Explain the properties of cardiac muscle For physiology 1st year MBBS
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Finding Sources
I now have comprehensive information to write a detailed, well-organized answer. Let me compose the full response.
Properties of Cardiac Muscle
Sources: Guyton & Hall Textbook of Medical Physiology, Costanzo Physiology 7th Edition, Ganong's Review of Medical Physiology 26th Edition
Overview
The heart is composed of three major types of cardiac muscle:
- Atrial muscle - thin-walled, pumps blood into ventricles
- Ventricular muscle - thick-walled, pumps blood into the circulation
- Specialized excitatory and conductive fibers (SA node, AV node, Bundle of His, Purkinje fibers) - contain few contractile fibrils; instead generate and conduct action potentials
The properties of cardiac muscle can be organized under the following headings:
1. Structural Properties (Anatomy)
Striated Appearance
Cardiac muscle is striated like skeletal muscle, with typical myofibrils containing actin and myosin filaments arranged in sarcomeres (Z line to Z line). Contraction occurs by the sliding filament mechanism - the same as skeletal muscle.
Intercalated Discs and Functional Syncytium
Cardiac muscle fibers are branching, interconnected cells separated by intercalated discs at their junctions. These discs contain:
- Desmosomes - mechanical junctions that hold cells together
- Gap junctions (nexuses) - permeable communicating junctions that allow free diffusion of ions
Because of gap junctions, an action potential spreads rapidly from cell to cell, causing the entire atrial or ventricular muscle to contract as a single unit - this is called a functional syncytium.
There are actually two separate syncytia:
- The atrial syncytium (separated from ventricles by the fibrous AV ring)
- The ventricular syncytium
The only normal electrical connection between them is the Bundle of His. This allows atria to contract slightly ahead of the ventricles, improving pumping efficiency. - Guyton & Hall, p. 122
2. Action Potential of Cardiac Muscle
The resting membrane potential of ventricular muscle is approximately -80 to -90 mV. The action potential averages about 105 mV (rises from -85 mV to +20 mV).
