I now have comprehensive information and excellent images. Let me compose the full detailed answer.
Charnley's Compression Arthrodesis - Complete Review
Historical Background
Sir John Charnley (1911-1982), the British orthopaedic surgeon best known for pioneering total hip replacement, also made a foundational contribution to joint arthrodesis. Inspired by the work of Roger Anderson and post-WWII external fixation research, Charnley developed and popularized compression arthrodesis as a technique for reliably fusing joints - particularly the knee, shoulder, and ankle. His landmark 1948 paper described positive-pressure arthrodesis of the knee, and in 1960 he reported a consolidation rate of 98.8% in 171 knee arthrodeses performed by 10 surgeons at his clinic, applying ~45 kg of compression via an external fixator. (Rockwood & Green's Fractures in Adults, 10th Ed.)
What is Compression Arthrodesis?
Arthrodesis means surgical fusion of a joint - elimination of movement by inducing bony union across the joint surfaces. Compression arthrodesis is the technique of applying controlled axial compressive force across denuded bone surfaces to accelerate and ensure bony union, based on the biological principle that compression stimulates osteogenesis (Wolff's law).
Charnley's method specifically uses a specially designed external compression clamp (the "Charnley clamp") with transfixion pins driven through the femur and tibia, connected by adjustable side bars that can be tightened to apply continuous axial compression across the knee joint.
Illustrative Diagrams
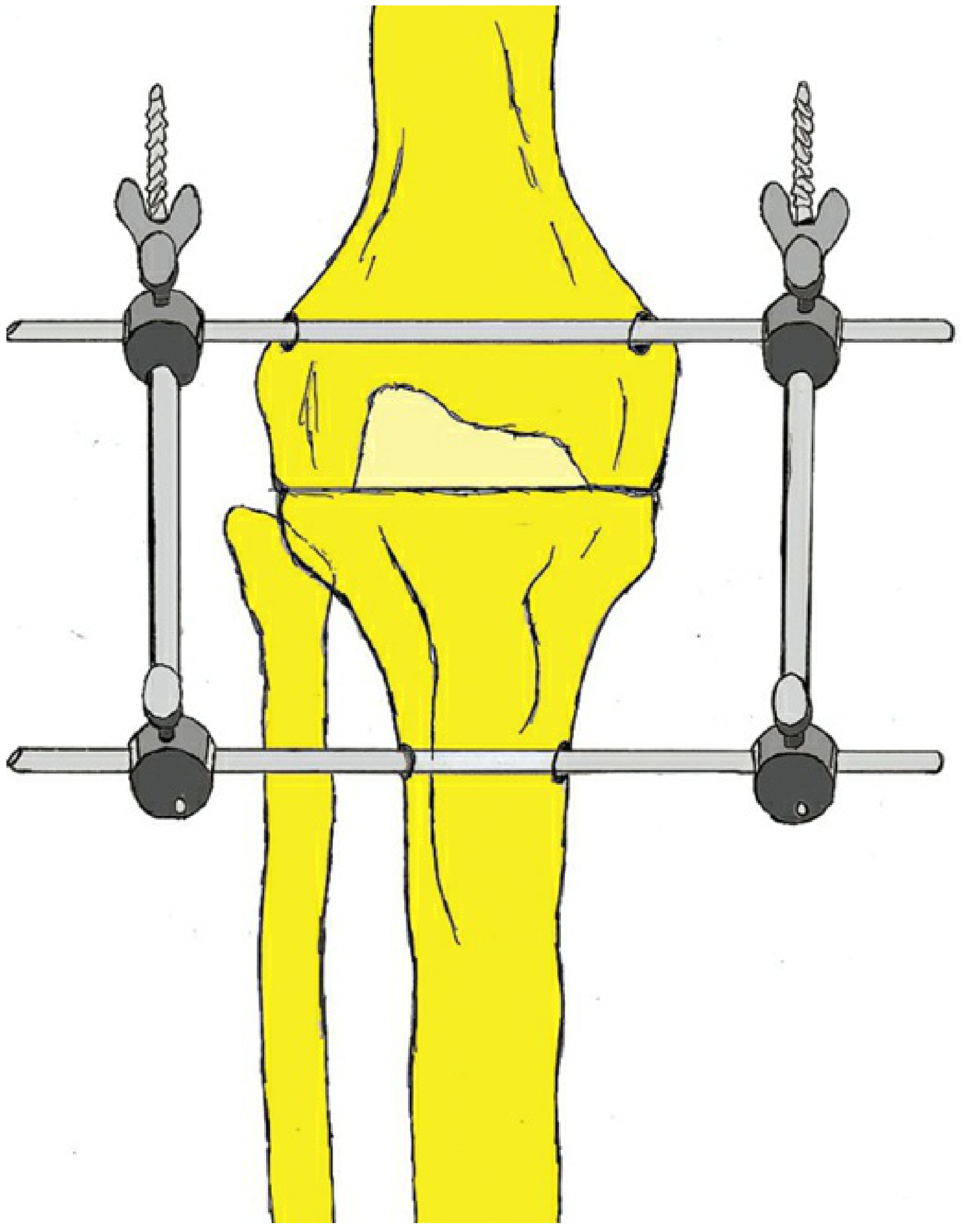
Charnley's simple "compression" fixator for arthrodesis - transfixion pins in femur and tibia connected by side bars with clamps. Compression is applied by tightening the connecting rods. (Rockwood & Green's Fractures in Adults, 10th Ed.)
