About blood pressure and its clinical aspects
Reading File
Finding Sources
Finding Sources
Searching PubMed
"blood pressure" AND "hypertension"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content and excellent diagrams. Let me compose the full, detailed clinical answer.
Blood Pressure: Physiology and Clinical Aspects
1. Definition and Units
Blood pressure (BP) is the force exerted by circulating blood against the walls of blood vessels, expressed in millimeters of mercury (mm Hg). The mercury manometer has been the standard reference since its invention by Poiseuille in 1846. A pressure of 100 mm Hg means sufficient force to raise a column of mercury 100 mm against gravity. It can also be expressed in cm H₂O (1 mm Hg = 1.36 cm H₂O), which is relevant for measuring central venous and cerebrospinal fluid pressures.
- Guyton and Hall Textbook of Medical Physiology, p. 2075
2. Physiological Determinants
The fundamental equation governing blood pressure is:
BP = Cardiac Output (CO) × Peripheral Vascular Resistance (PVR)
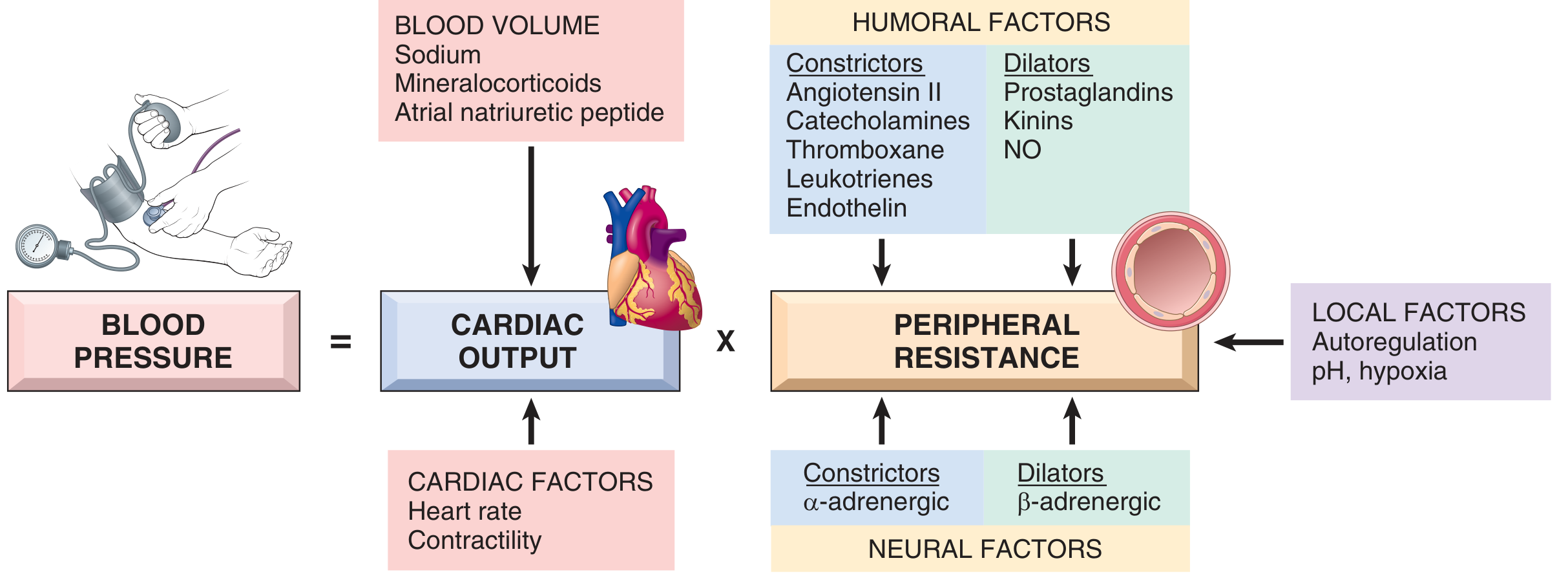
Fig. 8.2 - Blood pressure regulation (Robbins & Kumar Basic Pathology)
Cardiac Output
- CO = Heart Rate × Stroke Volume
- The most important determinant of stroke volume is filling pressure, regulated through sodium homeostasis and blood volume
- Heart rate and myocardial contractility are controlled by α- and β-adrenergic systems
Peripheral Vascular Resistance
-
