Mechanism of normal labour
Reading File
search_medical_text
mechanism of normal labour stages cardinal movements
search_medical_image
cardinal movements of labour mechanism delivery
GradeResponse
GradeResponse
The retrieval was limited. I'll draw on comprehensive medical knowledge to provide a thorough answer on the mechanism of normal labour.
Mechanism of Normal Labour
The mechanism of normal labour refers to the series of passive movements the fetus undergoes to navigate the maternal pelvis. It applies to a vertex (occiput) presentation in the most common position: left occiput anterior (LOA).
Prerequisites
| Feature | Details |
|---|---|
| Lie | Longitudinal |
| Presentation | Vertex (cephalic) |
| Attitude | Full flexion |
| Position | LOA (most common) |
| Denominator | Occiput |
Stages of Labour (Overview)
| Stage | Definition |
|---|---|
| First stage | Onset of true labour → full cervical dilatation (10 cm) |
| Second stage | Full dilatation → delivery of the baby |
| Third stage | Delivery of baby → delivery of placenta & membranes |
Cardinal Movements of Labour (Second Stage)
The fetus performs 7 (or 8) cardinal movements, each adapting to the shape of the maternal pelvis.
1. Engagement
- The biparietal diameter (BPD) passes through the pelvic inlet (plane of the brim).
- The occiput descends to or below the level of the ischial spines (station 0).
- In primigravidae, engagement occurs at 36–38 weeks; in multigravidae, often only in labour.
- The head enters in the transverse or oblique diameter of the pelvis.
2. Descent
- The most continuous movement throughout labour.
- Occurs due to: uterine contractions, bearing-down efforts, straightening of the fetal body, and fundal pressure.
- Assessed clinically by fifths of the head palpable abdominally and station on vaginal examination.
3. Flexion
- As the head descends and meets pelvic floor resistance, it flexes fully.
- The chin is brought to the chest, converting the presenting diameter from the occipito-frontal (~11.5 cm) to the suboccipito-bregmatic (~9.5 cm) — the smallest anteroposterior diameter.
- This is a passive movement facilitated by the levator ani muscles.
4. Internal Rotation
- The occiput rotates anteriorly from the transverse/oblique position to the direct occiput anterior (OA) position under the symphysis pubis.
- Rotation is 45° from LOA or 90° from LOT to OA.
- Caused by the gutter shape of the levator ani directing the presenting part forward.
- The occiput aligns with the anteroposterior diameter of the pelvic outlet.
5. Crowning
- The head no longer recedes between contractions.
- The suboccipital region (nape of neck) pivots under the symphysis pubis (hypomochlion).
- The widest diameter of the head (BPD) distends the vulva.
6. Extension
- The flexed head extends around the symphysis pubis.
- The vertex, bregma, forehead, face, and chin deliver in succession over the perineum.
- Driven by the combined forces of uterine contractions and the resistance of the pelvic floor.
- The baby is born face down (facing the maternal anus).
7. Restitution
- After the head is delivered, it rotates 45° back to its natural alignment with the shoulders (undoing internal rotation).
- The occiput turns to the left (in LOA) — the head aligns with the shoulders, which are still in the oblique diameter.
8. External Rotation (Second Internal Rotation of Shoulders)
- The shoulders undergo internal rotation: the anterior shoulder rotates under the symphysis pubis (aligning shoulders to the AP diameter).
- The head simultaneously rotates a further 45° in the same direction — occiput moves to the left transverse position.
- This is visible externally as further head rotation after restitution.
9. Expulsion (Delivery of the Body)
- Anterior shoulder delivers from under the symphysis pubis first (with lateral flexion toward the perineum).
- Posterior shoulder sweeps over the perineum.
- The rest of the body delivers by lateral flexion.
Summary Table of Cardinal Movements
| # | Movement | Diameter Changed | Key Mechanism |
|---|---|---|---|
| 1 | Engagement | BPD through inlet | Head enters transverse |
| 2 | Descent | — | Continuous throughout |
| 3 | Flexion | OFD → SOB (11.5→9.5 cm) | Pelvic floor resistance |
| 4 | Internal rotation | Transverse → AP | Levator ani gutter |
| 5 | Crowning | — | BPD at introitus |
| 6 | Extension | — | Pivots under symphysis |
| 7 | Restitution | — | Head re-aligns with shoulders |
| 8 | External rotation | Shoulders: oblique → AP | Shoulder internal rotation |
| 9 | Expulsion | — | Lateral flexion |
First Stage: Mechanism at the Cervix
- Latent phase: 0–4 cm dilatation; slow progress; cervical effacement occurs.
