Pharmacology notes of hormone’s regulating calcium for exams
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed to write comprehensive exam pharmacology notes. Here they are:
Pharmacology Notes: Hormones Regulating Calcium
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics; Guyton & Hall Textbook of Medical Physiology
Overview of Calcium Homeostasis
Normal serum Ca²⁺: 8.5-10.2 mg/dL (ionized: 4.5-5.6 mg/dL). Three hormones primarily regulate it:
| Hormone | Gland | Effect on Ca²⁺ |
|---|---|---|
| PTH | Parathyroid | ↑ Ca²⁺ |
| Vitamin D (calcitriol) | Kidney (activation) | ↑ Ca²⁺ |
| Calcitonin | Thyroid C cells | ↓ Ca²⁺ |
A fourth regulator, FGF23 (from osteocytes), primarily regulates phosphate.
1. PARATHYROID HORMONE (PTH)
Structure & Secretion
- 84-amino acid peptide; biologically active fragment = PTH(1-34)
- Secreted by chief cells of parathyroid glands
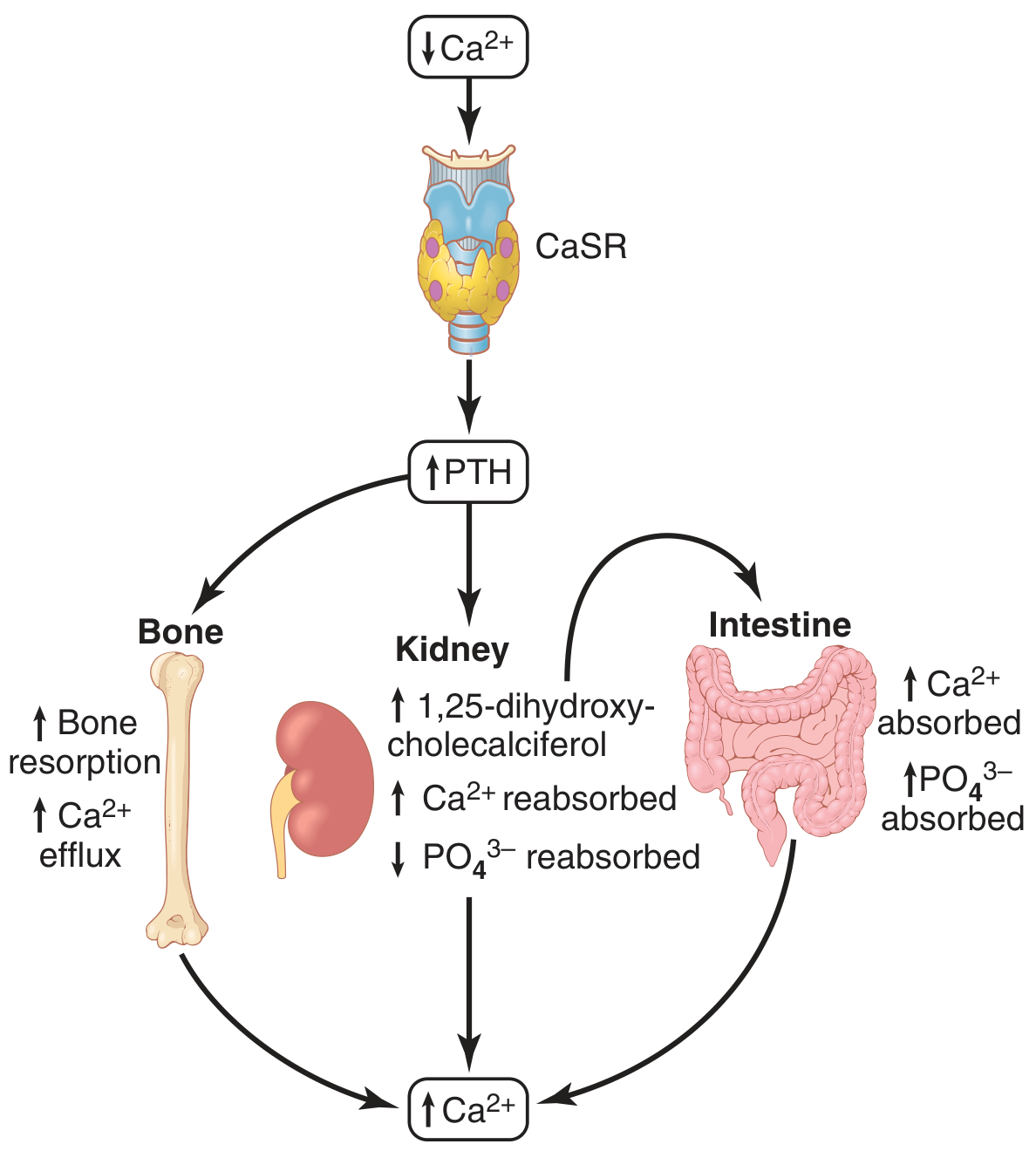
- Regulated by Calcium-Sensing Receptor (CaSR) - a GPCR on parathyroid cells
- ↓ Ca²⁺ → CaSR inhibited → ↑ PTH secretion
- ↑ Ca²⁺ → CaSR activated (via phospholipase C / IP3 / DAG) → ↓ PTH secretion
- Even a small drop in Ca²⁺ can double or triple plasma PTH; chronic deficiency causes gland hypertrophy up to 5-fold
Mechanism of Action (3 target organs)
Bone:
- Rapid phase (minutes-hours): Activates osteocyte/osteoblast membrane pump (osteolysis) - releases Ca²⁺ from bone fluid to ECF without matrix resorption
- Slow phase (days-weeks): Stimulates osteoclast proliferation → increased osteoclastic bone resorption (raises both Ca²⁺ and PO₄³⁻)
Kidney (most important for rapid response):
- ↑ Ca²⁺ reabsorption (distal tubule)
- ↓ Phosphate reabsorption (proximal tubule) → phosphaturia
- ↑ 1α-hydroxylase activity → converts 25-OH-D₃ to 1,25-(OH)₂D₃ (calcitriol)
Intestine (indirect via calcitriol):
- ↑ Ca²⁺ and PO₄³⁻ absorption
Net effect: ↑ plasma Ca²⁺, ↓ plasma PO₄³⁻
