Placental site trophoblastic tumor detailed description from standard text books and recent articles and guidelines in post graduate level
Reading File
Finding Sources
Finding Sources
Searching PubMed
"placental site trophoblastic tumor" management treatment
Reading File
Reading File
Reading File
Reading Article
PMID: 39322463
Reading File
Reading File
Reading File
Reading Article
PMID: 40631439
Loading Image
Finding Sources
Reading Article
PMID: 37198729
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Finding Sources
I now have comprehensive material from multiple authoritative textbooks and recent publications. Let me compile the full postgraduate-level response.
Placental Site Trophoblastic Tumor (PSTT) - Postgraduate Level Review
1. Introduction and Classification
Placental site trophoblastic tumor (PSTT) is one of the rarest forms of gestational trophoblastic disease (GTD), representing less than 2% of all gestational trophoblastic neoplasms (GTN). It belongs to the category of intermediate trophoblastic tumors (ITT), along with its close relative, epithelioid trophoblastic tumor (ETT).
GTD spans a spectrum from benign (hydatidiform moles) to malignant neoplasia (GTN). Within GTN, the entities are:
- Invasive mole
- Gestational choriocarcinoma
- Placental site trophoblastic tumor (PSTT)
- Epithelioid trophoblastic tumor (ETT)
Berek & Novak's Gynecology, p. 2492-2508 | Robbins & Kumar Basic Pathology, p. 620
2. Cell of Origin and Biology
PSTT arises from extravillous (intermediate) trophoblasts - cells that normally proliferate from the cytotrophoblast of the anchoring villi, migrate into maternal decidua and myometrium, and remodel spiral arteries. These intermediate trophoblasts have features overlapping between cytotrophoblasts and syncytiotrophoblasts, but are morphologically and functionally distinct.
Key biological characteristics:
- Diploid tumor, usually with XX karyotype
- Intermediate trophoblasts produce human placental lactogen (hPL) as their dominant secretory product, rather than hCG
- hCG production is minimal - serum hCG levels are disproportionately low relative to tumor burden (a defining clinical feature)
- Cells exhibit vascular tropism - they invade along vessel walls and replace endothelium, a pattern called "endovascular trophoblast invasion"
- Unlike choriocarcinoma, PSTT invades without causing the overt hemorrhage and necrosis typical of choriocarcinoma
Robbins & Kumar Basic Pathology, p. 620 | Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 958
3. Epidemiology
- Incidence: <2% of all GTN
- Can follow any type of gestation: normal term pregnancy (~50% of cases), spontaneous abortion, or hydatidiform mole
- Usually presents weeks to months (sometimes years) after the antecedent pregnancy - the interval from last pregnancy is clinically significant (see Prognosis section)
- No specific geographic or racial predilection documented
4. Clinical Presentation
| Feature | Details |
|---|---|
| Abnormal uterine bleeding | Most common presentation - irregular or heavy |
| Amenorrhea | Occurs in a subset |
| Uterine mass | Detectable on imaging |
| hCG elevation | Low-level or minimally elevated (unlike choriocarcinoma) |
| hPL elevation | More reliable marker than hCG |
| Virilization | Rare - from androgen secretion |
| Nephrotic syndrome | Rare paraneoplastic |
The tumor is usually confined to the uterus at presentation, with late metastasis. This is in contrast to choriocarcinoma, which metastasizes early and hematogenously.
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 958
5. Pathology
5.1 Gross Appearance
PSTT appears as a uterine mass, often soft and hemorrhagic but without the extreme necrosis seen in choriocarcinoma. The tumor may be polypoid within the endometrial cavity, myometrial, or rarely diffusely infiltrating.
