation)
→ Upregulation of E6 and E7 oncoproteins
→ CIN 2/CIN 3 / HSIL
│
┌─────────┴─────────┐
▼ ▼
E7 ONCOPROTEIN E6 ONCOPROTEIN
Binds & inactivates Binds & degrades
Rb protein (pRB) p53 protein
│ │
▼ ▼
Loss of G1 cell Loss of apoptosis &
cycle checkpoint p53-mediated DNA
→ uncontrolled repair checkpoint
proliferation → genomic instability
│
▼
ADDITIONAL MOLECULAR EVENTS:
• Telomerase activation (hTERT)
• Chromosomal alterations (LOH)
• Methylation of TSG promoters
• RAS mutations, PIK3CA mutations
│
▼
CARCINOMA IN SITU (CIS) / CIN 3
│
▼
INVASIVE CERVICAL CARCINOMA
(Squamous cell 75-80% | Adenocarcinoma 15-20%)
Sources: Berek & Novak's Gynecology, p. 842; Robbins Pathology; Henry's Clinical Diagnosis, p. 1844; Goldman-Cecil Medicine, p. 2011
4. Molecular Mechanisms: E6 and E7 Oncoproteins in Detail
E7 Oncoprotein - "The Rb Hijacker"
- Binds preferentially to the underphosphorylated (active) form of pRb
- In normal cells, hypophosphorylated Rb sequesters E2F transcription factors, preventing S-phase entry
- E7-Rb binding releases E2F → cell cycle progression past the G1 checkpoint unchecked
- Result: uncontrolled cellular proliferation
- Paradoxical p16 upregulation occurs as a negative feedback response to E7 activity - this makes p16 immunostaining a useful surrogate marker for HR-HPV infection
E6 Oncoprotein - "The p53 Assassin"
- Binds p53 and recruits ubiquitin ligase E6-AP, targeting p53 for proteasomal degradation
- Abolishes p53-mediated DNA repair checkpoints and apoptosis
- Also activates telomerase (hTERT), conferring replicative immortality
- Epigenetic effects: methylation of tumor suppressor gene promoters (GSPT1, APC, RASSF1)
Viral Integration - The Point of No Return
- In low-grade lesions, HPV exists as episomal (extrachromosomal) circular DNA
- As CIN progresses, HPV DNA integrates into the host genome - disrupting the E2 gene
- Loss of E2 (a transcriptional repressor) leads to upregulated E6/E7 expression
- Integration also causes direct chromosomal instability at insertion sites
- Integration is considered essential for malignant transformation
Henry's Clinical Diagnosis, p. 1844; Goldman-Cecil Medicine, p. 2011
5. Histological Spectrum: CIN Grading
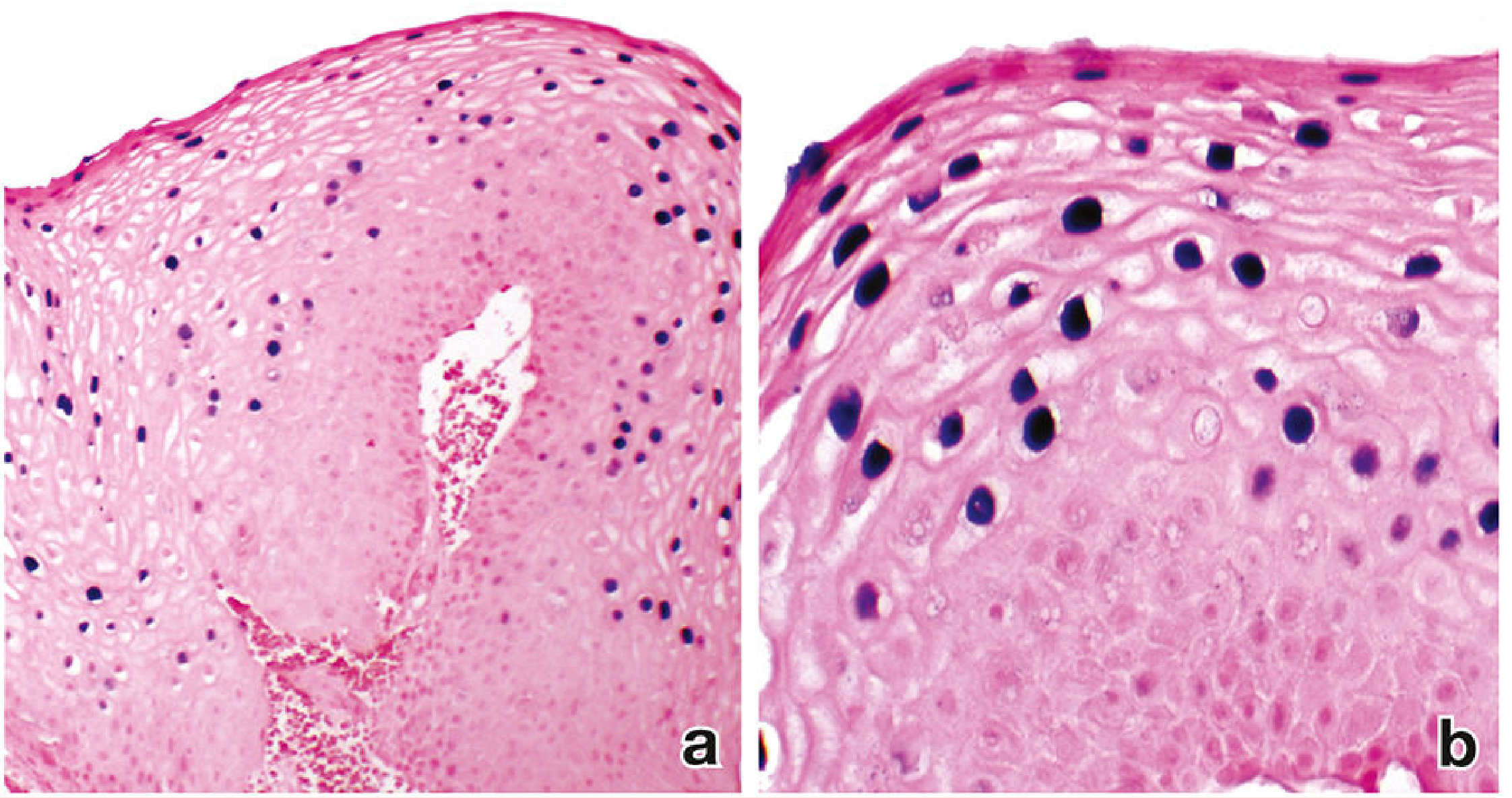
Fig: In situ hybridization of human cervical biopsy showing HPV types 6 and 11. (a) Low magnification showing HPV-infected cells in upper squamous layers. (b) Higher magnification showing viral particles (purple) within nuclei. - Histology: A Text and Atlas
| Grade | Old Term | Bethesda (Cytology) | Histologic Features | HPV Status |
|---|---|---|---|---|
| CIN 1 | Mild dysplasia | LSIL | Cellular changes (koilocytosis) limited to lower 1/3; episomal HPV | High copy episomal HPV; capsid antigen present |
| CIN 2 | Moderate dysplasia | HSIL | Abnormal cells extend to middle 2/3 of epithelium | Integration begins; E6/E7 increasing |
| CIN 3 | Severe dysplasia / CIS | HSIL | Full-thickness atypia; koilocytes disappear; no capsid antigen | Integrated HPV; high E6/E7 expression |
| Invasive Carcinoma | - | - | Breach of basement membrane | Fully integrated HPV |
