Here is a complete, exam-ready guide covering all the MUHS 2nd MBBS Pathology topics you listed, drawn directly from Robbins & Cotran Pathologic Basis of Disease and Robbins & Kumar Basic Pathology.
NEOPLASIA - Complete MUHS Exam Notes
1. NEOPLASIA - Definition and Classification
Definition (Robbins)
"A neoplasm is an abnormal mass of tissue, the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the same excessive manner after cessation of the stimuli which evoked the change." - Willis
Key points:
- Growth is autonomous (not regulated by normal controls)
- Monoclonal in origin (arises from a single transformed cell)
- Contains two components: parenchyma (neoplastic cells) and stroma (connective tissue + vessels)
Classification of Neoplasms
| Feature | Benign | Malignant |
|---|
| Differentiation | Well differentiated | Variable - poorly differentiated (anaplastic) |
| Rate of growth | Slow | Rapid, variable |
| Mode of growth | Expansile, encapsulated | Infiltrative, invasive |
| Metastasis | ABSENT | PRESENT |
| Recurrence | Rare | Common |
| Capsule | Present | Absent (usually) |
| Necrosis/hemorrhage | Uncommon | Common |
| Mitoses | Rare, normal | Frequent, abnormal |
| Effect on host | Usually local | Cachexia, death |
| Nuclear features | Normal N:C ratio | High N:C ratio, hyperchromatism |
Nomenclature Table
| Tissue of Origin | Benign | Malignant |
|---|
| Epithelium (gland) | Adenoma | Adenocarcinoma |
| Epithelium (surface) | Papilloma | Squamous cell carcinoma |
| Fibrous tissue | Fibroma | Fibrosarcoma |
| Smooth muscle | Leiomyoma | Leiomyosarcoma |
| Fat | Lipoma | Liposarcoma |
| Blood vessel | Hemangioma | Angiosarcoma |
| Bone | Osteoma | Osteosarcoma |
| Lymphocytes | - | Lymphoma |
| Plasma cells | - | Multiple myeloma |
| Melanocytes | Nevus | Melanoma |
| All 3 germ layers | Teratoma (mature) | Teratocarcinoma (immature) |
2. DIFFERENCES - Benign vs Malignant Neoplasms
Gross Appearance
Benign:
- Rounded, well-circumscribed
- Usually encapsulated (fibrous capsule)
- Smooth surface
- Homogeneous cut surface
- No necrosis or hemorrhage
- Example: Uterine leiomyoma - "whorled white firm nodule"
Malignant:
- Irregular, ill-defined margins
- No capsule (invades surrounding tissue)
- Irregular surface
- Heterogeneous - areas of necrosis, hemorrhage
- "Crab-like" projections (hence "cancer" from Latin cancer = crab)
- Example: Carcinoma breast - hard, gritty, irregular mass with spiculated margins
Easy-to-Draw Gross Diagram
BENIGN TUMOR MALIGNANT TUMOR
___________ ~~~~~~~~~~~
/ \ / Necrosis \
| Homogenous | | /~~~~~~~~\ |
| well-defined| | |Hemorrhage| |
| mass | | \~~~~~~~~/ |
\___________ / \~irregular~/
[Smooth capsule] [No capsule, irregular]
3. ANAPLASTIC TUMOR CELLS - Morphology
Anaplasia = loss of differentiation; hallmark of malignant neoplasms.