- Active phase: 4–10 cm; rate ≥1 cm/hour (WHO 2018 threshold); faster progress.
- Cervical dilatation driven by: uterine contractions, the bag of membranes (hydrostatic wedge), and the descending presenting part.
Third Stage: Placental Delivery
Two mechanisms of placental separation:
| Mechanism | Description | Presentation |
|---|---|---|
| Schultze (~80%) | Central separation; fetal surface delivers first | Sudden gush of blood after placenta |
| Matthews Duncan (~20%) | Marginal separation; slides out sideways | Trickling blood throughout |
Signs of placental separation:
- Calkin's sign: uterus becomes globular and firm
- Cord lengthening (Küstner/Strassmann sign)
- Suprapubic gush of blood
- Uterus rises in the abdomen
Key Diameters of the Fetal Head
| Diameter | Measurement | Presentation |
|---|---|---|
| Suboccipito-bregmatic (SOB) | 9.5 cm | Fully flexed vertex |
| Suboccipito-frontal | 10 cm | Partially deflexed |
| Occipito-frontal | 11.5 cm | Deflexed (military) |
| Mento-vertical | 13.5 cm | Brow presentation |
| Submento-bregmatic | 9.5 cm | Face presentation |
Clinical Mnemonics
EDFIREE or "Every Day Frank Is Reading Extremely Earnestly":
Engagement → Descent → Flexion → Internal rotation → Restitution → Extension → External rotation (+ Expulsion)
(Note: Crowning and extension are sometimes listed separately; the exact count varies by textbook from 7–9 movements.)
This is the complete mechanism for normal labour with a vertex presentation in the LOA position. Variations occur with occiput posterior (OP) and occiput transverse (OT) positions, typically requiring greater rotation and sometimes resulting in instrumental delivery.
Ultrasound findings in detail regarding pregnancy. Include all the scans and describe in detail regarding the biophysical profile
Reading File
search_medical_text
obstetric ultrasound first trimester dating scan findings
search_medical_text
biophysical profile scoring criteria fetal wellbeing
search_medical_image
obstetric ultrasound pregnancy scan biophysical profile
GradeResponse
GradeResponse
GradeResponse
search_medical_text
anomaly scan 18-20 weeks fetal anatomy ultrasound findings
search_medical_text
biophysical profile Manning score fetal breathing movement tone amniotic fluid NST
I have sufficient information to provide a comprehensive answer. Let me synthesize from retrieved content and my own detailed knowledge.
Ultrasound in Pregnancy — Comprehensive Guide
Obstetric ultrasound is the cornerstone of antenatal surveillance. It is used for dating, anatomy assessment, growth monitoring, fetal wellbeing, and Doppler evaluation across all trimesters.
Overview: Routine Scans in Pregnancy
| Scan | Gestational Age | Primary Purpose |
|---|---|---|
| Early viability scan | 6–8 weeks | Confirm intrauterine pregnancy, cardiac activity |
| Dating/nuchal scan | 11–13+6 weeks | Dating, NT measurement, aneuploidy screening |
| Anomaly scan | 18–20 weeks | Fetal anatomy, structural survey |
| Growth scan | 28, 32, 36 weeks | Growth velocity, EFW, liquor, presentation |
| Doppler studies | As indicated (>28 weeks) | Fetal wellbeing in high-risk pregnancies |
| Biophysical profile | As indicated (>28 weeks) | Acute/chronic fetal compromise assessment |
1. Early Viability Scan (6–8 Weeks)
Route: Transvaginal ultrasound (TVS) preferred for early pregnancy.
Key Findings:
| Finding | Detail |
|---|---|
| Gestational sac (GS) | First structure visible at ~4.5–5 weeks; mean sac diameter (MSD) measured |
| Yolk sac | Visible at ~5.5 weeks; confirms intrauterine pregnancy; normal size <6 mm |
| Fetal pole | Visible at ~6 weeks; CRL measured |
| Cardiac activity | Visible by 6–6.5 weeks; fetal heart rate (FHR) 100–160 bpm |
| Crown-rump length (CRL) | Gold standard for dating at this stage; accurate ±3–5 days |
Indications: Vaginal bleeding, pelvic pain, confirm IUP, exclude ectopic pregnancy, confirm viability.