Koilocyte: Pathognomonic of productive HPV infection - enlarged cell with perinuclear halo (cytoplasmic clearing), well-defined cell borders, nuclear hyperchromasia and irregularity. As lesions become more severe (CIN 2-3), koilocytes disappear because the virus cannot replicate in less-differentiated cells.
Berek & Novak's Gynecology, p. 842
6. Risk Factors for Persistence and Progression
| Risk Factor | Effect |
|---|---|
| HR-HPV type (esp. 16, 18) | Primary determinant - HPV 16 confers 250-fold increased risk of high-grade CIN |
| Persistent infection | Only 5-10% of infections persist; persistence = prerequisite for progression |
| Older age | Decreased immune clearance |
| Smoking | Local immunosuppression, genotoxic effect of tobacco carcinogens on cervix |
| HIV/Immunosuppression | Impaired E6/E7-specific T-cell responses |
| High parity | Repeated cervical trauma, ectropion, prolonged HPV exposure |
| Oral contraceptive use (>5 yrs) | Hormonal promotion of HPV-driven carcinogenesis |
| Co-infection (Chlamydia, HSV-2) | Increased inflammation, mucosal disruption |
| Dietary deficiency (folate, vitamins A, C, E) | Reduced immune competence |
7. Histological Types of Cervical Cancer
| Histological Type | Frequency | HPV Association | Notable Features |
|---|---|---|---|
| Squamous Cell Carcinoma | 75-80% | HPV 16 predominant | Arises at SCJ; keratinizing vs. non-keratinizing subtypes |
| Adenocarcinoma | 15-20% | HPV 18 predominant | Endocervical glands; increasing incidence; harder to detect by cytology |
| Adenosquamous Carcinoma | 3-5% | Both 16 and 18 | Mixed features; aggressive behavior |
| Small Cell Neuroendocrine | <1% | HPV 18 | Very aggressive; early metastasis |
8. Screening - From HPV to Diagnosis
| Age Group | ACOG Recommendation | Rationale |
|---|---|---|
| < 21 years | No screening | High rate of transient HPV infection; treatment harms outweigh benefits |
| 21-29 years | Pap (cytology) every 3 years | Primary HPV testing not recommended - high false positive rate in this age |
| 30-65 years | Primary HPV alone q5 yr, OR co-testing (HPV + Pap) q5 yr, OR Pap alone q3 yr | HPV test has better sensitivity for CIN 2/3 detection |
| >65 years | Discontinue if adequate negative history | 3 negative cytologies OR 2 negative co-tests in prior 10 years |
HPV Test Indications (Gynecologic Oncology Context):
- Triage of ASC-US cytology (reflex HR-HPV testing)
- Co-testing with cytology (ages 30-65)
- Primary HPV screening (ages 25-65 per newer guidelines)
- Sensitivity of conventional Pap: 51%; false-negative rate 49%
- HPV testing has sensitivity >90% for CIN 2+
Berek & Novak's Gynecology, p. 845
9. FIGO Staging 2018 (Current)
| Stage | Description |
|---|---|
| IA | Microscopic invasion only (diagnosed by microscopy) |
| IA1 | Stromal invasion ≤3 mm depth |
| IA2 | Stromal invasion >3 mm and ≤5 mm |
| IB | Visible lesion or microscopic >5 mm, confined to cervix |
| IB1 | Lesion >5 mm and ≤2 cm |
| IB2 | Lesion >2 cm and ≤4 cm |
| IB3 | Lesion >4 cm |
| IIA | Extension beyond uterus, upper 2/3 vagina, no parametrial involvement |
| IIA1 | Lesion ≤4 cm |
| IIA2 | Lesion >4 cm |
| IIB | Parametrial involvement |