Morphological Features of Anaplastic Cells
Nuclear Changes (MOST IMPORTANT):
- Pleomorphism - variation in size and shape of nuclei and cells
- Hyperchromatism - dark-staining nuclei (excess DNA)
- High nuclear:cytoplasmic (N:C) ratio - normally 1:4 to 1:6; in cancer cells approaches 1:1
- Prominent nucleoli - large, often multiple, "owl eye" appearance
- Abnormal mitoses - tripolar, quadripolar spindles; bizarre mitotic figures
- Coarse chromatin - clumped at nuclear membrane
Cytoplasmic Changes:
- Loss of polarity (cells no longer arranged in organized fashion)
- Loss of cohesion between cells
- Abundant, often basophilic cytoplasm
Architectural Changes:
- Loss of normal tissue architecture
- Sheets and nests of cells without gland formation
- Tumor giant cells - mononucleate or multinucleate
Histopathology Diagram (Easy to Draw in Exam)
NORMAL EPITHELIUM ANAPLASTIC CARCINOMA
[ ] [ ] [ ] [ ] [@@] [@@@] [@]
[ ] [ ] [ ] [ ] [@@@@@][@][@@@@]
[ ] [ ] [ ] [ ] [abnormal mitosis*]
----basement membrane----
Regular nuclei, Irregular, hyperchromatic
organized layers nuclei, loss of polarity
- @ = large irregular dark nucleus
-
- = abnormal mitotic figure (tripolar)
4. TERATOMA
A tumor derived from all three germinal layers (ectoderm, mesoderm, endoderm) arising from totipotent cells.
- Mature teratoma (Dermoid cyst): Benign; most common in ovary; contains hair, teeth, sebaceous material, cartilage, neural tissue
- Immature teratoma: Malignant; contains immature (embryonal) tissues, especially neural elements
- Monodermal teratoma: Specialized; e.g., struma ovarii (all thyroid tissue), carcinoid
Gross: Cystic mass with hair, sebum, teeth (dermoid cyst)
Histology: Multiple tissue types - squamous epithelium, glands, cartilage, neural tissue, bone
5. ROUTES/PATHWAYS OF SPREAD OF MALIGNANT NEOPLASMS
Modes of Metastasis
Metastasis = establishment of secondary tumor growths at a site discontinuous with the primary tumor. It is the single most important criterion of malignancy.
1. Direct/Local Invasion (Contiguous Spread)
- Tumor directly invades and destroys adjacent tissues
- Example: Carcinoma cervix invades bladder/rectum; carcinoma breast invades chest wall
- Mechanism: Proteases (MMPs), loss of E-cadherin, pseudopods
2. Lymphatic Spread (Most common for carcinomas)
- Tumor cells enter lymphatic channels and travel to regional lymph nodes
- Forms tumor emboli in lymph nodes
- Sentinel node = first draining lymph node (important in breast/melanoma surgery)
- Example: Carcinoma breast - axillary lymph nodes; carcinoma tongue - submandibular nodes
- Virchow's node = left supraclavicular node; enlarged in gastric carcinoma (Troisier's sign)
3. Hematogenous Spread (Most common for sarcomas)
- Tumor enters blood vessels (veins more than arteries - thinner walls)
- Portal system drains to liver; systemic veins to lungs
- Liver and lungs are most common sites of blood-borne metastases
- Example: Renal cell carcinoma - lung metastases; colon carcinoma - liver metastases; prostate - bone ("osteoblastic" metastases)
- Mechanism: Tumor cells secrete VEGF - angiogenesis - enter vessels - survive in circulation - adhere to endothelium - extravasate - proliferate
4. Transcoelomic (Seeding of Body Cavities)
- Tumor cells shed into peritoneal, pleural, or pericardial cavities
- Example: Ovarian carcinoma seeds peritoneum (pseudomyxoma peritonei); gastric carcinoma seeds peritoneum causing Krukenberg tumor (bilateral ovarian metastasis with signet ring cells)
5. Perineural Spread
- Tumor spreads along nerve sheaths
- Example: Carcinoma prostate, pancreas - perineural invasion
- Explains pain in many cancers
Metastasis - Mechanism (Invasion-Metastasis Cascade)
PRIMARY TUMOR
|
v
Invasion of ECM (loss of E-cadherin, ↑ MMPs)
|
v
Intravasation into blood/lymph vessels
|
v
Survival in circulation (evasion of NK cells)
|
v
Arrest in target organ capillaries
|
v
Extravasation
|
v
Proliferation → METASTATIC DEPOSIT
"Seed and soil" hypothesis (Paget, 1889): The tumor cell (seed) only grows in a compatible microenvironment (soil). Example: Prostate cancer metastasizes to bone because bone marrow provides growth factors for prostate cells.