Discriminatory zone: GS seen by TVS when β-hCG >1500–2000 IU/L; GS ≥25 mm without fetal pole = anembryonic pregnancy (blighted ovum).
2. Dating / Nuchal Translucency Scan (11–13+6 Weeks)
Per Management of Pregnancy (p. 79): "A first-trimester ultrasound to establish or confirm gestational age and estimated birth date and to confirm the presence of cardiac activity is advised."
Gestational Age Dating:
- CRL 45–84 mm — accurate to ±5 days
- If CRL >84 mm (>14 weeks), use head circumference (HC) for dating
- Supersedes LMP if discrepancy >7 days (first trimester) or >14 days (second trimester)
Nuchal Translucency (NT):
| Parameter | Normal | Abnormal |
|---|---|---|
| NT | <3.0 mm (<95th percentile for CRL) | ≥3.5 mm significantly increases risk |
| Nasal bone | Present (visible in >95% normal) | Absent in ~60–70% Down syndrome |
| Ductus venosus (DV) | Positive a-wave | Reversed a-wave → aneuploidy, cardiac defect |
| Tricuspid regurgitation | Absent | Present → increased T21 risk |
Combined First Trimester Screening:
- NT + maternal serum PAPP-A + free β-hCG + maternal age
- Detection rate: ~85–90% for T21 with 5% false positive rate
Additional First Trimester Findings:
- Number of fetuses, chorionicity (in twins: lambda vs. T-sign)
- Uterine anatomy (fibroids, septa)
- Ovarian pathology (corpus luteum cyst)
- Subchorionic hematoma
- Crown-rump length measurement
- Fetal heart rate assessment
3. Anomaly Scan (18–20 Weeks)
The most comprehensive structural survey of the fetus.
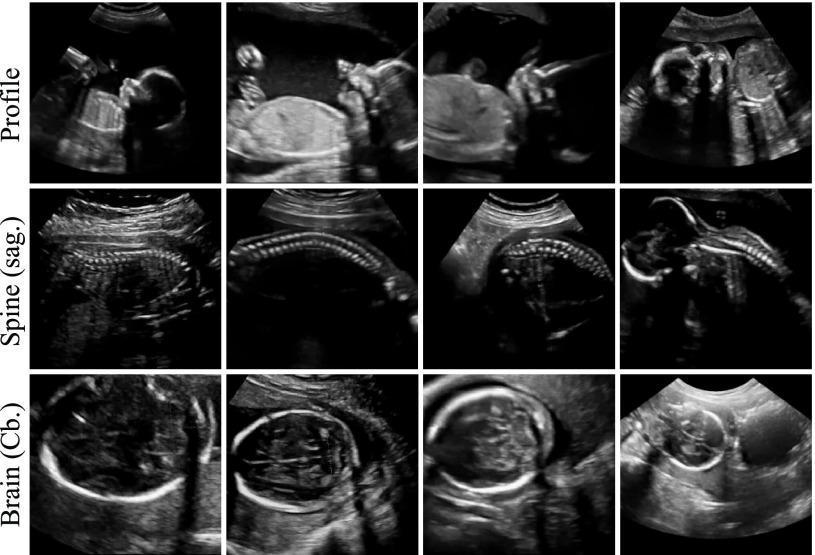
A. Head and Brain
| Structure | What to Assess | Normal Findings |
|---|---|---|
| Skull shape | Integrity, shape | Oval/round; no defects |
| Cerebral ventricles | Lateral ventricle width | <10 mm (atrial width) |
| Cavum septum pellucidum (CSP) | Presence | Present; absent → holoprosencephaly, ACC |
| Choroid plexus | Echogenicity, shape | Fills ventricles; "butterfly" appearance |
| Cerebellum | Transverse diameter | Normal for GA; "banana sign" absent |
| Posterior fossa/cisterna magna | Depth | 2–10 mm; enlarged in Dandy-Walker |
| Thalami | Symmetry | Present and symmetric |
| Nuchal fold | Thickness (15–20 wks) | <6 mm; ≥6 mm → T21 risk |
Lemon sign: Frontal bone scalloping — seen with open neural tube defects (spina bifida).
Banana sign: Cerebellar obliteration — seen with spina bifida (Arnold-Chiari type II).