Regulated predominantly at the arteriolar level by neural and humoral inputs
-
Vascular tone = balance between:
- Vasoconstrictors: Angiotensin II, catecholamines, endothelin, thromboxane, leukotrienes
- Vasodilators: Kinins, prostaglandins, nitric oxide (NO)
-
Blood vessels exhibit autoregulation: increased flow triggers vasoconstriction to protect tissues from hyperperfusion
-
Fine-tuned by local tissue pH and hypoxia
-
Robbins & Kumar Basic Pathology, p. 2501-2512
3. Anatomic Sites of BP Control
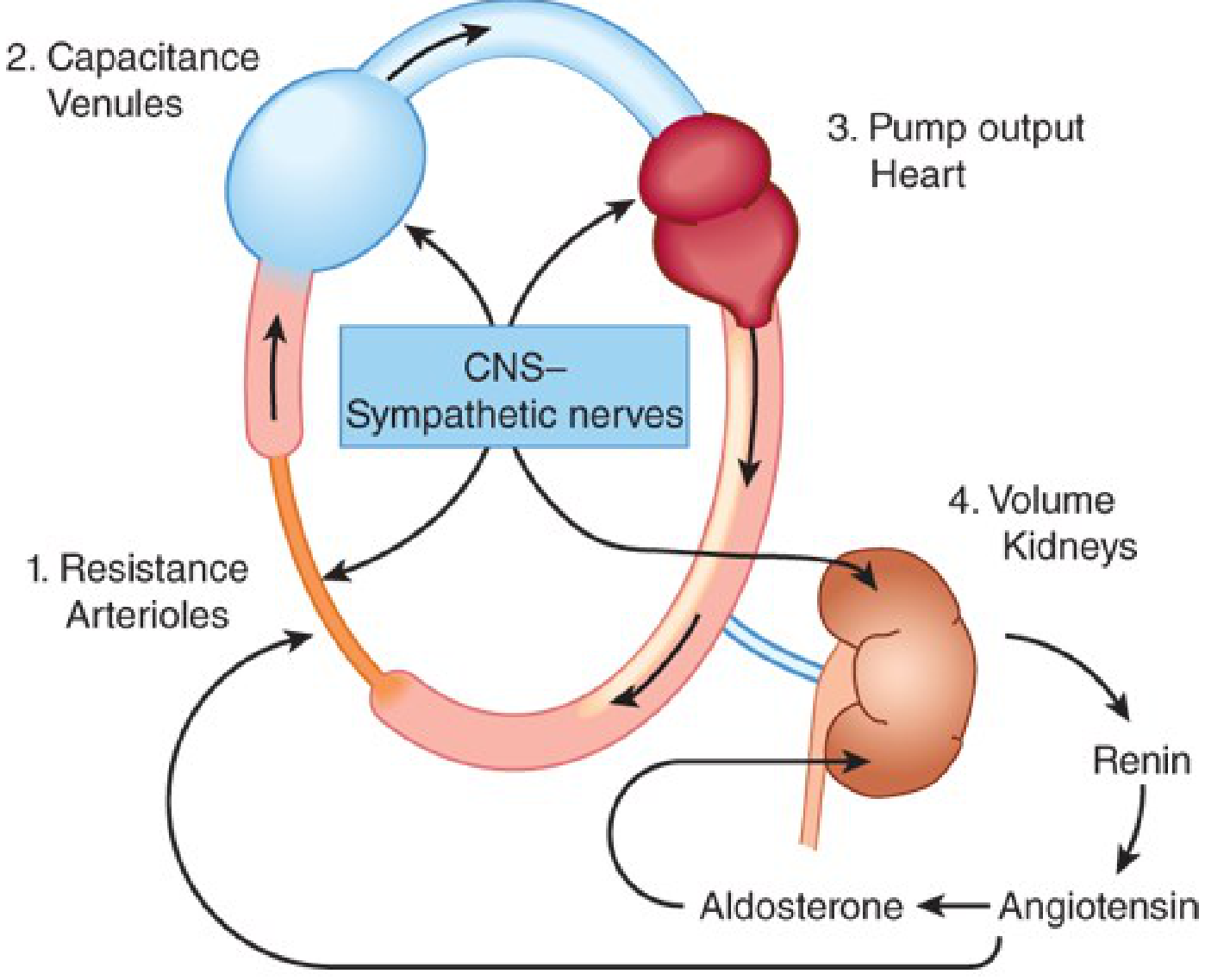
Fig. 11-1 - Anatomic sites of blood pressure control (Katzung's Basic and Clinical Pharmacology, 16e)
Katzung identifies four major anatomic sites of BP control:
- Resistance arterioles - primary site of peripheral vascular resistance
- Capacitance venules - regulate venous return and preload
- Heart (pump output) - cardiac output
- Kidneys (volume control) - via the renin-angiotensin-aldosterone system
All are coordinated by the CNS-sympathetic nervous system.
- Katzung's Basic and Clinical Pharmacology, 16e, p. 2905
4. Regulatory Mechanisms
A. Baroreceptor Reflex (Short-term)
Carotid baroreceptors sense arterial wall stretch. With a fall in BP (e.g., standing up):
- Baroreceptor activation decreases → sympathetic discharge increases
- Reflex responses: arteriolar constriction (↑ PVR), venoconstriction (↑ venous return), and cardiac stimulation (↑ CO)
- This rapid, moment-to-moment system is responsible for postural BP homeostasis