6. LABORATORY DIAGNOSIS OF CANCER
(Robbins & Cotran, Block 4)
A. Histologic and Cytologic Methods
1. Excision Biopsy
- Most definitive method
- Entire lesion removed and examined
- Used for small accessible lesions
2. Incision Biopsy / Core Needle Biopsy
- Part of lesion taken
- Used for large, deep-seated lesions
3. Fine Needle Aspiration Cytology (FNAC)
- Small-bore needle aspirates cells
- Examined as smear on slide
- Rapid, minimally invasive
- Used for breast lump, thyroid, lymph nodes
- Limitation: Cannot assess architecture (only cytology)
4. Cytologic Smears (Exfoliative Cytology)
- Cells shed naturally examined
- Pap smear - cervical cancer screening
- Sputum cytology - lung cancer
- Urine cytology - bladder cancer
- Pleural/ascitic fluid cytology
5. Frozen Section
- Rapid intraoperative histology (within 30 minutes)
- Used to assess surgical margins during cancer surgery
- Limitation: Inferior morphologic detail
B. Immunohistochemistry (IHC)
- Antibodies against tissue-specific antigens
- Identifies cell lineage of poorly differentiated tumors
| Marker | Tumor Type |
|---|
| Cytokeratin | Carcinomas |
| Vimentin | Sarcomas |
| Desmin | Muscle tumors |
| LCA (CD45) | Lymphomas |
| S-100 | Neural tumors, melanoma |
| PSA | Prostate carcinoma |
| HER2/neu | Breast carcinoma |
| AFP | Hepatocellular carcinoma, yolk sac |
| CD20 | B-cell lymphoma |
| CD3 | T-cell lymphoma |
C. Flow Cytometry
- Rapid analysis of cell surface proteins, DNA content
- Used for classification of hematopoietic neoplasms
- Detects aneuploidy (abnormal DNA content - marker of malignancy)
D. Tumor Grading and Staging
Grading (cytologic appearance):
- Grade 1 (well-differentiated) - low malignancy
- Grade 2 (moderately differentiated)
- Grade 3 (poorly differentiated) - high malignancy
- Grade 4 (undifferentiated/anaplastic)
Staging (extent of disease):
TNM system:
- T = Primary tumor size (T0-T4)
- N = Regional lymph node involvement (N0-N3)
- M = Distant metastasis (M0-M1)
Staging is of greater clinical value than grading.
E. Molecular Diagnosis
- PCR - detects specific translocations (e.g., BCR-ABL in CML, t(9;22))
- FISH - detects gene amplifications (HER2 in breast cancer, MYCN in neuroblastoma)
- DNA sequencing - identifies driver mutations (TP53, KRAS, BRAF)
- Liquid biopsy - circulating tumor DNA (ctDNA) in blood
- Next-generation sequencing (NGS) - comprehensive mutational profiling
7. TUMOR MARKERS - Role in Diagnosis
Tumor markers are substances (proteins, hormones, enzymes) produced by neoplastic cells or host in response to tumor, detectable in blood or body fluids.