5.2 Histopathology
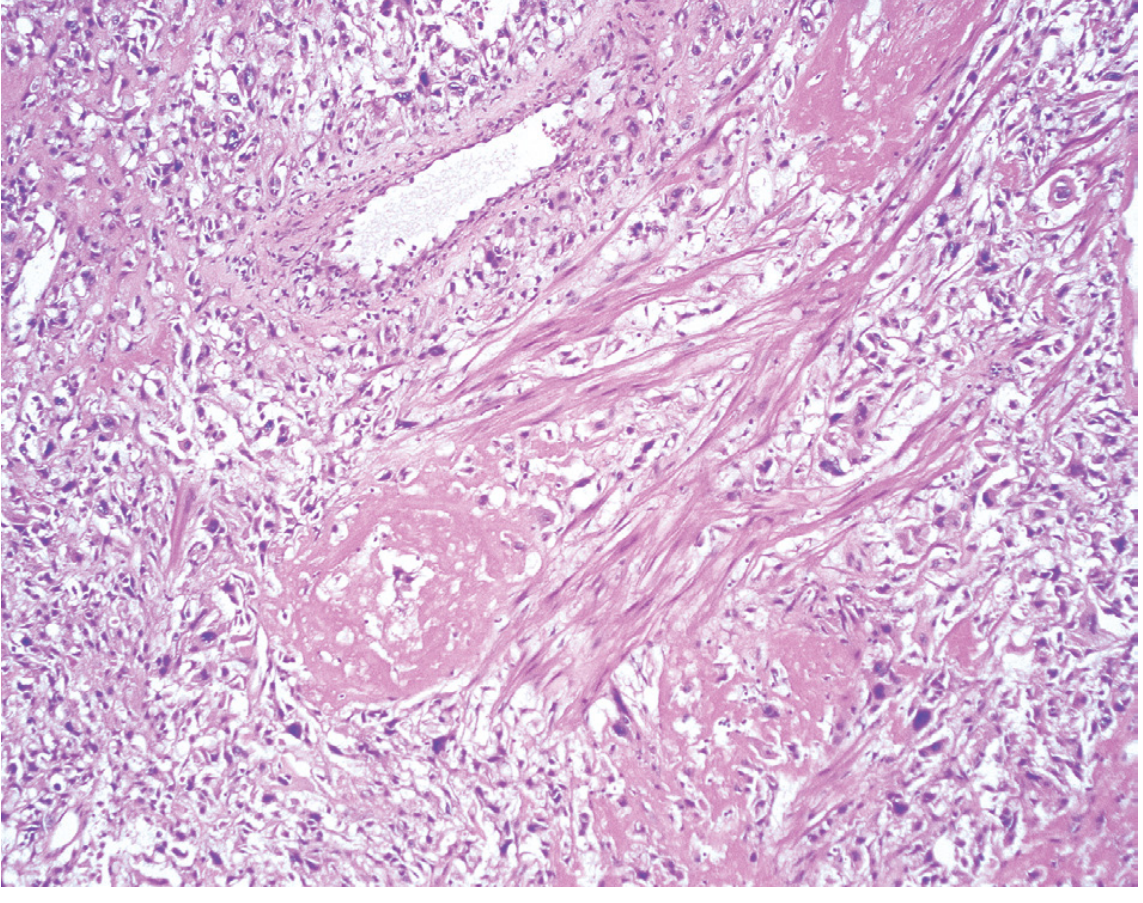
Key histologic features:
- Polygonal mononuclear or binucleated cells with abundant eosinophilic cytoplasm
- Cells infiltrate between smooth muscle fibers of the myometrium, splaying them apart (characteristic pattern) without destroying them
- Vascular invasion - tumor cells show striking tropism for uterine vessels, replacing the vessel wall endothelium (fibrinoid material deposited)
- No chorionic villi (differentiates from molar disease)
- No biphasic pattern of cytotrophoblasts and syncytiotrophoblasts (differentiates from choriocarcinoma)
- Mitotic figures present but variable (low mitotic index favors benign behavior)
- Necrosis may be present but less extensive than choriocarcinoma
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 957-958
5.3 Immunohistochemistry (IHC) - Critical for Diagnosis
| Marker | PSTT | Choriocarcinoma | ETT |
|---|---|---|---|
| hPL | Strongly + | Focal + | Focal + |
| hCG | Weakly/focally + | Strongly + | Weakly + |
| Cytokeratin | + | + | + |
| CD146 (Mel-CAM) | + | - | - |
| HLA-G | + | - | - |
| p63 | - | - | Strongly + (ETT marker) |
| Ki-67 | Variable | High | Low-moderate |
hPL immunostaining is the most useful confirmatory marker for PSTT. CD146 and HLA-G (markers of extravillous trophoblast) are helpful for distinguishing PSTT from ETT and choriocarcinoma.
6. FIGO Staging
PSTT is staged using the FIGO anatomical staging system for GTN:
| Stage | Definition |
|---|---|
| Stage I | Confined to the uterus |
| Stage II | Extends to genital structures (adnexa, vagina, broad ligament) |
| Stage III | Lung metastases (with/without genital tract involvement) |
| Stage IV | Other distant metastases (brain, liver, spleen, kidney, GI tract) |
Important: Unlike other GTN, the WHO/FIGO prognostic scoring system does NOT apply to PSTT and ETT. The standard risk-scoring system (which drives single-agent vs. multi-agent chemotherapy decisions in other GTN) is not used for PSTT.