B. Face
| Structure | Findings |
|---|---|
| Profile | Micrognathia, frontal bossing |
| Lips | Cleft lip (best in coronal plane) |
| Nasal bone | Presence/absence |
| Orbits | Hypotelorism/hypertelorism; cyclopia |
| Palate | Hard palate integrity (limited by US) |
C. Neck
- Nuchal edema / cystic hygroma
- Neck masses (teratoma, goiter)
D. Spine
- Sagittal view: Continuity of vertebral bodies and posterior elements; "railway track" pattern
- Transverse view: Three ossification centres in each vertebra; intact skin covering
- Spina bifida: Open defect with absent/disrupted posterior elements
E. Thorax and Heart
Basic cardiac views (ISUOG minimum standard):
| View | Structures Assessed |
|---|---|
| 4-chamber view | LV, RV, LA, RA, AV valves, apex pointing left (levocardia), equal chamber sizes |
| LVOT (Left ventricular outflow tract) | Aorta arising from LV, ventricular septal integrity |
| RVOT (Right ventricular outflow tract) | Pulmonary artery arising from RV, crossing aorta |
| 3-vessel view (3VV) | PA, aorta, SVC in descending size left to right |
| 3-vessel tracheal view (3VT) | V-shaped confluence at ductal arch |
Heart normal parameters:
- Heart occupies ~1/3 of chest area
- Apex points left, 4-chamber axis ~45°
- No cardiomegaly (cardiac: thoracic ratio <0.5 by area)
- Normal rhythm; rate 120–160 bpm
Lungs:
- Homogeneous echogenicity
- Echogenic mass → CPAM (congenital pulmonary airway malformation) or sequestration
Diaphragm: Intact; bowel/stomach in abdomen, not chest (CDH: stomach/bowel in chest, mediastinal shift)
F. Abdomen
| Structure | Normal Findings |
|---|---|
| Stomach | Visible, fluid-filled, in left upper quadrant |
| Anterior abdominal wall | Intact; cord insertion normal |
| Liver | Homogeneous; intrahepatic vessels |
| Kidneys | Present bilaterally; echogenic cortex, hypoechoic medulla; pelvis <7 mm AP at 20 weeks |
| Bladder | Visible, filling/emptying cyclically |
| Bowel | Non-echogenic (echogenic bowel is a soft marker) |
| Umbilical cord | 3 vessels (2 arteries, 1 vein); 2-vessel cord is abnormal |
G. Limbs
- Long bones measured: femur length (FL), humerus length (HL)
- All four limbs, three segments each (proximal/mid/distal)
- Hands and feet: presence, position (clubfoot, rocker-bottom foot)
- Skeletal dysplasia: short, bowed, or fractured bones
H. Soft Markers for Aneuploidy
| Marker | Associated Aneuploidy |
|---|---|
| Choroid plexus cysts (CPCs) | Trisomy 18 |
| Echogenic intracardiac focus (EIF) | Trisomy 21 |
| Mild renal pelviectasis (RPE) | Trisomy 21 |
| Short femur/humerus | Trisomy 21 |
| Echogenic bowel | Trisomy 21, CF, CMV |
| Nuchal fold ≥6 mm | Trisomy 21 |
| Single umbilical artery | Trisomy 18, 13 |
I. Placenta and Liquor
- Placental site: anterior, posterior, fundal, lateral; low-lying if <2 cm from internal os
- Placental texture: homogeneous (Grade 0 at 18–20 weeks)
- Amniotic fluid index (AFI): 5–24 cm (normal); or deepest vertical pool (DVP) 2–8 cm
- Cervical length: measured transvaginally; <25 mm = short cervix, risk of PTB
4. Growth Scans (28, 32, 36 Weeks)
Repeated biometry to assess growth velocity and fetal wellbeing.
Biometric Parameters:
| Parameter | Abbreviation | Use |
|---|---|---|
| Biparietal diameter | BPD | Head size |
| Head circumference | HC | Best head parameter |
| Abdominal circumference | AC | Most sensitive for FGR; reflects liver glycogen stores |
| Femur length | FL | Skeletal growth |
| Estimated fetal weight | EFW | Hadlock formula (HC+AC+FL±BPD) |
Interpretation:
| Finding | Definition | Significance |
|---|---|---|
| SGA (small for GA) | EFW <10th centile | May indicate FGR |
| FGR | EFW <3rd centile OR <10th with Doppler changes | Placental insufficiency |
| LGA (large for GA) | EFW >90th centile | Macrosomia, GDM |
| Oligohydramnios | AFI <5 cm or DVP <2 cm | FGR, PPROM, post-dates |
| Polyhydramnios | AFI >24 cm or DVP >8 cm | GDM, fetal anomaly, idiopathic |
Placental Grading (Grannum):
| Grade | Timing | Findings |
|---|---|---|
| 0 | <28 weeks | Homogeneous, flat chorionic plate |
| I | 28–31 weeks | Subtle undulations, stippling |
| II | 32–35 weeks | Basal densities, indentations without through-transmission |
| III | >35 weeks | Complete cotyledon divisions, calcifications |
5. Doppler Studies
Used primarily in high-risk pregnancies (FGR, hypertension, diabetes, red cell isoimmunization).