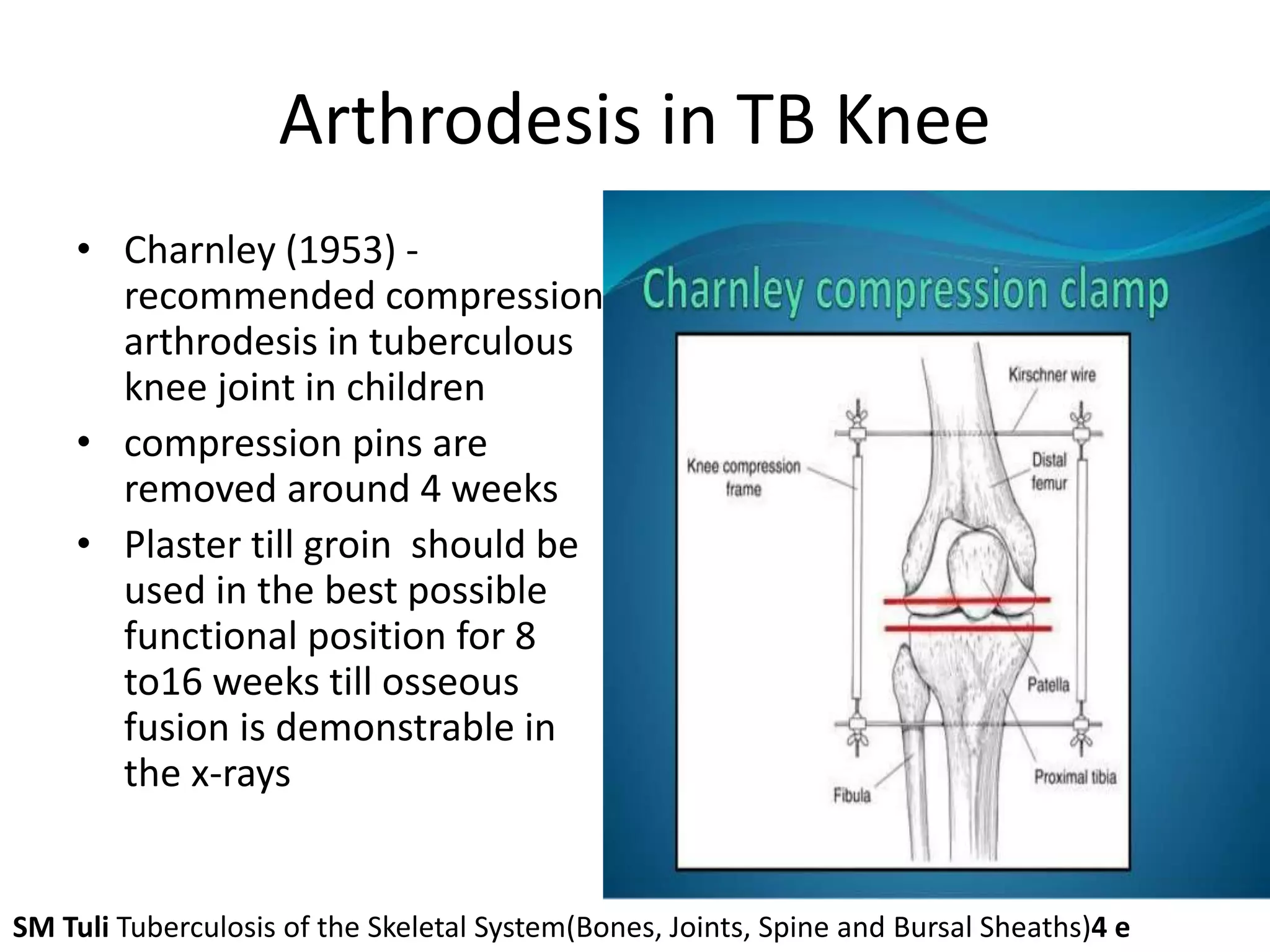
Labeled diagram of Charnley's compression clamp applied to the knee: Kirschner wires/pins, knee compression frame, distal femur, patella, proximal tibia, and fibula. (Based on SM Tuli - Tuberculosis of the Skeletal System)
External compression fixation applied to the shoulder joint for glenohumeral arthrodesis (Charnley and Houston technique) - Campbell's Operative Orthopaedics 15th Ed.
1. Etiology / Background Conditions
Charnley's compression arthrodesis addresses the end-stage destruction of a joint where pain relief and stability are the priority and joint preservation/replacement is not feasible. The common underlying conditions include:
Primary Disease Causes:
| Etiology | Notes |
|---|
| Tuberculous (TB) arthritis | Historically the most common indication; joint destruction with "triple deformity" in the knee |
| Septic arthritis | Acute or chronic pyogenic infection destroying articular cartilage |
| Rheumatoid arthritis | End-stage inflammatory destruction |
| Osteoarthritis (Gonarthrosis) | Severe degenerative disease - historically used before TKA |
| Post-traumatic arthritis | Following intra-articular fractures with articular cartilage destruction |
| Failed total knee arthroplasty (TKA) | Current most common indication in developed settings |
| Neuropathic (Charcot) joint | Bony destruction with severe instability |
| Tumour surgery | After resection of distal femur or proximal tibia when endoprosthesis is not feasible |
| Failed fracture fixation | Around the knee with bone loss |
2. Indications
Absolute Indications:
- Chronic or recurrent septic arthritis of the knee (including TB) with severe joint destruction
- Failed TKA with infection and bone loss where revision arthroplasty is not feasible
