Plural effusion according to Harrison's
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive summary of Pleural Effusion from Harrison's Principles of Internal Medicine, 22nd Edition (Chapter 305 — Rebecca M. Baron):
Pleural Effusion — Harrison's 22e
Anatomy & Normal Physiology
The pleural space lies between the lung (visceral pleura) and the chest wall (parietal pleura), maintained at −3 to −5 cmH₂O by a balance between lung elastic recoil and chest wall counter-expansion. Under normal conditions:
- Fluid enters the pleural space from parietal pleural capillaries and from lung interstitium via the visceral pleura (or from the peritoneal cavity via diaphragmatic defects).
- Fluid is removed by parietal pleural lymphatics, which can absorb up to 20× the normal rate of formation.
An effusion forms when this hydrostatic-oncotic balance is disturbed and fluid formation overwhelms lymphatic drainage. ~1.5 million Americans develop a pleural effusion annually; the most common presentation is dyspnoea and occasionally pleuritic chest pain.
Diagnostic Approach
Chest imaging (CXR, CT, ultrasound) is first used to characterize extent. The critical first step is to classify the effusion as transudate vs. exudate using thoracentesis.
Light's Criteria (Exudate if ≥1 criterion met):
| Criterion | Threshold |
|---|---|
| PF protein / Serum protein | > 0.5 |
| PF LDH / Serum LDH | > 0.6 |
| PF LDH | > 2/3 upper normal serum limit |
These criteria misidentify ~25% of transudates as exudates — particularly in diuretic-treated heart failure and hepatic hydrothorax (pseudoexudates). When protein criteria are borderline, a serum-PF albumin gradient > 1.2 g/dL or serum-PF protein gradient > 3.1 g/dL can identify pseudoexudates (100% sensitivity in CHF, 99% in hepatothorax). Elevated PF cholesterol combined with elevated LDH also favors a true exudate.
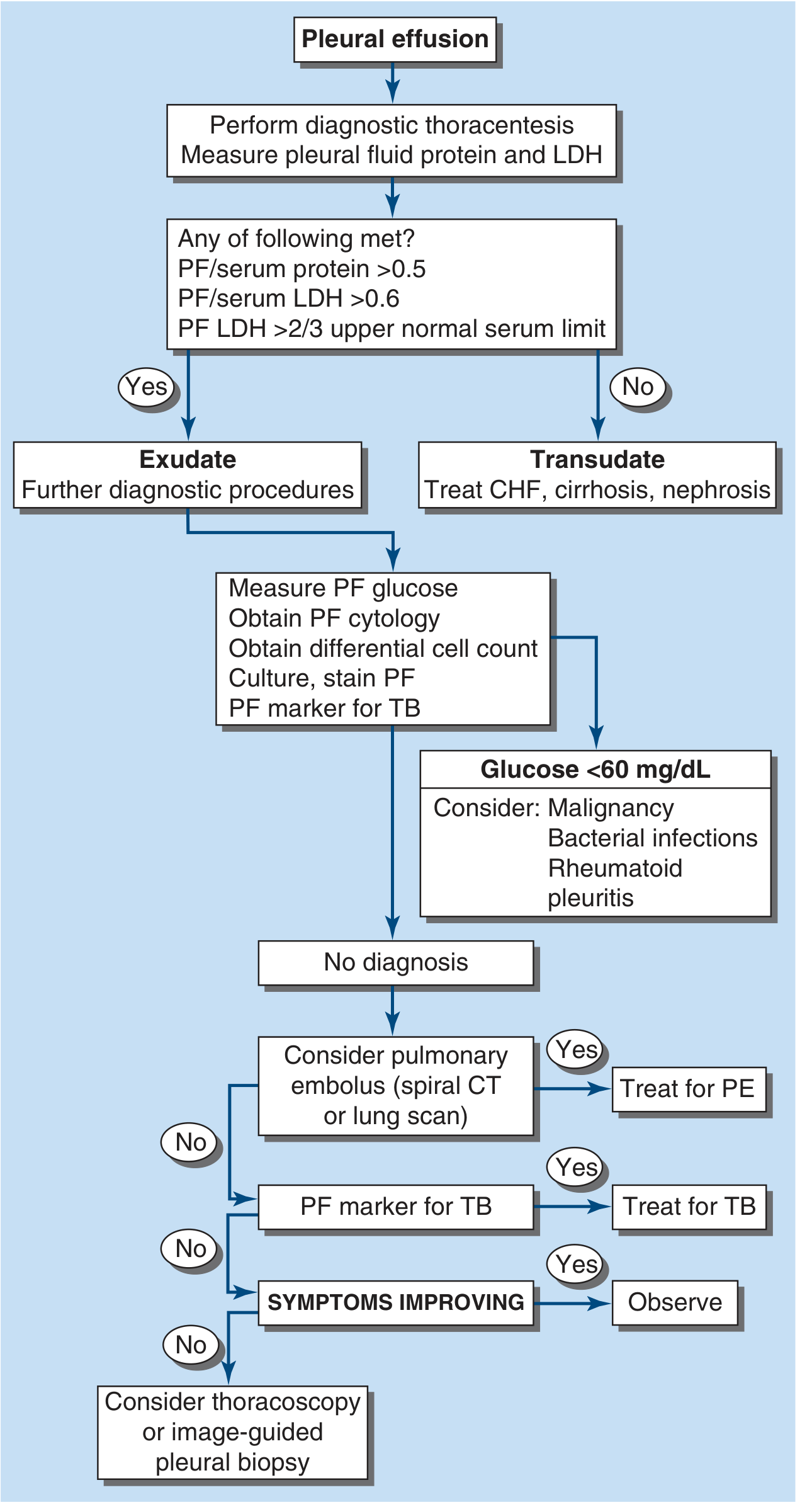
FIGURE 305-1: Diagnostic algorithm. PF = pleural fluid; CHF = congestive heart failure; LDH = lactate dehydrogenase; PE = pulmonary embolism; TB = tuberculosis.
For exudates, additionally obtain: PF glucose, differential cell count, microbiologic studies (culture/stain), cytology, and disease-specific markers (see below).
Disease-Specific PF Tests (Table 305-2):
| Suspected Disease | Test |
