Hey tell me about emphysema form basics to clinical
Reading File
Finding Sources
Finding Sources
Searching PubMed
"emphysema"[MeSH Terms] AND ("pathophysiology" OR "treatment")
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Emphysema: From Basics to Clinical
1. Definition
Emphysema is defined as permanent, irreversible enlargement of the airspaces distal to the terminal bronchiole, accompanied by destruction of alveolar walls, without significant fibrosis. Unlike chronic bronchitis, which is defined clinically, emphysema is an anatomic diagnosis.
- Robbins & Kumar Basic Pathology, p. 448
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 634
2. Anatomy Primer: The Acinus
The fundamental lung unit is the acinus - the structure distal to the terminal bronchiole. It includes:
- Respiratory bronchioles
- Alveolar ducts
- Alveolar sacs and alveoli
A cluster of 3-5 acini forms a lobule. Understanding which part of the acinus is destroyed defines the type of emphysema.
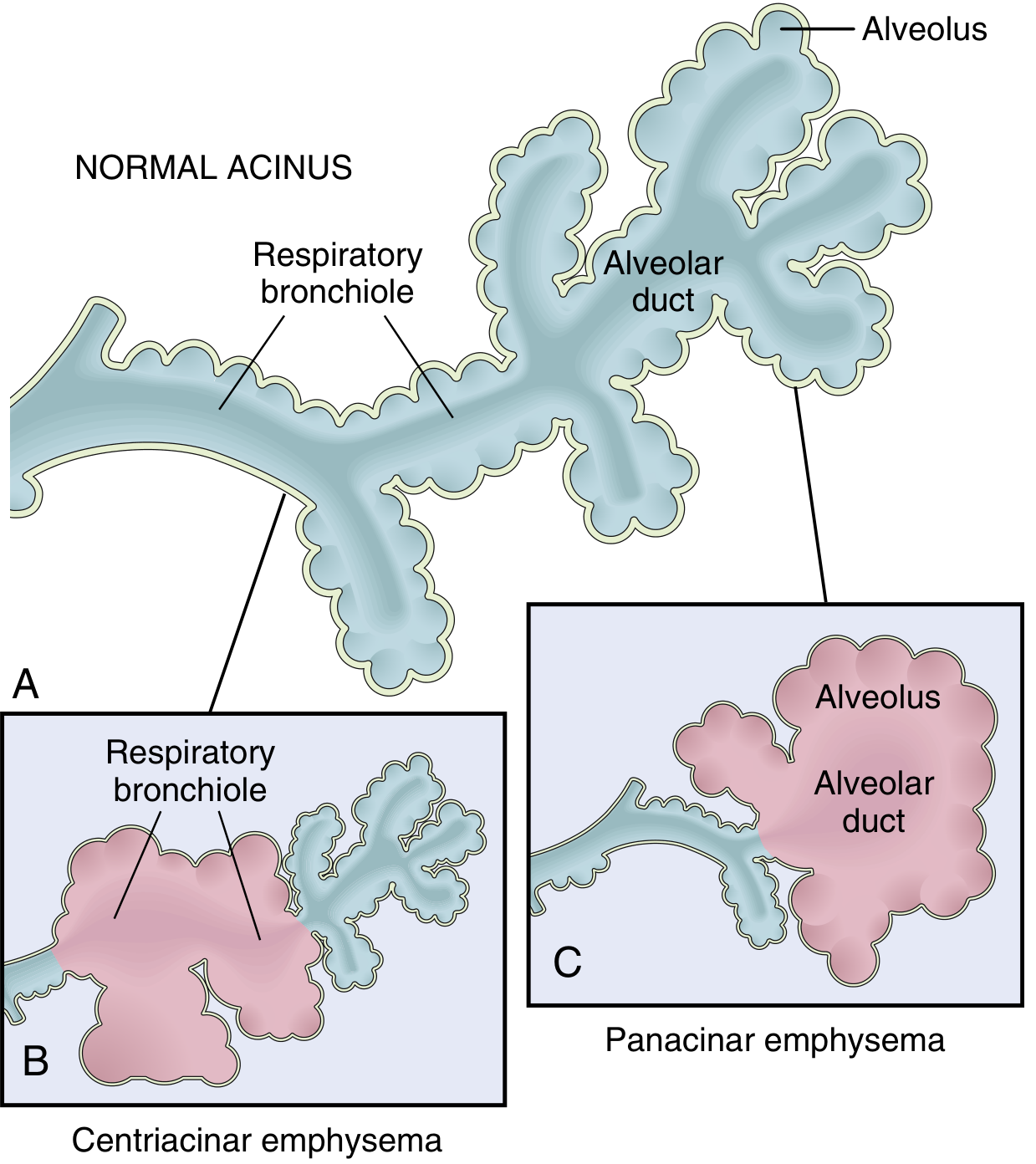
3. Classification / Types of Emphysema
There are four anatomic types. Only the first two cause clinically significant airflow obstruction:
(A) Centriacinar (Centrilobular) Emphysema
- Most common type - >95% of clinically significant cases
- Destruction of the central/proximal parts of the acinus (respiratory bronchioles), with sparing of distal alveoli
- Both emphysematous and normal airspaces coexist in the same lobule
- Distribution: Upper lobes, apical segments predominate
- Cause: Almost exclusively in cigarette smokers, often with concurrent chronic bronchitis
- The "classic" smoking-related emphysema
(B) Panacinar (Panlobular) Emphysema
- Uniform destruction from respiratory bronchiole all the way to the terminal alveoli - the entire acinus is enlarged
- Distribution: Lower lobes predominate; anterior margins
- Cause: Strongly associated with α1-antitrypsin (A1AT) deficiency; exacerbated by smoking
- ZZ homozygotes for the Pi locus on chromosome 14 have very low A1AT serum levels; >80% of ZZ individuals develop symptomatic panacinar emphysema