| IIIA | Lower 1/3 vagina, no pelvic wall |
| IIIB | Pelvic wall extension or hydronephrosis/non-functioning kidney |
| IIIC1 | Pelvic lymph node metastasis only |
| IIIC2 | Para-aortic lymph node metastasis |
| IVA | Invasion of bladder or rectal mucosa |
| IVB | Distant metastasis |
2018 FIGO Update: Lymph node status (IIIC1/IIIC2) was added for the first time. Imaging (MRI, CT, PET) is now permissible for staging.
10. Vaccination - Primary Prevention
| Vaccine | Genotypes Covered | Target |
|---|---|---|
| Gardasil 9 (current standard) | 6, 11, 16, 18, 31, 33, 45, 52, 58 | Prevents ~90% of HPV-associated cancers |
| Gardasil (original, discontinued) | 6, 11, 16, 18 | - |
| Cervarix (bivalent) | 16, 18 | - |
Key Points:
- Vaccines are prophylactic only - they do not clear existing infection
- Target the L1 capsid protein (virus-like particles)
- Most effective when administered before sexual debut
- Recommended ages 9-26 years for both males and females (ACOG/CDC)
- Catch-up vaccination available up to age 45 with shared decision-making
- E6 and E7 oncoproteins are targets for therapeutic vaccines (investigational)
11. Summary Table: HPV Molecular Carcinogenesis
| Step | Molecular Event | Clinical Correlate |
|---|---|---|
| 1 | HR-HPV infects basal cells of transformation zone | Transient infection, often asymptomatic |
| 2 | Episomal HPV replication, E6/E7 low expression | Koilocytosis, CIN 1 |
| 3 | Persistent infection, immune evasion | Continued cytologic abnormality |
| 4 | HPV integrates into host genome (E2 disrupted) | CIN 2 begins |
| 5 | E6 upregulated → p53 degradation | Loss of apoptosis, DNA repair failure |
| 6 | E7 upregulated → Rb inactivation | Unchecked cell cycle progression |
| 7 | p16 overexpressed (negative feedback) | p16 immunopositivity (diagnostic marker) |
| 8 | Telomerase activation (E6-hTERT) | Replicative immortality |
| 9 | Chromosomal instability, RAS/PIK3CA mutations | CIN 3, carcinoma in situ |
| 10 | Breach of basement membrane | Invasive carcinoma |
12. Key Diagnostic Markers (Gynecologic Pathology)
| Marker | Finding in HPV-Driven CIN/Cancer | Use |
|---|---|---|
| p16 (CDKN2A) | Diffuse strong block-positive staining | Surrogate for HR-HPV E7 activity; confirms CIN 2/3 |
| Ki-67 | High proliferative index | Confirms active cell cycling |
| p53 | Usually wild-type (absent/diffuse) | E6 degrades p53; TP53 mutations rare in HPV+ cancer |
| HPV ISH | Punctate signal (integrated) vs. diffuse (episomal) | Confirms viral integration |
| Pap Cytology | Koilocytes, LSIL, HSIL | Screening |
| HR-HPV DNA testing | Positive in >90% of CIN 2+ | Primary screening, triage |
References (Authoritative Sources):
- Berek & Novak's Gynecology - Chapter 16: Cervical Intraepithelial Neoplasia, pp. 832-858
- Robbins & Cotran Pathologic Basis of Disease - Viral and Bacterial Oncogenesis, p. 184-190
- Goldman-Cecil Medicine - Viral Carcinogenesis, pp. 2011
- Henry's Clinical Diagnosis and Management by Laboratory Methods - Cervical Cancer, p. 1844
- Histology: A Text and Atlas - Clinical Correlation: HPV and Cervical Cancer, p. 2314
This is a shared conversation. Sign in to Orris to start your own chat.