|---|---|
| Pancreatic disease / esophageal rupture | PF amylase |
| Drug-induced effusion | PF eosinophils |
| Congestive heart failure | PF NT-proBNP (>1500 pg/mL strongly suggests CHF) |
| Chylothorax / hemothorax | PF cholesterol + triglycerides / PF hematocrit |
| Rheumatoid disease | PF glucose and pH |
| Amyloidosis | Congo red staining |
| Lymphoma | Flow cytometry |
Causes
Transudative Effusions
- Congestive heart failure (most common cause overall)
- Cirrhosis (hepatic hydrothorax)
- Nephrotic syndrome
- Peritoneal dialysis
- Superior vena cava obstruction
- Myxedema
- Urinothorax
Exudative Effusions
Neoplastic: Metastatic disease, mesothelioma
Infectious:
- Bacterial (parapneumonic / empyema) — most common exudative cause in the US
- Tuberculosis
- Fungal, viral, parasitic
Other major causes:
- Pulmonary embolism
- GI disease: esophageal perforation, pancreatic disease, intraabdominal abscess, diaphragmatic hernia, post-abdominal surgery, endoscopic variceal sclerotherapy, post-liver transplant
- Collagen vascular disease: rheumatoid pleuritis, SLE, drug-induced lupus, Sjögren syndrome, granulomatosis with polyangiitis (Wegener's), Churg-Strauss
- Post-CABG
- Asbestos exposure
- Sarcoidosis, uremia, Meigs' syndrome, yellow nail syndrome
- Drug-induced: nitrofurantoin, dantrolene, methysergide, bromocriptine, procarbazine, amiodarone, dasatinib
- Trapped lung, radiation therapy, post-cardiac injury syndrome
- Hemothorax, chylothorax, ovarian hyperstimulation syndrome, pericardial disease
- Iatrogenic injury
Key Individual Effusion Types
1. Heart Failure (Transudate)
- Mechanism: elevated left atrial/pulmonary venous pressure → increased interstitial fluid → overwhelms parietal lymphatics.
- Thoracentesis is indicated if effusions are not bilateral/comparable in size, patient is febrile, or pleuritic chest pain is present.
- PF NT-proBNP > 1500 pg/mL supports CHF etiology.
2. Parapneumonic Effusions (PPE) / Empyema (Exudate)
- Found in up to 50% of community-acquired pneumonia; most common exudative cause in the US.
- Most PPEs are reactive (culture-negative). In ~10%, infection sets in → complicated PPE or empyema (fibrinopurulent/grossly purulent fluid).
- Aerobic bacteria: acute febrile illness, pleuritic chest pain, leukocytosis.