Berek & Novak's Gynecology, p. 2508 | [Wang et al., Hematol Oncol Clin North Am, 2024 - PMID 39322463]
7. Diagnostic Workup
Serum markers:
- Beta-hCG (low or mildly elevated; if hCG is very high, reconsider diagnosis)
- hPL (more specific for PSTT)
- Free beta-hCG subunit
Imaging:
- Pelvic ultrasound with Doppler - uterine mass with variable vascularity
- MRI pelvis - preferred for local staging and myometrial invasion assessment
- CT chest/abdomen/pelvis - staging workup
- PET-CT - increasingly used for equivocal cases
Histology - Definitive diagnosis requires tissue. Curettage specimens may be sufficient, but hysterectomy specimen provides complete assessment.
8. Management
8.1 Surgery - Cornerstone of Treatment
Hysterectomy is the primary and definitive treatment for PSTT, including for Stage I disease. This is the most important distinction from other GTN (which are predominantly managed with chemotherapy).
Rationale for hysterectomy:
- PSTT is relatively chemoresistant compared to other GTN
- Most cases are confined to the uterus at presentation
- Surgical removal provides cure in the majority of Stage I cases
Lymphadenectomy: Pelvic/para-aortic lymphadenectomy should be considered as PSTT can metastasize via lymphatics (unlike choriocarcinoma, which is predominantly hematogenous).
Fertility-sparing surgery: Case reports support local resection/uterine curettage for young patients with disease strictly confined to the uterine cavity, followed by close hCG and hPL surveillance. However, this remains non-standard and should only be considered in specialized centers.
Schwartz's Principles of Surgery, p. [section on GTD] | Berek & Novak's Gynecology, p. 2508
8.2 Chemotherapy
Unlike other GTN, standard WHO risk-stratification does not guide chemotherapy in PSTT. Chemotherapy is indicated for:
- Metastatic disease (Stages II-IV)
- High-risk features: interval >48 months from antecedent pregnancy, advanced stage, deep myometrial invasion, high mitotic index, or necrosis
Preferred regimens:
- EMA-EP (Etoposide, Methotrexate, Actinomycin-D - Etoposide, Cisplatin) - preferred for PSTT
- EMA-CO (Etoposide, Methotrexate, Actinomycin-D - Cyclophosphamide, Vincristine/Oncovin) - less preferred for PSTT given relative resistance
EMA-EP is preferred over EMA-CO for PSTT/ETT because the cisplatin component appears to have greater activity in intermediate trophoblastic tumors. Per Berek & Novak: patients resistant to EMA-CO can achieve remission in up to 76% with EMA-EP.
8.3 Emerging Therapies (2023-2025 Updates)
Recent evidence (Wang et al., 2024; Deleuze et al., 2023; FIGO 2025 update) highlights:
- Immune checkpoint inhibitors (pembrolizumab, avelumab): PSTT/ETT express PD-L1 and show evidence of immune tolerance. Pembrolizumab has been used in combination with multi-agent chemotherapy for high-risk or refractory PSTT. The FIGO 2025 update explicitly mentions pembrolizumab as an option for high-risk PSTT with advanced stage or antecedent pregnancy interval ≥48 months.
- Anti-angiogenic agents (apatinib/sunitinib): Tyrosine kinase inhibitors targeting VEGF pathway are under investigation
- Molecular profiling may help identify targetable mutations in refractory disease
[Wang et al., Hematol Oncol Clin North Am, 2024 - PMID 39322463] | [Ngan et al., IJGO 2025 - PMID 40631439]
9. Prognosis and Prognostic Factors
Overall, PSTT has a favorable prognosis when confined to the uterus (Stage I). However, metastatic disease carries poor outcomes.
Mortality: 10-15% of patients die of disseminated disease (Robbins, Cotran & Kumar).
Key Adverse Prognostic Factors:
| Factor | Comment |
|---|---|
| Interval >48 months from antecedent pregnancy | Single most important adverse prognostic factor |
| Advanced FIGO stage (II-IV) | Independently poor prognosis |
| Deep myometrial invasion | |
| High mitotic index | >5 mitoses/10 HPF correlates with aggressive behavior |
| Tumor necrosis | |
| Metastasis at presentation | |
| Age >35 years | Some series |
The interval from last pregnancy is so critical that it defines the high-risk cutoff for chemotherapy (≥48 months = high risk, analogous to the WHO score interval variable in standard GTN).