The most distinctive feature is its long duration (~0.2-0.3 seconds) with a plateau, compared to skeletal muscle (~1-2 ms). This is shown in the diagram below:
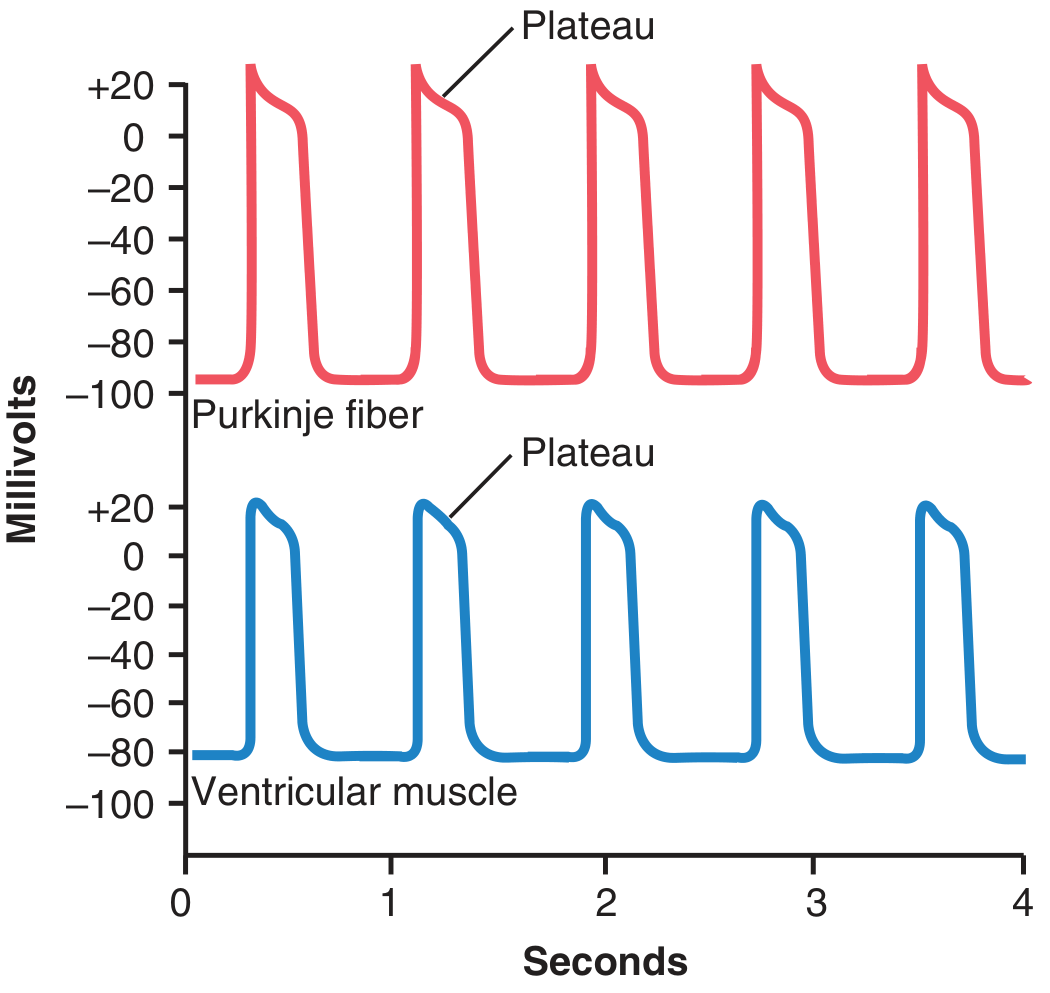
Phases of the Cardiac Action Potential
| Phase | Name | Ion Movement |
|---|---|---|
| Phase 0 | Rapid Depolarization | Fast voltage-gated Na+ channels open → massive Na+ influx; membrane rises to ~+20 mV |
| Phase 1 | Initial Rapid Repolarization | Fast Na+ channels close; K+ begins to leave via transient outward K+ channels |
| Phase 2 | Plateau | Slow L-type Ca2+ channels (calcium-sodium channels) open → sustained Ca2+ and Na2+ influx; simultaneously, K+ permeability decreases (~5-fold) preventing repolarization |
| Phase 3 | Rapid Repolarization | L-type Ca2+ channels close; slow K+ channels open → rapid K+ efflux → return to resting potential |
| Phase 4 | Resting Membrane Potential | -80 to -90 mV; maintained by Na+/K+ ATPase |
Why is there a Plateau? (Two key reasons - Guyton)
- Slow L-type Ca2+ channels open during phases 0/1 and remain open for several tenths of a second, providing sustained inward Ca2+ + Na+ current
- Decreased K+ permeability (~5-fold) during the plateau prevents early efflux of K+ that would otherwise restore the resting potential
This plateau makes ventricular contraction last up to 15 times longer than skeletal muscle contraction - essential for effective blood ejection. - Guyton & Hall, p. 123
3. Refractory Period
Because the action potential is so prolonged, the cardiac muscle has a very long refractory period:
- Absolute Refractory Period (ARP): 0.25-0.30 seconds (atria: ~0.15 sec) - no stimulus, however strong, can re-excite the muscle
- Relative Refractory Period (RRP): ~0.05 seconds additional - a very strong stimulus can excite the muscle but produces a weaker contraction
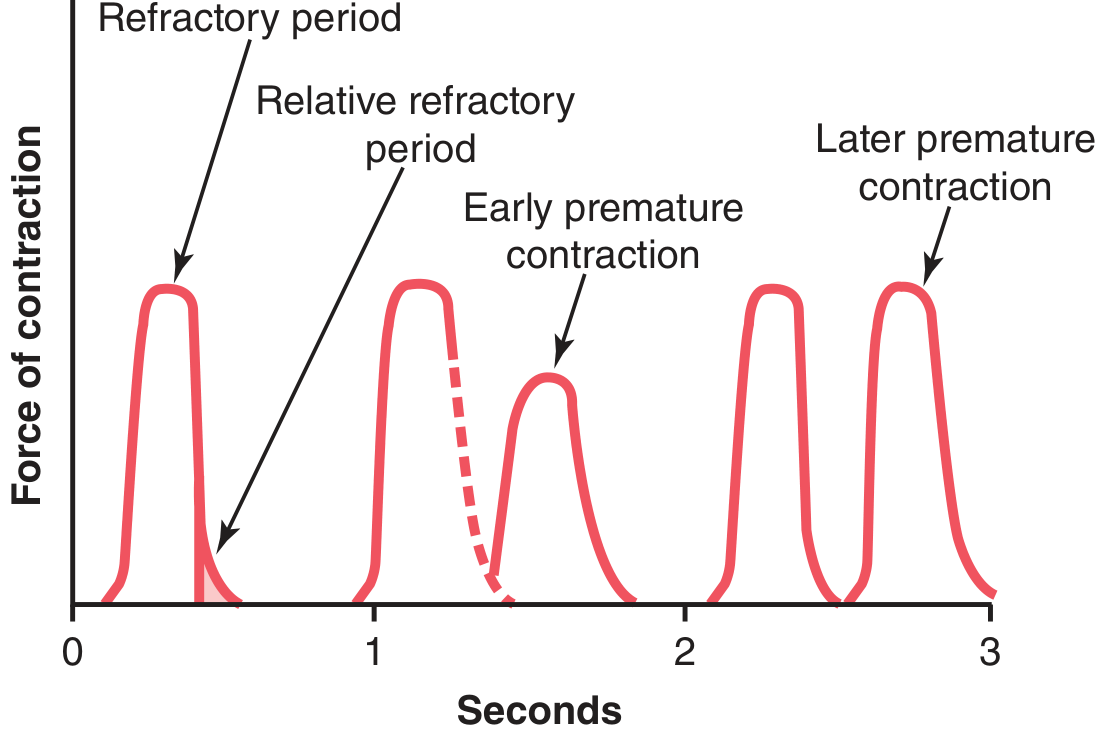
Key clinical implication: Cardiac muscle cannot undergo tetanus
The long refractory period lasts almost as long as the contraction itself (~0.3 sec). By the time the muscle can be re-excited, it has already started to relax. This prevents summation of contractions and tetanus - if the heart went into tetanus, it would stop pumping entirely. - Guyton & Hall, p. 124
4. Excitation-Contraction Coupling