- Anaerobic: subacute, weight loss, mild anemia, aspiration history — may have large effusion with minimal parenchymal infiltrate.
- Free-flowing fluid confirmed by lateral decubitus CXR, CT, or ultrasound.
- Drainage indications (any of the following):
- Loculated fluid on imaging
- PF pH < 7.20 or PF glucose < 60 mg/dL
- Positive Gram stain or culture
- Gross pus (empyema)
- Options: thoracentesis, tube thoracostomy, VATS (video-assisted thoracoscopic surgery).
- Intrapleural fibrinolytics (t-PA + DNase) used for loculated/complex parapneumonic effusions.
3. Malignant Effusion (Exudate)
- Second most common cause of exudative effusion.
- Most common primaries: lung > breast > lymphoma.
- Diagnosed by PF cytology (positive in ~60%) or pleural biopsy. Thoracoscopy improves yield.
- PF glucose < 60 mg/dL and pH < 7.30 → poor prognosis, reduced pleurodesis success.
- Management: therapeutic thoracentesis, pleurodesis (talc most effective), indwelling pleural catheter (IPC) for trapped lung or recurrent effusion.
4. Tuberculous Pleuritis (Exudate)
- Lymphocyte-predominant exudate; often in young patients in endemic areas.
- Diagnosis: PF adenosine deaminase (ADA) levels, PF culture (positive in <40%), or pleural biopsy.
- Treated with standard anti-TB regimens; glucocorticoids may reduce acute symptoms.
5. Pulmonary Embolism (Exudate or Transudate)
- Present in up to 30% of PE cases; usually small.
- Can be transudative or exudative.
- Diagnosis with CT pulmonary angiography or V/Q scan.
6. Hepatic Hydrothorax (Transudate)
- Cirrhosis with ascites → fluid migrates through diaphragmatic defects → usually right-sided.
- Diagnosed by injecting Tc-99m sulfur colloid intraperitoneally — if detected in pleural space, confirms hepatic hydrothorax.
- Treatment: sodium restriction, diuretics, TIPS; recurrent cases may need IPC.
7. Chylothorax
- Milky fluid; PF triglycerides > 110 mg/dL confirms diagnosis.
- Causes: thoracic duct disruption (trauma, surgery, malignancy).
- Treatment: low-fat diet/TPN, octreotide, surgical ligation/pleurodesis.
Management Summary
| Situation | Action |
|---|---|
| Transudate | Treat underlying cause (CHF, cirrhosis, nephrosis) |
| Exudate — no diagnosis | CT pulmonary angiography (PE?), ADA/TB markers |
| Still no diagnosis, symptoms worsening | Thoracoscopy or image-guided pleural biopsy |
| Complicated PPE / empyema | Drainage + antibiotics ± fibrinolytics (t-PA/DNase) |
| Malignant effusion, recurrent | Pleurodesis (talc) or indwelling pleural catheter |
| Hepatic hydrothorax | Diuretics, Na restriction; TIPS if refractory |
— Harrison's Principles of Internal Medicine, 22nd Edition, Chapter 305 (Rebecca M. Baron), pp. 2310–2316
Examination of pleural effusion, classical signs in inspection, palpation, percussion and auscultation.