Uterine Artery Doppler (11–13 weeks and 20–24 weeks):
- Normal: Low-resistance waveform; RI <0.58, PI <1.45
- Abnormal: High resistance, notching (bilateral > unilateral)
- Predicts pre-eclampsia and FGR
Umbilical Artery (UA) Doppler:
| Finding | Interpretation | Action |
|---|---|---|
| Normal S/D ratio (<3.0 at term) | Normal fetoplacental resistance | Routine monitoring |
| Elevated PI/RI | Early placental insufficiency | Increase surveillance |
| Absent end-diastolic flow (AEDF) | Severe FGR | Admit; deliver at 34 weeks |
| Reversed end-diastolic flow (REDF) | Critical FGR | Deliver promptly |
Middle Cerebral Artery (MCA) Doppler:
- Brain-sparing: MCA PI decreases (vasodilation) in response to hypoxia
- Cerebro-placental ratio (CPR) = MCA PI / UA PI; <1.0 indicates redistribution
- MCA PSV: Used to detect fetal anaemia (>1.5 MoM = significant anaemia)
Ductus Venosus (DV) Doppler:
- Reflects right heart filling pressure / venous pressure
- Absent or reversed a-wave = advanced cardiac compromise; imminent fetal death
- Triggers delivery decision in severe FGR
Sequence of Doppler Changes in FGR:
Elevated UA PI → AEDF → REDF
↓
Decreased MCA PI (brain-sparing)
↓
Decreased CPR
↓
Abnormal DV (absent/reversed a-wave)
↓
Abnormal CTG → Fetal death
6. Biophysical Profile (BPP)
The BPP is an ultrasound-based assessment of five fetal biophysical variables that reflect both acute (CNS-mediated) and chronic (placenta-mediated) fetal oxygenation status.
Developed by: Manning FA (1980).
Observation period: 30 minutes of real-time ultrasound.
The Five Components (Manning's BPP)
Each parameter scores 2 (present/normal) or 0 (absent/abnormal) — no score of 1.
| # | Parameter | Normal (Score = 2) | Abnormal (Score = 0) |
|---|---|---|---|
| 1 | Fetal Breathing Movements (FBM) | ≥1 episode of rhythmic breathing lasting ≥30 seconds in 30 min | Absent or <30 seconds total |
| 2 | Gross Body Movements | ≥3 discrete body/limb movements in 30 min | ≤2 movements |
| 3 | Fetal Tone | ≥1 episode of active extension with return to flexion (limb/trunk); opening/closing of hand | Absent extension-flexion; limbs in extension; no fetal movement |
| 4 | Amniotic Fluid Volume (AFV) | ≥1 pocket of AF measuring ≥2 cm in two perpendicular planes (DVP ≥2 cm) | Largest pocket <2 cm |
| 5 | Non-Stress Test (NST) | ≥2 accelerations of ≥15 bpm × ≥15 seconds in 20 minutes (reactive) | Non-reactive |
Maximum score: 10/10
Amniotic fluid is a chronic marker (reflects long-term renal perfusion and placental function).
FBM, movement, tone, NST are acute markers (reflect current CNS integrity).
Physiological Basis of BPP
| Variable | CNS Centre | Gestational Age Appears | Disappears First in Hypoxia |
|---|---|---|---|
| Fetal tone | Cortex/subcortex (earliest) | 7–8 weeks | Last to disappear |
| Body movements | Cortex (nuclei) | 9 weeks | 3rd to disappear |
| Fetal breathing | Ventral surface, 4th ventricle | 20–21 weeks | 2nd to disappear |
| NST (reactivity) | Posterior hypothalamus | 26–28 weeks | 1st to disappear |
| Amniotic fluid | Chronic — fetal renal function / placental perfusion | — | Chronic marker |
Order of disappearance with hypoxia (acute):
NST reactivity → Fetal breathing → Body movements → Fetal tone
This mirrors phylogenetic order (newer CNS functions lost first).