- Neuropathic knee (Charcot arthropathy) with severe instability and bony destruction
- Severe post-traumatic arthritis where arthroplasty is contraindicated (young, heavy, active patients)
- Irreparable ligamentous instability with cartilage destruction
Relative Indications:
- End-stage gonarthrosis in young patients (< 40 years) with high physical demand
- After tumour resection (distal femur/proximal tibia) when endoprosthesis fails or is not available
- Multiple drug-resistant infection or immunocompromised patients where arthroplasty would inevitably re-infect
Specific Indication for Charnley's External Fixator Technique:
- Relatively minimal bony loss (allowing good bony apposition and contact)
- Adequate bone stock to accept and hold transfixion pins securely for 8-12 weeks
- Active infection present (external fixator avoids implanting metal in infected field)
- Patient willing and able to manage external frame
3. Contraindications
- Progressively septic course with impending multi-organ failure
- General inoperability / unfit for anaesthesia
- Previously bedridden patients (fusion removes any residual function)
- Spinal cord injury / paraplegia (ambulatory benefit is lost)
- Peripheral arterial disease stage IV (healing risk)
- Severe osteoporosis (pins will not hold adequately)
- Extensive bone loss preventing bony apposition (relative - may need bone grafting)
4. Principles of Compression Arthrodesis
The technique rests on four biological and mechanical principles:
Principle 1: Compression Promotes Osteogenesis
Sustained axial compression across denuded cancellous surfaces stimulates osteoblastic activity and accelerates bone union. Charnley applied approximately 45 kg (100 lbs) of compressive force. This follows Wolff's law: bone responds to mechanical stress by remodeling and depositing new bone.