In hypertensive patients, both baroreceptors and the renal pressure-volume control systems are "set" at a higher pressure level - this is why antihypertensives work by interfering with these same normal mechanisms.
- Katzung's Basic and Clinical Pharmacology, 16e, p. 2908-2910
B. Renin-Angiotensin-Aldosterone System (Long-term)
-
Juxtaglomerular cells of the kidney release renin in response to low renal perfusion pressure or low distal tubular sodium
-
Renin cleaves angiotensinogen → angiotensin I → ACE converts to angiotensin II (Ang II)
-
Ang II is the key effector: ~40× more potent than norepinephrine as a pressor agent
-
Ang II actions:
- Direct arteriolar vasoconstriction
- Stimulates aldosterone release → sodium and water retention → increases blood volume
- Acts on CNS to reset the baroreceptor reflex to higher pressure
- Stimulates sympathetic ganglia and adrenal medulla (epinephrine/norepinephrine release)
- Is mitogenic for vascular and cardiac muscle (mediates hypertensive remodeling)
-
Atrial natriuretic peptide (ANP) counteracts this system by promoting sodium excretion in response to volume overload
-
Katzung's Basic and Clinical Pharmacology, 16e, p. 323-350
-
Robbins & Kumar Basic Pathology, p. 2516-2520
C. Sodium Homeostasis
The kidneys filter ~170 L of plasma and 23 moles of salt daily. Net sodium balance is tightly controlled by aldosterone acting on ENaC (epithelial sodium channel) in the collecting duct. Sodium retention → expanded plasma volume → ↑ CO → ↑ BP.