Uses of Tumor Markers
- Screening (limited use - poor sensitivity/specificity)
- Monitoring response to therapy
- Detecting recurrence after treatment (most important use)
- Prognosis
Important Tumor Markers Table
| Marker | Tumor | Normal Level | Notes |
|---|
| PSA (Prostate Specific Antigen) | Prostate carcinoma | <4 ng/mL | Elevated in BPH too - low specificity |
| AFP (Alpha-fetoprotein) | HCC, Yolk sac tumor, Embryonal carcinoma | <10 ng/mL | Elevated in cirrhosis, hepatitis |
| CEA (Carcinoembryonic Antigen) | Colon, Pancreas, Stomach, Breast | <5 ng/mL | Used to monitor colon cancer recurrence |
| CA-125 | Ovarian carcinoma | <35 U/mL | Elevated in endometriosis, PID |
| CA 19-9 | Pancreatic carcinoma | <37 U/mL | Also biliary tract, GI cancers |
| CA 15-3 | Breast carcinoma | <30 U/mL | Monitoring metastatic breast cancer |
| hCG (beta-hCG) | Choriocarcinoma, Testicular germ cell | - | Very sensitive for choriocarcinoma |
| LDH | Lymphoma, testicular cancer | - | Non-specific |
| Calcitonin | Medullary thyroid carcinoma | <10 pg/mL | Screening in MEN2 families |
| S-100 | Melanoma, Schwannoma | - | |
| Chromogranin A | Neuroendocrine tumors, Carcinoid | - | |
| Thyroglobulin | Differentiated thyroid carcinoma | - | Post-thyroidectomy monitoring |
Limitations
- Low sensitivity (cancer may not produce marker)
- Low specificity (benign conditions also elevate markers)
- Best used for monitoring, not primary diagnosis
8. ONCOGENIC VIRUSES - Enumerate, Cancer Caused by Each
(Robbins & Cotran Block 4)
RNA Oncogenic Viruses