Principle 2: Rigid Fixation
Micromotion at the fusion interface prevents bony union and encourages fibrous tissue formation. The external clamp provides sufficient rigidity to eliminate interfragmentary motion.
Principle 3: Maximum Bony Contact
Removal of cartilage and subchondral bone down to well-vascularized cancellous bone maximizes the contact area for bone ingrowth. Flat, parallel cuts (osteotomy) ensure congruent apposition.
Principle 4: Optimal Position of Fusion
The joint must be fused in the most functionally useful position to allow ambulation and activities of daily living.
Position of fusion for the knee:
- 0-5° of valgus (slight outward alignment)
- 5-15° of flexion (allows toe clearance during swing phase)
- Neutral rotation (slight external rotation acceptable)
- Shortening ~1 cm (limb length discrepancy minimized)
5. Procedure - Step-by-Step
Pre-operative Planning:
- Full clinical assessment, X-rays (AP and lateral), CT scan to assess bone stock
- ESR, CRP, WBC, blood cultures (particularly in infected cases)
- Scannogram to assess limb lengths and plan for shortening
- Antibiotic therapy if active infection (ideally 6 weeks before surgery in TB)
- Pre-operative counseling regarding permanent stiffness, shortening, and timeline
Surgical Steps (Knee - Classic Charnley Technique):
Step 1: Anaesthesia and Positioning
- General or spinal anaesthesia.
- Patient supine with a tourniquet applied to the thigh.
- The affected limb is draped free.
Step 2: Incision
- An anterior midline longitudinal incision is made over the knee from lower thigh to upper tibia.
- Alternatively, the pre-existing scar from previous surgery is utilized.
Step 3: Joint Exposure
- The knee joint is opened through a medial parapatellar approach.
- Thickened, fibrous, or infected synovium is excised (synovectomy).
- The patella is everted or reflected.
Step 4: Joint Surface Preparation (Most Critical Step)
- All articular cartilage is denuded from the distal femur and proximal tibia using:
- Oscillating saw
- Osteotome
- Curettes and rongeurs
- Subchondral bone is removed to expose vascular cancellous bleeding bone on both surfaces.
- Flat, parallel cuts are made on the femoral and tibial surfaces to ensure maximum bony contact and accurate alignment.
- The patella may be excised or prepared for incorporation into the fusion mass.
- Bone surfaces are brought together with the knee in the desired position (slight flexion, neutral/slight valgus).
Step 5: Pin Insertion
- Two Steinmann pins or Kirschner wires (or Schanz screws) are driven transversely through the distal femur, perpendicular to its long axis, above the fusion site.
- Two similar pins are driven transversely through the proximal tibia, below the fusion site.
- Pins are placed under fluoroscopic guidance to ensure correct positioning.
- Pin placement must clear neurovascular structures (popliteal vessels, peroneal nerve).
Step 6: Application of Charnley Clamp
- The two Charnley compression bars (side bars with adjustable connecting clamps) are applied on either side of the knee.
- Each bar connects the proximal femoral pin to the distal tibial pin via adjustable clamp devices.
- The bars are tightened symmetrically to apply controlled compression across the fusion site.
- Compression of approximately 45 kg (10 lbs per square inch) is applied.
Step 7: Wound Closure
- The wound is closed in layers over a suction drain.
- Dressing applied around pin sites.
Step 8: Plaster Immobilization
- A well-padded high groin (hip spica-type) plaster cast is applied with the ankle free, incorporating the clamp or applied after pin removal.
- This eliminates rotational forces that the clamp cannot control.