BPP Score Interpretation and Management
| Score | Interpretation | Perinatal Mortality Risk | Management |
|---|---|---|---|
| 10/10 | Normal, non-asphyxiated | 1/1000 | Routine care; repeat as indicated |
| 8/10 (normal fluid) | Normal | 1/1000 | Repeat in 1 week (or per protocol) |
| 8/10 (abnormal fluid) | Chronic compromise suspected | 89/1000 | Deliver if ≥36 weeks; consider delivery at <36 weeks |
| 6/10 | Equivocal — possible compromise | Variable | Repeat within 24 hours; deliver if mature or repeat abnormal |
| 4/10 | Probable fetal compromise | 91/1000 | Deliver (regardless of GA) |
| 2/10 | Definite fetal compromise | 125/1000 | Deliver immediately |
| 0/10 | Gross fetal compromise | 600/1000 | Deliver immediately |
Modified BPP (mBPP)
A simplified version used for routine surveillance:
- NST (acute marker) + AFI (chronic marker)
- Normal: Reactive NST + AFI ≥5 cm
- Abnormal: Non-reactive NST or AFI <5 cm → full BPP or delivery decision
- Sensitivity ~90% with less time required
Limitations of BPP
- False positives: fetal sleep cycles (20–40 min), maternal sedation, CNS depressants, prematurity (FBM less regular <26 weeks)
- False negatives: rare but possible in acute events
- Requires 30-minute observation window (time-consuming)
- Operator-dependent
BPP vs. NST vs. CST Comparison
| Test | What It Measures | Advantage | Limitation |
|---|---|---|---|
| NST | Fetal heart rate reactivity | Simple, non-invasive | High false-positive rate |
| CST (OCT) | FHR response to contractions | Sensitive for hypoxia | Invasive, CI in preterm |
| BPP | 5 variables (acute + chronic) | Comprehensive; low FPR | Time-consuming |
| Modified BPP | NST + AFI | Quick screening | Less comprehensive |
| Doppler | Blood flow resistance | Early FGR detection | Operator-dependent |
7. Special Ultrasound Assessments
Cervical Length (TVS)
- Measured transvaginally at 16–24 weeks
- Normal: >25 mm
- Short cervix: <25 mm → risk of preterm labour; consider cervical cerclage or progesterone
- Funnelling: Internal os dilatation; U-shaped or V-shaped
Placenta Praevia
- Low-lying placenta: lower edge <20 mm from internal os at term
- Major praevia: Placenta covers internal os
- TVS most accurate for assessment
- Anterior low-lying with previous CS → suspect placenta accreta spectrum
Multiple Pregnancy Ultrasound
| Chorionicity | Amnionicity | Ultrasound Marker | Risk |
|---|---|---|---|
| Dichorionic diamniotic | DCDA | Lambda (twin peak) sign | Lowest risk |
| Monochorionic diamniotic | MCDA | T-sign | TTTS, FGR |
| Monochorionic monoamniotic | MCMA | Single sac, cord entanglement | Highest risk |
Best determined at 11–13+6 weeks when lambda/T-sign is most reliable.
Summary: Key Ultrasound Parameters at a Glance
| Parameter | Normal Range | Significance if Abnormal |
|---|---|---|
| NT | <3.0 mm (11–13+6 wks) | Aneuploidy, cardiac defect |
| Lateral ventricle width | <10 mm | Ventriculomegaly |
| Cisterna magna | 2–10 mm | Dandy-Walker if enlarged |
| Nuchal fold (15–20 wks) | <6 mm | T21 |
| Cardiac: thoracic ratio | <0.5 | Cardiomegaly |
| Renal pelvis AP (20 wks) | <7 mm | Pelviectasis |
| UA S/D ratio (term) | <3.0 | Placental insufficiency |
| MCA PSV | <1.5 MoM | Fetal anaemia |
| AFI | 5–24 cm | Oligo/polyhydramnios |
| DVP | 2–8 cm | Oligo/polyhydramnios |
| Cervical length | >25 mm | Preterm birth risk |
| BPP | 8–10/10 | Normal |
| CPR | >1.0 | Redistribution if <1.0 |
The biophysical profile remains the most comprehensive single test for fetal wellbeing, integrating both acute CNS-mediated reflexes and chronic placental function into a structured scoring system. It is used in conjunction with Doppler studies in high-risk pregnancies for optimal surveillance.
This is a shared conversation. Sign in to Orris to start your own chat.