Stage-specific outcomes:
- Stage I (uterus confined): Excellent - surgical cure rate >90%
- Metastatic/high-risk: 5-year survival ~50-70% with aggressive therapy; outcomes significantly worse than other GTN
10. Comparison: PSTT vs. ETT vs. Choriocarcinoma
| Feature | PSTT | ETT | Choriocarcinoma |
|---|---|---|---|
| Cell of origin | Implantation site IT | Chorionic-type IT | Cytotrophoblast + syncytiotrophoblast |
| hCG | Low/absent | Low/absent | High |
| hPL | Strongly positive | Weak | Weak |
| p63 | Negative | Positive | Negative |
| Histology | Infiltrating mononuclear cells | Nested epithelioid cells, hyaline material | Biphasic, hemorrhagic, necrotic |
| Invasion | Splits muscle fibers | Less invasive | Destructive, hemorrhagic |
| Chemo sensitivity | Relatively resistant | Relatively resistant | Very sensitive |
| Treatment | Surgery + chemo for metastatic | Surgery + chemo for metastatic | Chemotherapy primarily |
| Prognosis | Good if localized | Good if localized | Excellent even with metastasis |
11. Differential Diagnosis
- Choriocarcinoma: Biphasic, high hCG, hemorrhagic - distinguished by IHC and hCG levels
- ETT: Mononuclear cells with hyaline deposits, p63-positive - key differential; ETT tends to be more circumscribed
- Exaggerated placental site reaction (EPS): Physiologic infiltration by intermediate trophoblasts; distinguished by absence of mitoses, no atypia, and clinical context (early pregnancy)
- Placental site nodule (PSN): Hyalinized, focal, incidental - low-mitotic, small; precursor lesion to ETT
- Epithelioid leiomyosarcoma: Negative for trophoblastic markers; cytokeratin pattern differs
- Poorly differentiated carcinoma: IHC panel resolves (cytokeratin pattern, hPL, hCG)
12. FIGO/WHO 2025 Guideline Update - Key Points for PSTT
The FIGO 2025 update (Ngan et al., IJGO 2025 - PMID 40631439) emphasizes:
- Molecular genetic studies are increasingly helpful alongside histology for diagnosis of GTD
- hCG monitoring after treatment is essential but levels may remain low/borderline in PSTT - hPL is a complementary marker
- High-risk PSTT (stage ≥II or interval ≥48 months): multi-agent chemotherapy (EMA-EP) ± pembrolizumab
- Immunotherapy (pembrolizumab) is now explicitly mentioned as an option in recurrent/refractory PSTT
- Late mortality still occurs from treatment-resistant tumors - ongoing research into novel therapies is needed
The Wang et al. 2024 review (PMID 39322463) in Hematol Oncol Clin North Am specifically states:
"Multi-agent chemotherapy ± pembrolizumab is added for those with high risk features defined as advanced stage disease and those diagnosed ≥48 months from the antecedent pregnancy. Survival for early stage, low risk disease remains quite good but the prognosis for high-risk disease is poor."
Summary Mnemonic: PSTT Features
P - Polygonal intermediate trophoblasts, hPL-positive
S - Surgery (hysterectomy) is cornerstone; Splays smooth muscle fibers
T - Typically follows Term pregnancy (50%); Tropism for vessels
T - hCG is Trivially low (disproportionate to tumor mass)
High-risk = interval >48 months + advanced stage → EMA-EP ± pembrolizumab
S - Surgery (hysterectomy) is cornerstone; Splays smooth muscle fibers
T - Typically follows Term pregnancy (50%); Tropism for vessels
T - hCG is Trivially low (disproportionate to tumor mass)
High-risk = interval >48 months + advanced stage → EMA-EP ± pembrolizumab
Sources:
- Robbins & Kumar Basic Pathology - p. 620
- Robbins, Cotran & Kumar Pathologic Basis of Disease - p. 957-958
- Berek & Novak's Gynecology - pp. 2492-2508
- Schwartz's Principles of Surgery, 11th ed.
- Wang V et al. PSTT and ETT. Hematol Oncol Clin North Am. 2024 Dec. PMID 39322463
- Ngan HYS et al. Diagnosis and management of GTD: 2025 update. Int J Gynaecol Obstet. 2025. PMID 40631439
- Deleuze A et al. Management of trophoblastic tumors. Expert Rev Anticancer Ther. 2023. PMID 37198729
This is a shared conversation. Sign in to Orris to start your own chat.