| Virus | Type | Cancer Caused | Mechanism |
|---|
| HTLV-1 (Human T-Cell Leukemia Virus Type 1) | Retrovirus | Adult T-cell leukemia/lymphoma (ATLL) | Tax and HBZ proteins activate NF-kB, promote T-cell proliferation |
DNA Oncogenic Viruses
| Virus | Type | Cancer Caused | Mechanism |
|---|
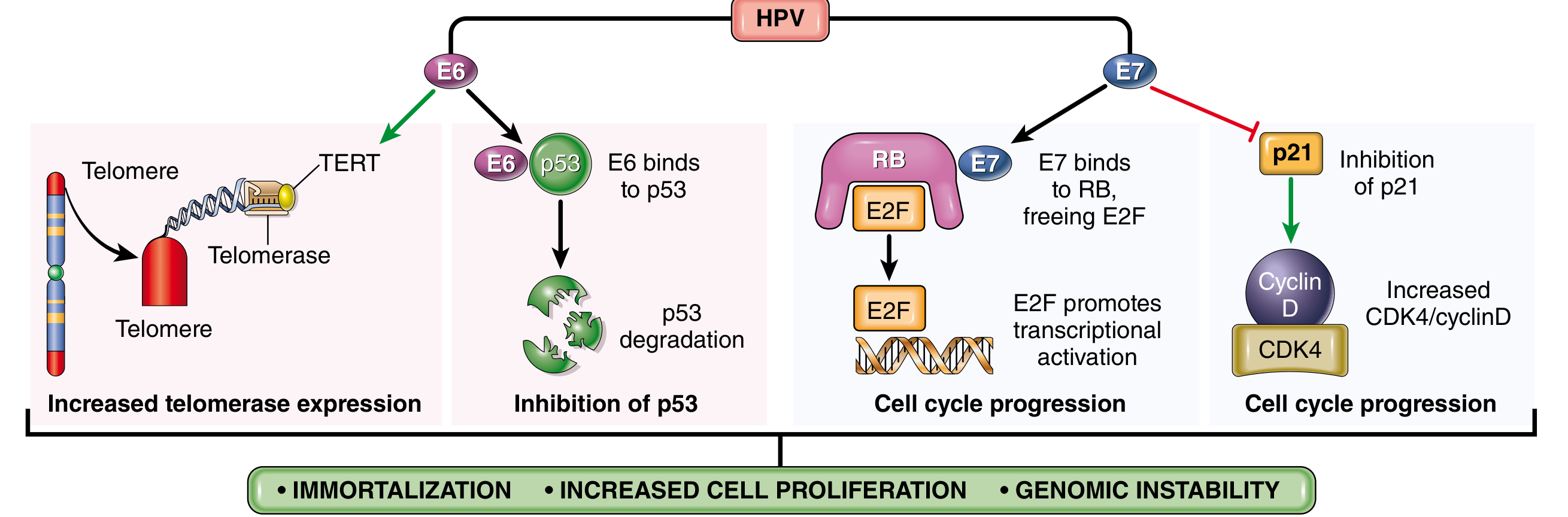
| HPV (Human Papillomavirus) 16, 18 | Papovavirus | Cervical carcinoma, Oropharyngeal cancer, Anal carcinoma, Vulvar carcinoma | E6 inhibits p53; E7 inhibits RB protein |
| EBV (Epstein-Barr Virus) | Herpesvirus | Burkitt lymphoma, Nasopharyngeal carcinoma, Hodgkin lymphoma (mixed cellularity), EBV+ diffuse large B-cell lymphoma | LMP1 mimics CD40 (activates NF-kB, JAK/STAT); EBNA2 activates MYC |
| HBV (Hepatitis B Virus) | Hepadnavirus | Hepatocellular carcinoma | Chronic inflammation, cirrhosis, HBx protein activates telomerase |
| HCV (Hepatitis C Virus) | Flavivirus (RNA) | Hepatocellular carcinoma | Chronic inflammation, cirrhosis |
| KSHV/HHV-8 (Kaposi Sarcoma Herpesvirus) | Herpesvirus | Kaposi sarcoma, Primary effusion lymphoma | Viral FLICE inhibitory protein (vFLIP), viral cyclin D |
| Merkel Cell Polyomavirus | Polyomavirus | Merkel cell carcinoma | Large T antigen inactivates RB |
HPV Mechanism Diagram (from Robbins)
Fig: HPV E6 degrades p53 (prevents apoptosis) and activates TERT (telomerase). E7 binds RB, releasing E2F for uncontrolled cell cycle progression and inhibits p21. Net result: immortalization + increased proliferation + genomic instability.
Also: Bacterial Carcinogen
- H. pylori - Gastric adenocarcinoma and MALT lymphoma