Post-Operative Protocol:
| Phase | Timing | Activity |
|---|
| Immediate post-op | Days 1-7 | Bed rest, limb elevation, pin site care, IV antibiotics if infected |
| Pin removal | 4-6 weeks | Clamp and pins removed under sedation/GA once early union developing |
| Cast immobilization | After pin removal to 8-16 weeks | High groin cast with ankle free; non-weight bearing then partial weight bearing |
| Full weight bearing | When radiographic fusion confirmed (trabecular bridging across fusion site on 2 views) | Usually 3-6 months post-op |
| Physiotherapy | Throughout | Hip and ankle range of motion exercises; quadriceps strengthening |
| Shoe raise | After fusion | 1-2 cm raise on contralateral shoe to compensate for shortening |
6. Radiographic Confirmation of Fusion
Endpoint of arthrodesis: Successful when bony trabeculae from femur to tibia are visible in at least two radiographic projections (AP and lateral). No visible fusion line should remain. (Musculoskeletal Key)
7. Outcomes
Charnley's Own Results (1960):
- 171 cases, 10 surgeons
- Consolidation rate: 98.8%
- Common etiologies: post-TB joint destruction, gonarthrosis, rheumatoid arthritis
- Minimal operative time and minimal complications
Recent Clinical Outcomes (Shah et al., Cureus 2024 - [PMID: 39583435]):
- 15 patients, Charnley's compression clamps
- Septic arthritis and tuberculosis most common indications (>70% previously operated on the same knee)
- Fixator duration: 35.73 weeks average (range 32-39 weeks / ~8 months)
- Knee Society Score improved: 16.2 → 54 (out of 100)
- Functional score improved: 43.6 → 89.66 (out of 100)
- Fusion rate: high; complications relatively few
- Conclusion: "easy, cost-effective, and comfortable for patients"
Comparative Fusion Rates (External Fixator Methods):
| Method | Fusion Rate |
|---|
| Charnley external clamp (simple) | ~83-99% |
| Monolateral external fixator | ~80-90% |
| Circular/Ilizarov frame | ~85-95% |
| Intramedullary nail (gold standard) | ~90-100% |
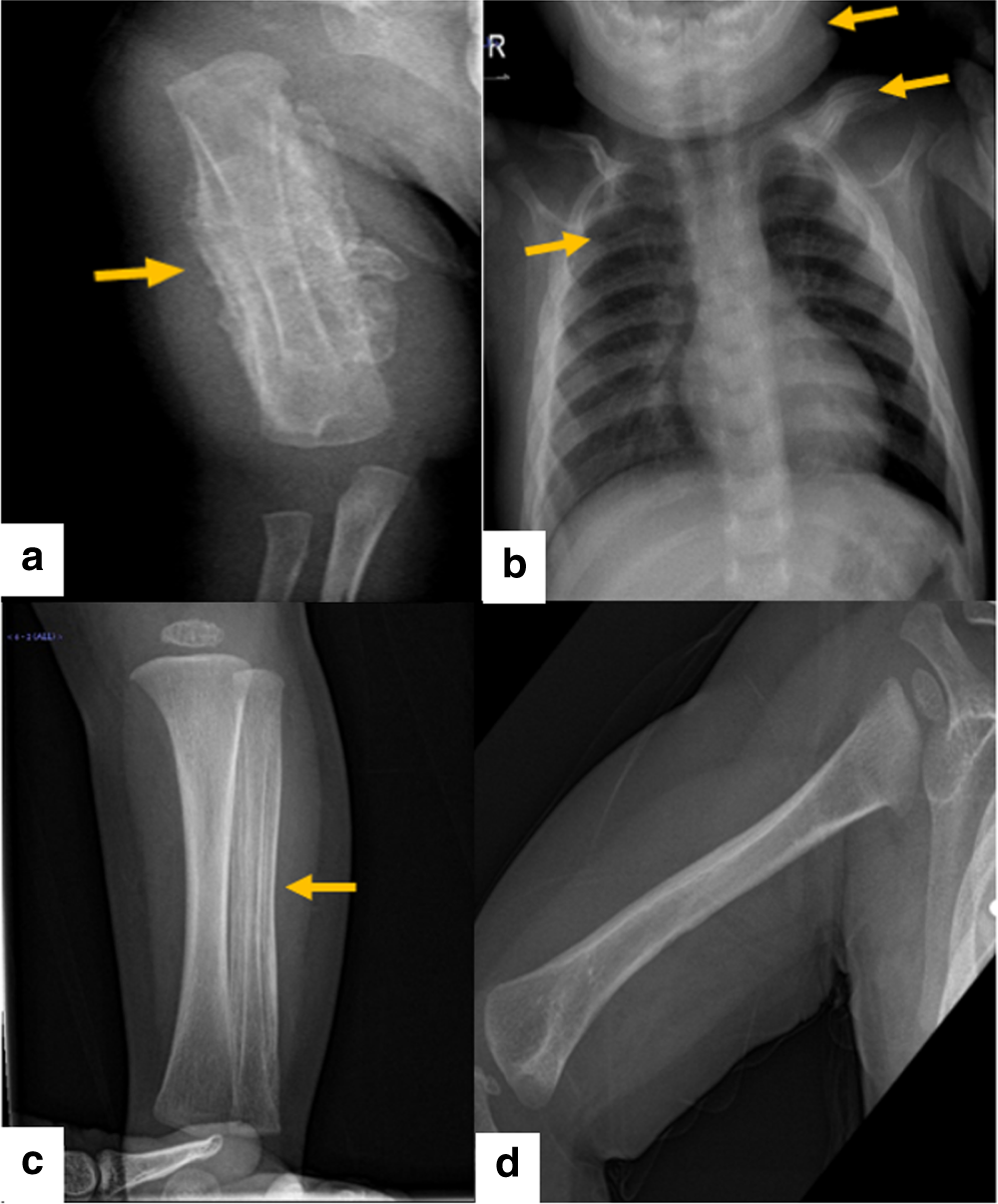
Radiographs showing knee arthrodesis with external compression fixator - (a,b) with fixator in situ, (c,d) after fixator removal with bony union confirmed.
8. Comparison with Other Arthrodesis Methods
Principal historical methods of knee arthrodesis: Key (external compression - bottom left), intra-articular fusion, Gray, Bosworth, Galloway, Albee, Hatt, Milgram, Hibbs, Henderson, Brittain.
| Method | Principle | Best For |
|---|
| Charnley external clamp | External compression | Infected knee, minimal bone loss, cost-effective setting |
| Intramedullary nail (long) | Axial compression + rigid fixation | Non-infected cases, maximum bone stock |
| Circular external fixator (Ilizarov) | Multi-plane compression + bone transport | Bone loss, deformity, complex cases |