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
I now have comprehensive data from Harrison's and supporting authoritative sources. Here is the complete structured answer:
Physical Examination of Pleural Effusion
(Sources: Harrison's 22e Ch. 305; Rosen's Emergency Medicine 9e; Textbook of Family Medicine 9e; Washington Manual of Medical Therapeutics)
Symptoms (Pre-examination Context)
- Small effusions (<500 mL) are often asymptomatic
- Dyspnoea — the cardinal symptom, typically appearing once fluid exceeds ~500 mL
- Pleuritic chest pain — sharp, worse on inspiration; or referred pain to the ipsilateral shoulder
- With massive effusions (>1.5–2 L): haemodynamic compromise, orthopnoea, inability to lie flat
1. INSPECTION
| Finding | Detail |
|---|---|
| Respiratory distress | Tachypnoea, use of accessory muscles in large effusions |
| Lag on the affected side | The ipsilateral hemithorax shows reduced expansion on inspiration — the single most sensitive clinical sign |
| Bulging of the chest wall | Seen in massive effusions — the intercostal spaces may be widened/full rather than retracted |
| Trachea/mediastinal shift | In large effusions: trachea and apex beat displaced away from the affected side (mass effect of fluid) — distinguishes from atelectasis where they shift toward |
| Hypotension / raised JVP | In tension hydrothorax (rare) — haemodynamic compromise from mediastinal compression |
The examination finding that best correlates with presence of a pleural effusion is asymmetric chest wall expansion (lag on affected side). — Washington Manual
2. PALPATION
| Finding | Detail |
|---|---|
| Decreased / absent tactile (vocal) fremitus | Fluid dampens transmission of vibration from the lung to the chest wall — key differentiator from consolidation (where fremitus is increased) |
| Reduced chest wall expansion | Felt by placing both hands on the lower chest — ipsilateral side moves less |
| Tracheal deviation | Palpable shift of the trachea away from the side of a large effusion |
| Apex beat displacement | Shifted away from the effusion in large/tension effusions |
| Intercostal space fullness | Bulging felt on palpation in massive effusions |
3. PERCUSSION
| Finding | Detail |
|---|---|
| Stony dullness | The hallmark of pleural effusion — a flat/stony dull note over the fluid, duller than the dullness of consolidation |
| Distribution | Starts at the lung base, extends upward; small/moderate effusions show dullness at the base posteriorly |
| Damoiseau's (Ellis-Damoiseau) line | The upper border of dullness forms a curved line — highest in the axilla, lower medially and laterally — due to fluid meniscus effect |
| Traube's space obliteration | Left-sided effusions obliterate the gastric tympanic area |
| Grocco's triangle | Paravertebral resonance on the contralateral side — a triangular area of dullness next to the spine on the opposite side, caused by mediastinal displacement |
| Shifting dullness | The dullness shifts with position (lateral decubitus) — confirms free fluid vs. fixed consolidation |
| Upper border: resonance or hyperresonance | Just above the effusion, compressed atelectatic lung may give relative resonance |
"Auscultatory percussion" (percussing while listening with the stethoscope) may be more sensitive and specific for detecting pleural effusion than standard percussion alone. — Rosen's
4. AUSCULTATION
| Finding | Detail |
|---|---|
| Diminished / absent breath sounds | Over the fluid — reduced air entry as fluid attenuates sound transmission |
| Decreased vocal resonance / absent bronchophony | Voice sounds muffled or absent over the effusion |
| Egophony ("E-to-A" change) | At the superior border of the effusion — patient says "eeee" but clinician hears "aaaa"; due to the underlying compressed/atelectatic lung at the fluid–air interface. Absent over the bulk of the effusion |
| Enhanced / bronchial breath sounds | At the upper border of the effusion (over compressed atelectatic lung) — a narrow band of bronchial character may be heard |
| Pleural friction rub | May be present in pleurisy without effusion, or at the margins; disappears once fluid separates the pleural layers |
| Absent adventitial sounds (crackles/wheeze) | The fluid zone itself is silent — distinguishes from consolidation (which has crackles) |
Comparison Table: Classical Physical Signs
| Pleural Effusion (Large) | Consolidation (Pneumonia) | Pneumothorax | Atelectasis | |
|---|---|---|---|---|
| Inspection | Lag, bulging intercostals, trachea shifted away | Possible lag/splinting | Lag, trachea shifted away | Lag, trachea shifted toward |
| Palpation (fremitus) | Decreased / absent | Increased | Absent | Decreased |
| Percussion | Stony dull / flat | Dull | Hyperresonant/tympanitic | Dull/flat |
| Auscultation | Absent breath sounds ± egophony at upper border | Bronchial, crackles, bronchophony | Absent breath sounds | Absent breath sounds |
(Table adapted from Hinshaw & Murray, as cited in Textbook of Family Medicine 9e, Table 16-2)
Key Differentiating Points
- Effusion vs. Consolidation: The critical distinction is fremitus — decreased in effusion, increased in consolidation. Egophony is localised to the upper border of the effusion (not throughout), whereas in consolidation it is present throughout the consolidated area.
- Effusion vs. Atelectasis: Both cause dullness and absent breath sounds, but in atelectasis the trachea/mediastinum shifts toward the affected side; in effusion it shifts away.
- >200 mL of fluid is needed before physical signs become detectable; imaging (CXR, ultrasound, CT) is more sensitive for smaller volumes.
— Harrison's Principles of Internal Medicine 22e, Ch. 305 (p. 2310); Rosen's Emergency Medicine 9e, Ch. 63; Textbook of Family Medicine 9e, Ch. 16; Washington Manual of Medical Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.