This refers to how the action potential triggers mechanical contraction. The process in cardiac muscle is summarized below:
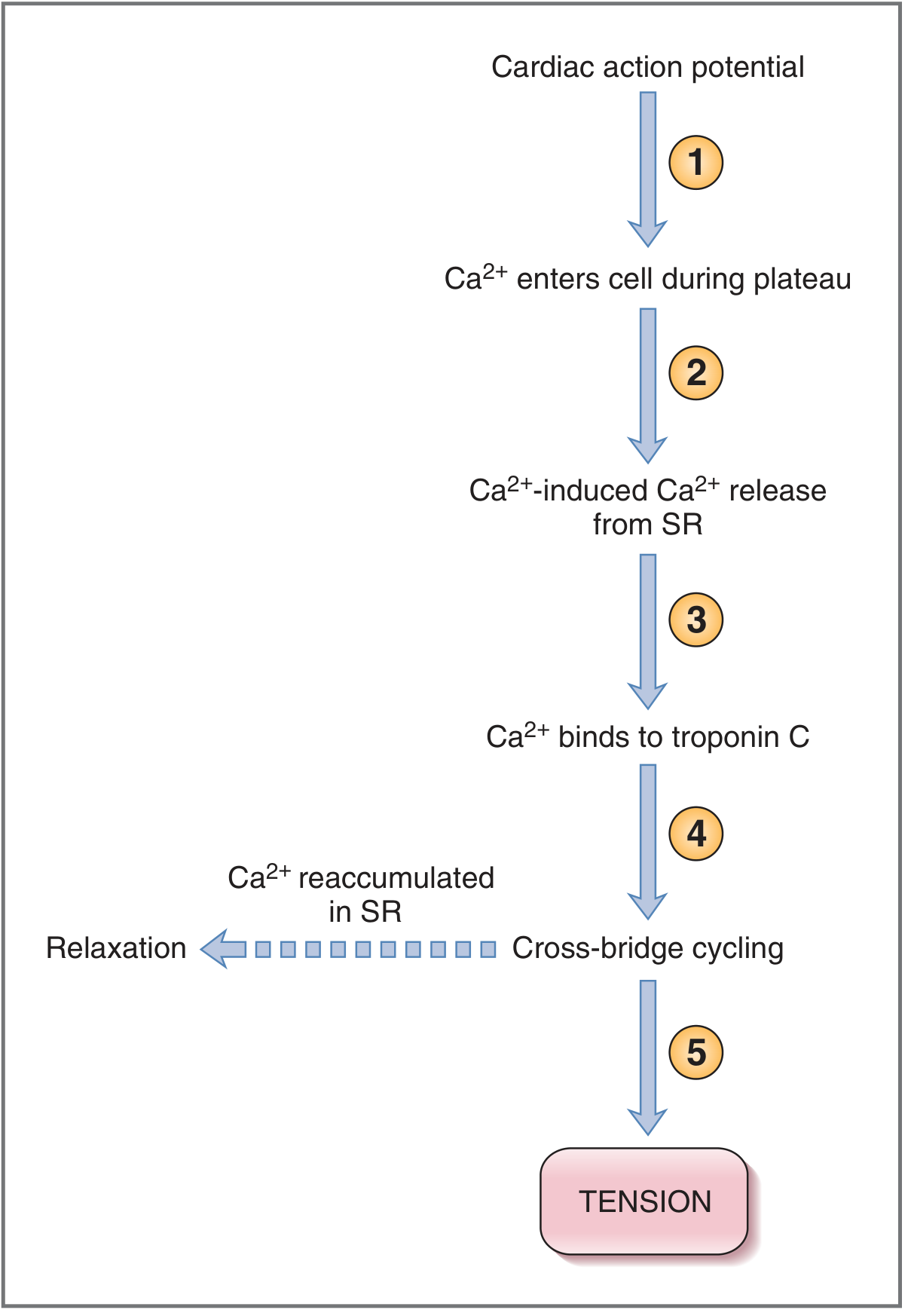
Steps:
- Action potential spreads along the sarcolemma and down the T-tubules (which invaginate at the Z-lines in cardiac muscle)
- Depolarization opens L-type (dihydropyridine) Ca2+ channels in the T-tubule membrane → Ca2+ enters from ECF (this is the trigger Ca2+)
- Trigger Ca2+ activates ryanodine receptors on the sarcoplasmic reticulum (SR) → massive Ca2+ release from SR (Ca2+-induced Ca2+ release, CICR)
- Intracellular Ca2+ rises → Ca2+ binds troponin C → conformational change removes tropomyosin inhibition → actin-myosin cross-bridge cycling → contraction
- Relaxation: Ca2+ is actively pumped back into SR by Ca2+-ATPase (SERCA); Ca2+ is also extruded from the cell by sarcolemmal Ca2+-ATPase and Na+/Ca2+ exchanger (NCX)
Key difference from skeletal muscle:
In cardiac muscle, a significant portion of the Ca2+ triggering contraction comes from extracellular sources (through L-type channels), not only from the SR. This is why extracellular Ca2+ concentration directly affects cardiac contractility. - Costanzo, p. 150
5. Contractility (Inotropism)
Contractility is the intrinsic ability of the myocardium to develop force at a given muscle cell length, independent of preload and afterload.
- Tension developed is directly proportional to intracellular Ca2+ concentration
- Positive inotropic agents (↑ contractility): catecholamines (adrenaline via β1 receptors), digoxin, Ca2+ itself
- Negative inotropic agents (↓ contractility): β-blockers, Ca2+ channel blockers, acidosis
Mechanisms to increase contractility:
- Increase Ca2+ influx during action potential plateau
- Increase SR Ca2+ stores
- Sensitize troponin C to Ca2+
- Costanzo, p. 151
6. Length-Tension Relationship (Frank-Starling Law)
Cardiac muscle obeys the Frank-Starling (Starling's) Law of the Heart: the greater the initial fiber length (end-diastolic volume = preload), the greater the force of contraction, up to a physiological optimum.
- This is the cardiac equivalent of the length-tension relationship in skeletal muscle
- Physiologically, when more blood returns to the heart (increased venous return), the ventricle is stretched more, and contracts more forcefully to eject that extra volume