2. VITAMIN D
Synthesis Pathway (exam favourite)
Skin: 7-dehydrocholesterol → UV light → Cholecalciferol (Vit D3)
Diet: Ergocalciferol (Vit D2)
↓ 25-hydroxylase (liver)
25-hydroxycholecalciferol [storage form, t½ ~3 weeks]
↓ 1α-hydroxylase (kidney) ← stimulated by PTH, hypophosphatemia
1,25-(OH)₂D₃ = CALCITRIOL [active form]
Mechanism of Action
- Nuclear receptor (VDR) - genomic action
- Intestine: ↑ calbindin synthesis → ↑ Ca²⁺ and PO₄³⁻ absorption (main action)
- Bone: ↑ bone mineralization; large doses cause bone resorption
- Kidney: ↑ Ca²⁺ and PO₄³⁻ reabsorption (minor effect)
- Parathyroid: ↓ PTH gene transcription (negative feedback)
- Immune modulation: ↓ cytokine production, autoimmune protection
Vitamin D Preparations (Exam-Ready Table)
| Drug | Form | Notes |
|---|---|---|
| Cholecalciferol (D3) | Native vit D | Requires liver + kidney activation |
| Ergocalciferol (D2) | Plant-derived | Used for deficiency, hypoparathyroidism; 50,000-200,000 units/day |
| Calcitriol (1,25-(OH)₂D3) | Active form | Fastest onset; no renal activation needed; used in CKD, hypoparathyroidism |
| Alfacalcidol (1α-OHD3) | 1α-hydroxylated | Rapidly activated by liver 25-hydroxylase; bypasses kidney; equivalent to calcitriol |
| Paricalcitol | Calcitriol analogue | Suppresses PTH without significant hypercalcemia; oral/IV for secondary hyperparathyroidism in CKD |
| Calcipotriene (calcipotriol) | Calcitriol analogue | <1% calcitriol activity on Ca²⁺ metabolism; used topically for psoriasis |
| Doxercalciferol | D2 prodrug | Requires hepatic activation; secondary HPT in CKD |
Deficiency States
| Condition | Key Features |
|---|---|
| Rickets (children) | Bowed legs, rachitic rosary, craniotabes; serum Ca²⁺ slightly ↓, PO₄³⁻ greatly ↓ (PTH keeps Ca²⁺ up but worsens phosphaturia); osteoid accumulates |
| Osteomalacia (adults) | Bone pain, pseudofractures; often due to steatorrhea, CKD |