| Dual plate construct | Rigid internal fixation | Non-infected; large bone stock |
| Hybrid (nail + external) | Combined | Complex cases, revision |
9. Advantages of Charnley's Compression Arthrodesis
Technical Advantages:
- Simple device - Two pins + two connecting bars; easy to learn and apply
- Cost-effective - Significantly cheaper than intramedullary nails or ring fixators
- No internal implant in infected field - Ideal for active septic arthritis or TB (avoids osteomyelitis from retained metal)
- Adjustable compression - Can increase or decrease compression at any time post-operatively
- Reversible - Pins can be removed if needed; does not commit to permanent metalwork
- Minimal dissection - Less soft-tissue stripping than plating
- Allows wound inspection - Open wounds or infected cavities can be managed simultaneously
- Suitable for children - Does not violate growth plates if pins placed correctly
Biological Advantages:
- Promotes faster fusion - Compression directly stimulates periosteal and endosteal bone formation
- High fusion rate - ~98.8% in Charnley's own series
- Works in infected bone - Compression arthrodesis is effective even with active infection (unlike internal fixation)
Clinical Advantages:
- Effective pain relief - Elimination of painful articular motion
- Stable weight-bearing limb - Allows ambulation (with aids)
- Eliminates septic focus - Joint debridement + fusion cures chronic knee infection
- Reproducible results - Multiple surgeons can achieve consistent outcomes
10. Disadvantages of Charnley's Compression Arthrodesis
Functional Disadvantages:
- Permanent loss of knee motion - Patient cannot bend the knee; significant functional limitation
- Difficulty sitting - Restricted in aircraft seats, theaters, small cars
- Climbing - Difficulty with stairs, ladders
- Increased energy expenditure - Walking energy cost increased by ~25% compared to healthy individuals
- 50% require permanent crutches - Long-term walking aids
- Limb shortening (~1-2 cm unavoidable) - Requires shoe raise, may cause gait abnormality
- Increased stress on adjacent joints - Hip and ankle develop accelerated degeneration
Device-Specific Disadvantages:
- Pin-tract infection - Most common complication; daily pin care essential
- Pin loosening - Especially in osteoporotic bone; may require replacement
- Frame discomfort - Bulky external hardware restricts mobility and clothing
- Rotational control limited - The simple clamp does not resist rotation well; requires plaster cast supplement
- Reduced fusion rate vs. intramedullary nail - External fixator alone has lower rates than locked IM nail for non-infected cases
- Long fixator duration - Average ~8 months (35 weeks) before removal
Psychological Disadvantages:
- Irreversibility - Patient must accept permanent stiffness