(C) Distal Acinar (Paraseptal) Emphysema
- Proximal acinus is normal; distal portion is primarily involved
- Located near the pleura, along lobular connective tissue septa, near areas of scarring or atelectasis
- More severe in upper lung halves
- Creates enlarged airspaces up to >2 cm and bullae
- Clinical relevance: Classically presents as spontaneous pneumothorax in young adults
(D) Irregular (Paracicatricial) Emphysema
- Acinus is irregularly involved, almost always associated with scarring
- Clinically insignificant in most cases
4. Pathogenesis
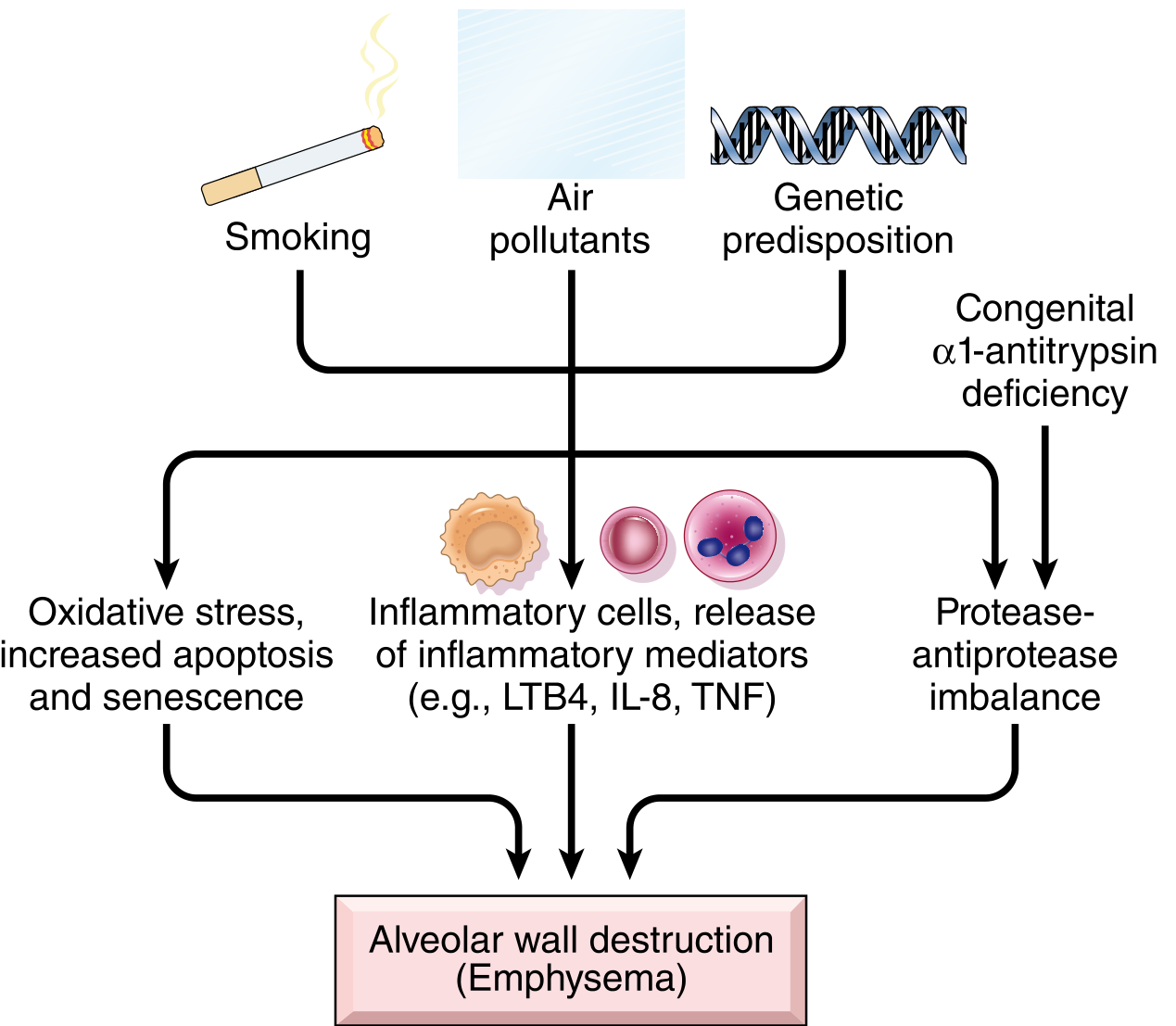
Three key mechanisms work together:
(i) Toxic Injury & Inflammation
- Inhaled cigarette smoke damages respiratory epithelium and recruits inflammatory cells
- Resident macrophages and epithelial cells release mediators: LTB4, IL-8, TNF, and others
- This triggers chemotaxis of neutrophils and macrophages to the lung
- Chronic inflammation leads to accumulation of T and B lymphocytes
(ii) Protease-Antiprotease Imbalance (the central mechanism)
- Neutrophils and macrophages release elastase and other proteases that degrade connective tissue, particularly elastin in alveolar walls
- Normally, α1-antitrypsin (A1AT) inhibits these elastases
- In emphysema, there is a relative deficiency of antiproteases - either acquired (in smokers) or genetic (A1AT deficiency)
- Loss of elastin = loss of radial traction on respiratory bronchioles → bronchiolar collapse on expiration → functional airflow obstruction without mechanical blockage
(iii) Oxidative Stress
-
Tobacco smoke and inflammatory cells generate reactive oxygen species (ROS)
-
ROS cause direct tissue damage and worsen the antiprotease deficit (oxidants inactivate A1AT)
-
The NRF2 pathway (encoded by NFE2L2) normally counteracts oxidants; genetic variants in this pathway increase susceptibility to smoking-related lung disease
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 636
5. Morphology (Gross & Histology)
Gross:
- Advanced emphysema: voluminous, pale lungs that overlap the heart anteriorly and flatten the diaphragm