- This is the intrinsic mechanism by which the heart matches output to input moment to moment
7. Automaticity (Rhythmicity)
Unlike skeletal muscle (which requires nervous stimulation), cardiac muscle has the property of automaticity - it can generate its own action potentials spontaneously. This is a property of the specialized pacemaker cells (SA node > AV node > Bundle of His > Purkinje fibers), which show spontaneous diastolic depolarization (slow upward drift of Phase 4 potential due to funny current, If, and T-type Ca2+ channels). - Ganong's, p. 522
8. Conduction Velocity
| Region | Conduction Velocity |
|---|---|
| Atrial/ventricular muscle | 0.3-0.5 m/sec |
| AV node | ~0.05 m/sec (deliberate delay) |
| Purkinje fibers | Up to 4 m/sec |
| Skeletal muscle (for comparison) | ~5 m/sec |
The slow conduction at the AV node creates a vital ~0.1 second delay, allowing atria to finish emptying into ventricles before ventricular contraction begins.
Summary Table: Cardiac vs. Skeletal Muscle
| Property | Cardiac Muscle | Skeletal Muscle |
|---|---|---|
| Striation | Yes | Yes |
| Nuclei | 1-2, central | Multiple, peripheral |
| Intercalated discs | Yes (gap junctions) | No |
| Syncytium | Functional (gap junctions) | No |
| Action potential duration | ~200-300 ms (plateau) | ~1-2 ms |
| Refractory period | ~250-300 ms (long) | ~1-2 ms (short) |
| Tetanus possible? | No | Yes |
| Ca2+ source | SR + extracellular | SR only |
| Automaticity | Yes (pacemaker cells) | No |
| Fatigue | Very resistant | Fatigues readily |
| Energy source | Aerobic (predominantly) | Aerobic + anaerobic |
Key exam points to remember:
- Cardiac muscle = functional syncytium via gap junctions in intercalated discs
- Long action potential plateau due to L-type Ca2+ channels + decreased K+ permeability
- Long refractory period → cannot tetanize → essential for pumping function
- Ca2+-induced Ca2+ release (CICR) is the key step in excitation-contraction coupling
- Contractility ∝ intracellular Ca2+
- Frank-Starling law = intrinsic preload-dependent regulation of stroke volume
- Automaticity is unique to cardiac muscle among all muscle types
This is a shared conversation. Sign in to Orris to start your own chat.