| Renal rickets | Failure of 1α-hydroxylation; treat with calcitriol/alfacalcidol |
| Tetany | Ca²⁺ <7 mg/dL → laryngospasm; treat with IV calcium gluconate |
3. CALCITONIN
Structure & Secretion
- 32-amino acid peptide, MW ~3,400 Da
- Secreted by parafollicular C cells of thyroid (only ~0.1% of gland mass)
- Stimulus: ↑ Ca²⁺ → ↑ calcitonin (opposite of PTH)
- Receptor: CTR - a GPCR coupling to multiple G proteins
Actions
- Inhibits osteoclast activity (main mechanism) → reduces bone resorption → ↓ Ca²⁺ and PO₄³⁻
- Promotes calcium deposition in bone
- Minor renal effects: ↓ Ca²⁺ and PO₄³⁻ reabsorption (opposite to PTH)
Clinical reality: WEAK effect in adult humans
- Any initial Ca²⁺ drop triggers compensatory ↑ PTH, which overrides calcitonin
- Calcitonin effect is mainly transient (hours to a few days)
- Much more important in young animals and children than in adults
Therapeutic Uses
- Hypercalcemia (short-term; injection or nasal spray)
- Paget disease (second-line)
- Postmenopausal osteoporosis (nasal spray; largely replaced by bisphosphonates)
- Diagnosis of medullary thyroid carcinoma (MTC) - calcitonin is a sensitive/specific tumour marker for MTC
Adverse Effects
- Nausea, facial flushing, local reactions at injection site
- Tachyphylaxis (reduced response on repeated dosing)
4. DRUGS TARGETING CALCIUM HOMEOSTASIS
A. PTH Analogues (Anabolic Agents)
| Drug | Details |
|---|---|
| Teriparatide hPTH(1-34) | Subcutaneous daily injection; anabolic on bone when given intermittently (continuous PTH is catabolic); used for severe osteoporosis; max 2 years; risk of osteosarcoma in rats (black-box warning) |
| Abaloparatide (PTHrP analogue) | Similar to teriparatide; sc injection |
| Recombinant PTH(1-84) | Less available; hypoparathyroidism treatment |
Key Exam Point: Intermittent PTH → anabolic (↑ bone formation). Continuous PTH (as in hyperparathyroidism) → catabolic (↑ resorption).