- Mechanism: Chronic inflammation, CagA protein disrupts epithelial signaling
9. CHEMICAL CARCINOGENESIS - Process and Examples
(Robbins & Cotran, Block 3 and 4)
Definition
Chemical carcinogenesis is the process by which chemical agents cause permanent, heritable DNA damage (mutation) leading to malignant transformation.
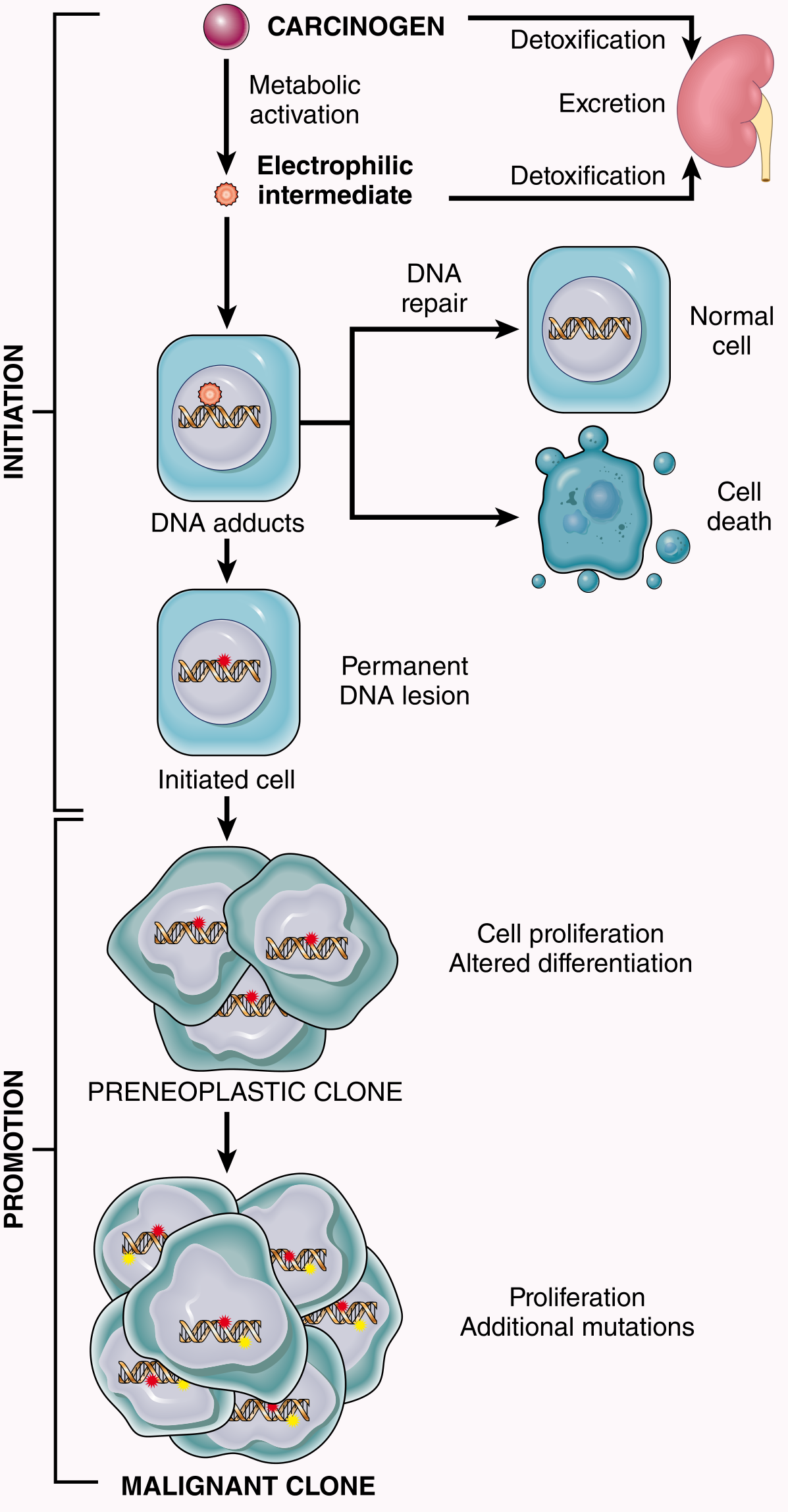
Two-Stage Process: Initiation and Promotion
Fig 7.43: Initiation (permanent DNA damage by carcinogen) followed by Promotion (clonal expansion by promoter) leading to preneoplastic and then malignant clone.
Stage 1: INITIATION
- Exposure to initiating agent (carcinogen)
- Causes permanent, irreversible DNA mutation
- Single exposure sufficient
- Cell does not become malignant immediately
- The mutation is heritable (passed to daughter cells)
- Initiated cells = morphologically normal but genetically altered
- Cannot be reversed
Stage 2: PROMOTION
- Promoters act on initiated cells - no inherent carcinogenicity alone
- Cause clonal expansion of initiated mutated cells
- Stimulate cell proliferation, inhibit apoptosis
- Reversible - if promoter stopped, cells may not progress
- Example: Phorbol esters (TPA), chronic inflammation, unopposed estrogen
Progression
- Further mutations in expanding clone
- Acquisition of additional oncogenic alterations
- Eventual emergence of full malignant phenotype
KEY CONCEPTS
- Initiator without promoter = no tumor
- Promoter without initiator = no tumor
- Initiator first, THEN promoter = TUMOR
- Promoter first, THEN initiator = NO tumor (order matters!)