5. BP Measurement
Clinical Auscultatory Method
- Korotkoff sounds heard during cuff deflation
- Systolic BP = first Korotkoff sound
- Diastolic BP = disappearance of sounds (Phase V)
- White coat hypertension: alerting reaction causes BP rise during physician measurement
Home Blood Pressure Monitoring (HBPM)
- Proper technique is mandatory; average home BP goal is <135/85 mm Hg
Ambulatory Blood Pressure Monitoring (ABPM)
- 24-hour average goal: <130/80 mm Hg
- ABPM is the gold standard to rule out white coat hypertension and detect masked hypertension
High-Fidelity Methods
For rapidly changing pressures, electronic pressure transducers are used (capacitance, inductance, or resistance wire types), capable of recording pressure cycles up to 20-500 Hz - used in invasive arterial monitoring (arterial lines, cardiac catheterization).
- Guyton & Hall, p. 2079-2104
- Textbook of Family Medicine, 9e, p. 3210
6. Normal Values and Classification
| Category | Systolic (mm Hg) | Diastolic (mm Hg) |
|---|---|---|
| Normal | <120 | <80 |
| Elevated (Prehypertension) | 120-129 | <80 |
| Stage 1 Hypertension | 130-139 | 80-89 |
| Stage 2 Hypertension | ≥140 | ≥90 |
| Hypertensive Crisis | >180 | >120 |
In children, hypertension is defined as average SBP or DBP ≥95th percentile for age, gender, and height on 3 or more occasions; prehypertension is ≥90th percentile.
- Textbook of Family Medicine, 9e, p. 2456
7. Hypertension: Clinical Aspects
Epidemiology
- Affects approximately one third of the adult population
- Only ~50% of hypertensive patients achieve BP goals in the US
- Leading modifiable risk factor for stroke, heart attack, heart failure, and CKD
Causes
- Primary (essential) hypertension: ~95% of cases; polygenic, no single identifiable cause; influenced by genetics, salt intake, obesity, stress, and the RAAS
- Secondary hypertension (~5%): identifiable causes include:
- Renovascular hypertension (renal artery stenosis)
- Primary hyperaldosteronism (Conn syndrome)
- Pheochromocytoma
- Cushing syndrome
- Obstructive sleep apnea
- Coarctation of the aorta
- Drug-induced (NSAIDs, OCPs, stimulants, decongestants)
Hypertension as a Risk Factor
-
Peripheral arterial disease (PAD): 2.5-fold age-adjusted risk in men, 3.9-fold in women
-
Stroke, coronary artery disease, heart failure, CKD
-
Each 20 mmHg rise in systolic (or 10 mmHg in diastolic) above 115/75 mm Hg doubles cardiovascular mortality risk (data from 1 million adults across 61 prospective studies - Lewington et al.)
-
Textbook of Family Medicine, 9e, p. 974
8. Treatment of Hypertension
BP Targets
- General population <60 years: <140/90 mm Hg
- Age >60 years (JNC 8): <150/90 mm Hg; most other guidelines prefer <140/90 mm Hg in this group too
- Diabetics/CKD with significant proteinuria (>500 mg/day): <130/80 mm Hg may offer additional renal protection
- Home BP goal: <135/85 mm Hg | 24-hour ABPM goal: <130/80 mm Hg
Lifestyle Modifications (first-line for all)
- Dietary sodium restriction
- Weight reduction (DASH diet)
- Regular aerobic exercise
- Limiting alcohol
- Smoking cessation
Drug Therapy
First-line agents (for uncomplicated essential hypertension):
- Thiazide/thiazide-like diuretics (chlorthalidone preferred over hydrochlorothiazide)
- ACE inhibitors (e.g., lisinopril, ramipril)
- Angiotensin receptor blockers (ARBs, e.g., losartan, irbesartan)
- Calcium channel blockers (CCBs, e.g., amlodipine)
Combination therapy: If BP is >20/10 mm Hg above target, start two agents simultaneously. Evidence from the ACCOMPLISH trial supports ACE inhibitor + CCB (amlodipine) as the optimal two-drug combination. ~75% of patients will require two or more medications.