- Body image concerns - Altered gait, limb length discrepancy
11. Complications
| Complication | Frequency | Management |
|---|
| Pin-tract infection | Most common | Daily cleaning, antibiotics; pin change if severe |
| Pin loosening | Common | Re-tightening; re-pinning |
| Non-union / delayed union | Uncommon | Prolonged compression, bone grafting, change to IM nail |
| Malunion (varus/valgus/excessive flexion) | Avoidable with care | Corrective osteotomy if severe |
| Limb length discrepancy | Expected ~1 cm | Shoe raise |
| Wound infection / breakdown | Uncommon | Antibiotics, wound care |
| Deep vein thrombosis | Possible | Prophylaxis (LMWH, TED stockings) |
| Peroneal nerve palsy | Rare | Pin placement precautions |
| Vascular injury | Rare | Careful technique |
| Refracture (after fixator removal) | Rare | Protection with cast until union confirmed |
| Adjacent joint degeneration (hip, ankle) | Long-term | Conservative management; eventual arthroplasty |
12. Charnley's Technique for Other Joints
Charnley extended his compression arthrodesis technique beyond the knee:
Shoulder (Charnley-Houston Technique) - Campbell's Operative Orthopaedics 15th Ed.:
- Beach-chair position; "saber cut" incision over lateral acromion
- Deltoid reflected; subacromial space excised
- Articular cartilage removed from humeral head and glenoid fossa; acromion undersurface decorticated
- Greater tuberosity resected; bone used as graft
- Pins inserted: scapular spine (proximal) and humeral surgical neck (distal)
- External compression frame applied to connect proximal and distal pins
- Deltoid reattached; wound closed
Position of shoulder fusion: 20° abduction, 30° flexion, 40° internal rotation
Ankle Arthrodesis:
Charnley also described compression arthrodesis of the ankle (1951) using the same external compression principle with transfixion pins through tibia and calcaneus/talus.
Summary Table
| Feature | Detail |
|---|
| Originator | Sir John Charnley, 1948 (knee), 1951 (ankle, shoulder) |
| Principle | Axial compression (~45 kg) across denuded bone surfaces stimulates osteogenesis |
| Device | External compression clamp: 2 femoral + 2 tibial transfixion pins connected by adjustable side bars |
| Best indication | Infected knee (TB, septic), failed TKA, neuropathic joint - minimal bone loss |
| Optimal position (knee) | 0-5° valgus, 5-15° flexion, neutral rotation, ~1 cm shortening |
| Fusion rate | 98.8% (Charnley 1960); ~83-99% modern series |
| Fixator duration | Average 4-6 weeks (pins), then cast 8-16 weeks; total ~6-9 months |
| Key advantage | Simple, cheap, no implant in infected field, high fusion rate |
| Key disadvantage | Permanent stiffness, pin-tract infection, bulky frame, increased energy expenditure |
| Outcome | Excellent pain relief, stable limb; 25% increased walking energy cost |