Classification of Chemical Carcinogens
A. Direct-Acting Carcinogens (do not require metabolic activation)
- Already reactive electrophiles
- Generally weak carcinogens
- Examples: β-Propiolactone, Dimethyl sulfate, Alkylating agents (cyclophosphamide, chlorambucil, nitrosoureas)
- Clinical note: Some anticancer drugs (alkylating agents) can cause secondary AML years later
B. Indirect-Acting Carcinogens (Procarcinogens)
- Require metabolic activation by cytochrome P-450 to become ultimate carcinogens
- More common and more potent
| Carcinogen Class | Example | Cancer Caused |
|---|
| Polycyclic aromatic hydrocarbons | Benzo[a]pyrene (in cigarette smoke, charred meats) | Lung, skin cancer |
| Aromatic amines | 2-Naphthylamine (β-naphthylamine), Benzidine | Bladder cancer (dye/rubber industry) |
| Azo dyes | Dimethylaminoazobenzene ("Butter Yellow") | Liver tumors (in rats) |
| Aflatoxin B1 | Aspergillus flavus (contaminated peanuts/grain) | Hepatocellular carcinoma |
| Nitrosamines | Nitrosamines in preserved meats, tobacco | Gastric, esophageal cancer |
| Vinyl chloride | Industrial chemical | Angiosarcoma of liver |
Mechanism of Action (MOA)
- Chemical carcinogen (procarcinogen) enters cell
- Metabolized by cytochrome P-450 to electrophilic ultimate carcinogen
- Electrophile reacts with nucleophilic sites on DNA (guanine N-7 most common)
- Forms DNA adducts
- If repair fails - permanent mutation in proto-oncogene or tumor suppressor gene
- Mutated cell = initiated cell
- Promoters cause clonal expansion
- Accumulation of additional mutations = cancer
10. PARANEOPLASTIC SYNDROMES
Definition
Symptom complexes occurring in cancer patients that cannot be explained by:
- Local or distant spread of the tumor, OR
- Elaboration of hormones appropriate to the tissue of origin
Importance (Exam Point)
- May be the earliest manifestation of an occult/occult neoplasm
- May produce significant clinical illness (even lethal)
- May mimic metastatic disease and confound treatment
- Occur in ~10% of cancer patients
Classification with Examples (Robbins & Cotran Table 7.11)
A. Endocrinopathies (Ectopic Hormone Production)
| Syndrome | Hormone/Mediator | Associated Cancer |
|---|
| Cushing syndrome | Ectopic ACTH | Small cell lung carcinoma, Pancreatic carcinoma |
| SIADH (↓Na, ↑urine osmolality) | ADH | Small cell lung carcinoma |
| Hypercalcemia (most common) | PTHrP, TGF-α, TNF, IL-1 | Squamous cell lung carcinoma, Breast carcinoma, Renal cell carcinoma, Adult T-cell leukemia/lymphoma |
| Hypoglycemia | Insulin-like substance | Fibrosarcoma, Ovarian carcinoma |
| Polycythemia | Erythropoietin | Renal cell carcinoma, Cerebellar hemangioblastoma, HCC |
| Osteomalacia | FGF-23 | Phosphaturic mesenchymal tumor |
B. Nerve and Muscle Syndromes
| Syndrome | Associated Cancer |
|---|
| Myasthenia gravis-like | Bronchogenic carcinoma, Thymoma |
| Peripheral neuropathy | Breast carcinoma |
| Cerebellar degeneration | Lung, ovarian cancer |
| Eaton-Lambert syndrome | Small cell lung carcinoma |
C. Dermatologic Disorders
| Syndrome | Cancer | Mechanism |
|---|
| Acanthosis nigricans (velvety hyperpigmentation in axilla/neck) | Gastric, Lung, Uterine carcinoma | EGF secretion by tumor |
| Dermatomyositis | Bronchogenic, Breast carcinoma | Immunologic |
D. Osseous/Articular Changes
| Syndrome | Cancer |
|---|
| Hypertrophic osteoarthropathy + clubbing | Bronchogenic carcinoma |
E. Vascular/Hematologic Changes
| Syndrome | Cancer | Mechanism |
|---|
| Trousseau's sign (migratory thrombophlebitis) | Pancreatic carcinoma, Bronchogenic carcinoma | Tumor mucins activate clotting |