Avoid combining two RAAS blockers (e.g., ACE inhibitor + ARB) - almost always contraindicated.
Compelling Indications (JNC 7) - Drug Selection by Comorbidity
| Condition | Diuretic | β-Blocker | ACE Inhibitor | ARB | CCB | MRA |
|---|---|---|---|---|---|---|
| Heart failure | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Post-MI | ✓ | ✓ | ✓ | |||
| CAD risk | ✓ | ✓ | ✓ | ✓ | ||
| Diabetes mellitus | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Renal disease | ✓ | ✓ | ||||
| Recurrent stroke prevention | ✓ | ✓ |
ACE = angiotensin-converting enzyme; ARB = angiotensin receptor blocker; CCB = calcium channel blocker; MRA = mineralocorticoid receptor antagonist
- Textbook of Family Medicine, 9e, p. 3453-3464
Resistant Hypertension
- Defined as BP above goal on ≥3 antihypertensive medications (including a diuretic)
- Affects ~10% of the hypertensive population
- Empirical use of spironolactone (2.5-50 mg/day) has demonstrated efficacy as add-on therapy
- CPAP therapy helps in resistant hypertension with obstructive sleep apnea (HIPARCO trial)
9. Hypotension and Shock
Clinical Importance of Hypotension
- Hypotension is one of the last signs of shock
- Children and fit young adults can maintain BP until the final stages of shock through increased stroke volume and vasoconstriction - they can be in profound shock with a "normal" BP
- Elderly patients who are chronically hypertensive may be hypotensive at "normal" population values (e.g., 120/80 in a patient whose usual BP is 160/90)
- Beta-blockers or other medications may prevent the expected tachycardic response, masking the diagnosis
Hypertension in Heart Failure (AHF)
-
Most patients with acute heart failure present with elevated BP and benefit from vasodilator therapy
-
In AHF with pulmonary edema, vasodilators (nitroglycerin, nitroprusside) are primary therapy
-
SBP <85-90 mm Hg or peripheral hypoperfusion are poor prognostic signs in AHF
-
IV catecholamines (dopamine, dobutamine, norepinephrine) carry increased in-hospital mortality risk and should be used only when necessary
-
Braunwald's Heart Disease, p. 3078-3080
-
Bailey and Love's Surgery, 28e, p. 1003-1013
10. Special Populations
Pregnancy
A 2025 network meta-analysis in the American Journal of Obstetrics and Gynecology (PMID: 40216176) reviewed oral antihypertensives in pregnancy; this is an active area where treatment selection requires particular care.
Older Adults
A 2024 Cochrane meta-analysis (PMID: 39688187) examined whether higher BP targets (e.g., <150/90 rather than <140/90) are appropriate in older adults - still a matter of clinical debate.
Recent Evidence Update (2025)
A landmark Lancet meta-analysis (PMID: 40885583) systematically reviewed BP-lowering efficacy of antihypertensive drugs and combinations from randomized placebo-controlled trials, providing updated comparative evidence for drug selection.
Summary
| Concept | Key Fact |
|---|---|
| BP equation | CO × PVR |
| Normal | <120/80 mm Hg |
| Stage 2 HTN | ≥140/90 mm Hg |
| Most common type | Primary/essential (~95%) |
| Best 2-drug combo | ACE inhibitor + amlodipine (ACCOMPLISH) |
| Long-term BP controller | Kidneys (RAAS + sodium) |
| Short-term BP controller | Baroreceptor reflex |
| Shock caveat | BP normal until very late in young/fit patients |
Sources: Robbins & Kumar Basic Pathology | Katzung's Basic & Clinical Pharmacology, 16e | Guyton & Hall Textbook of Medical Physiology | Braunwald's Heart Disease | Textbook of Family Medicine, 9e | Bailey and Love's Surgery, 28e
This is a shared conversation. Sign in to Orris to start your own chat.