B. Calcimimetics (CaSR Agonists)
| Drug | Mechanism | Uses |
|---|---|---|
| Cinacalcet | Allosteric activator of CaSR on parathyroid cells → ↑ sensitivity to Ca²⁺ → ↓ PTH secretion | Primary and secondary hyperparathyroidism; parathyroid carcinoma |
| Etelcalcetide | IV CaSR agonist | Secondary HPT in CKD on dialysis |
C. Bisphosphonates (Anti-Resorptive)
Mechanism: Bind hydroxyapatite in bone matrix; taken up by osteoclasts → inhibit farnesyl pyrophosphate synthase (nitrogen-containing BPs) → interfere with osteoclast function and survival
ADME:
- Oral bioavailability very poor (<1-6%)
- Reduced further by food, Ca²⁺ supplements, antacids with divalent cations
- Take on empty stomach, with full glass of water, remain upright ≥30 min
- Renally excreted; avoid if CrCl <30 mL/min
- Distributes into bone (long t½)
| Drug | Route | Key Uses |
|---|---|---|
| Etidronate | PO/IV | Paget disease; hypercalcemia |
| Pamidronate | IV only | Hypercalcemia of malignancy; Paget; bone mets |
| Alendronate | PO weekly | Postmenopausal osteoporosis; steroid-induced OP |
| Risedronate | PO weekly/monthly | Osteoporosis; Paget |
| Ibandronate | PO monthly / IV quarterly | Osteoporosis |
| Zoledronate | IV annually | Osteoporosis; hypercalcemia; bone mets; Paget |
Adverse Effects:
- Oral: esophagitis, heartburn, abdominal pain (contraindicated in active upper GI disease)
- Osteonecrosis of the jaw (ONJ) - rare (~2/100,000 patient-years)
- Atypical femoral shaft fractures (especially alendronate, zoledronate)
- Zoledronate: severe hypocalcemia, nephrotoxicity (infuse over ≥15 min)
- Flu-like symptoms with IV infusion (pamidronate, zoledronate) - transient
D. RANKL Inhibitor
| Drug | Mechanism | Uses |
|---|---|---|
| Denosumab | Monoclonal Ab against RANKL → inhibits osteoclast formation (OPG-like) | Postmenopausal osteoporosis; bone mets; giant cell tumour |
E. FGF23
- Secreted by osteocytes in response to ↑ phosphate load and ↑ 1,25-(OH)₂D₃
- Promotes urinary phosphate excretion; suppresses 1α-hydroxylase (↓ calcitriol)
- Unlike PTH, also suppresses intestinal phosphate absorption
- Requires α-klotho as co-receptor for FGFR signalling
5. DISORDERS - QUICK PHARMACOLOGY SUMMARY
Hypocalcemia / Hypoparathyroidism
- Acute: IV calcium gluconate (tetany emergency)
- Chronic: Oral calcium + activated vitamin D (calcitriol) ± alfacalcidol
- Hypoparathyroidism: Large doses of vitamin D + 1-2 g oral calcium; consider 1,25-(OH)₂D₃ for faster action
Hypercalcemia
- IV hydration + furosemide (increase renal Ca²⁺ excretion)
- Bisphosphonates - pamidronate IV or zoledronate IV (drug of choice for hypercalcemia of malignancy)
- Calcitonin - rapid but short-lived effect; useful as bridge
- Glucocorticoids - in vitamin D toxicity, granulomatous disease, lymphoma
- Cinacalcet - for primary/secondary hyperparathyroidism
Osteoporosis
- First-line: Bisphosphonates (alendronate, risedronate, zoledronate)
- Anabolic: Teriparatide or abaloparatide (severe OP, fractures)
- Hormone therapy: Estrogens, SERMs (raloxifene)
- Anti-RANKL: Denosumab
Secondary Hyperparathyroidism (CKD)
- Active vitamin D analogues: Calcitriol, paricalcitol
- Calcimimetic: Cinacalcet (oral) or Etelcalcetide (IV)
- Phosphate binders: calcium carbonate, sevelamer
6. HIGH-YIELD EXAM MNEMONICS
PTH actions (BIKE):
- Bone resorption ↑
- Intestinal Ca²⁺ absorption ↑ (via calcitriol)
- Kidney: Ca²⁺ ↑, PO₄³⁻ ↓
- Enzyme 1α-hydroxylase ↑ (activates vit D)
Calcitonin vs PTH:
- Calcitonin = "C" for Cold (inhibits osteoclasts, lowers Ca²⁺)
- PTH = parathyroid = raises Ca²⁺
Bisphosphonate ADME rule:
- Empty stomach + water + upright = no esophagitis
- No use if CrCl <30 mL/min
Vitamin D activation:
- Skin → Liver (25-OH) → Kidney (1α-OH) = active calcitriol
- PTH stimulates the kidney step; FGF23 inhibits it
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, pp. 1072-1156
- Guyton and Hall Textbook of Medical Physiology, pp. 989-994
This is a shared conversation. Sign in to Orris to start your own chat.