| DIC | Acute promyelocytic leukemia, Prostatic carcinoma | Tumor clotting factors |
| Nonbacterial thrombotic endocarditis | Advanced cancers | Hypercoagulability |
| Red cell aplasia | Thymoma | Immunologic |
11. TELEPATHOLOGY AND PRECANCEROUS LESIONS
Telepathology
- Digital transmission of pathologic images for remote diagnosis
- Process: Glass slide - scanned to digital format - transmitted via internet - viewed remotely by pathologist
- Types:
- Static - pre-selected images sent; quick but limited
- Dynamic (real-time) - remote control of robotic microscope; comprehensive but needs fast network
- Whole slide imaging (WSI)/Virtual microscopy - entire slide scanned at multiple magnifications; most modern approach
- Uses: Intraoperative frozen section consultation, expert second opinion, rural/underserved areas, digital pathology archives, AI integration
Precancerous Lesions (Precancerous Conditions)
Lesions with increased risk of malignant transformation:
| Lesion | Malignancy Risk |
|---|
| Leukoplakia (oral/vulvar) | Squamous cell carcinoma |
| Erythroplakia (oral) | Squamous cell carcinoma (higher risk than leukoplakia) |
| Barrett's esophagus | Adenocarcinoma of esophagus |
| Cervical dysplasia (CIN) | Cervical squamous cell carcinoma |
| Ulcerative colitis (long-standing) | Colorectal carcinoma |
| Cirrhosis | Hepatocellular carcinoma |
| Adenomatous polyps (colon) | Colorectal carcinoma |
| Atrophic gastritis | Gastric carcinoma |
| Actinic keratosis | Squamous cell carcinoma of skin |
| Paget's disease of bone | Osteosarcoma |
| Xeroderma pigmentosum | Skin cancers |
QUICK EXAM SUMMARY TABLES
Virchow's vs Sentinel Lymph Node
| Term | Definition | Example |
|---|
| Virchow's node | Left supraclavicular LN - enlarged due to metastasis via thoracic duct | Gastric carcinoma |
| Sister Mary Joseph nodule | Periumbilical nodule due to peritoneal metastasis | GI/Ovarian carcinoma |
| Krukenberg tumor | Bilateral ovarian metastasis with signet ring cells | Gastric/Colon carcinoma |
Key Differentials for Exam
Benign Neoplasm Easy Mnemonics:
- BLESS = Benign: Localized, Encapsulated, Slow-growing, Similar to normal, Seldom kills
Malignant Neoplasm:
- MIDAS = Malignant: Invasive, Differentiation (poor), Abnormal mitoses, Spreads (metastasizes), Survival (poor)
Routes of Spread - Summary
METASTASIS ROUTES
├── 1. Direct/Local invasion (all cancers)
├── 2. Lymphatic (carcinomas > sarcomas)
│ └── Regional LN → distant LN
├── 3. Hematogenous (sarcomas, RCC, HCC)
│ └── Via veins → Liver, Lungs, Brain, Bone
├── 4. Transcoelomic (peritoneal, pleural)
│ └── Ovarian Ca → peritoneum
└── 5. Perineural spread
└── Prostate Ca, Pancreatic Ca
Sources
- Robbins, Cotran & Kumar Pathologic Basis of Disease (10th Ed.) - Chapters 7 (Neoplasia), Block 3-4
- Robbins & Kumar Basic Pathology - Chapter 6 (Neoplasia)
- All images: Robbins & Cotran Pathologic Basis of Disease via medical library
MUHS Exam Tips:
- Define every term asked - neoplasia, metastasis, paraneoplastic syndrome
- Always write a table when comparing benign vs malignant
- Draw the chemical carcinogenesis diagram (initiation-promotion) - easy marks
- For oncogenic viruses - remember virus name, cancer type, and one key protein/mechanism
- Paraneoplastic: Always mention "10% of cancers," give 3-4 clinical examples, explain significance
- Lab diagnosis: Organize as histologic, IHC, molecular, tumor markers - don't mix them up
- Routes of spread: Always give an example for each route