- Panacinar: pale, very voluminous
- Centriacinar: deeper pink, upper 2/3 more severely affected; less voluminous until late
- Apical blebs and bullae (spaces >1 cm) may be present, especially in irregular emphysema
Histology:

- Abnormally large alveoli separated by thin septa
- Destruction of alveolar walls without fibrosis (key distinguishing feature)
- Decreased capillary bed (loss of alveolar capillaries)
- Pores of Kohn enlarged - septa appear "floating" or protrude club-shaped into air spaces
- Terminal/respiratory bronchioles deformed due to loss of anchoring septa
- Bronchiolar inflammation and submucosal fibrosis in advanced disease
6. Pathophysiology of Airflow Obstruction
The mechanisms of obstruction are functional, not mechanical:
- Loss of elastic recoil - destruction of elastin in alveolar walls removes the radial traction that normally holds small airways open
- Bronchiolar collapse during expiration - without radial traction support, respiratory bronchioles collapse on expiration → air trapping and hyperinflation
- Loss of capillary bed → reduced diffusion capacity → hypoxemia (late)
- Pulmonary hypertension - from hypoxia-induced vascular spasm + loss of capillary surface area → right heart strain → cor pulmonale
7. Clinical Features
Symptoms
- Dyspnea is the first and most prominent symptom; begins insidiously and is steadily progressive
- In chronic bronchitis-predominant COPD: cough and wheezing may precede dyspnea
- Weight loss can be prominent (increased work of breathing, reduced appetite)
Classic Physical Examination - the "Pink Puffer"
Pure emphysema patients classically present as:
- Barrel chest (increased anterior-posterior diameter due to hyperinflation)
- Pursed-lip breathing during expiration (auto-PEEP to prevent airway collapse)
- Sitting hunched forward (tripod position)
- Prolonged expiration
- Pink skin (relatively preserved oxygenation until late stages)
- Hyperresonant chest on percussion
- Reduced breath sounds, quiet chest
Contrast this with the "Blue Bloater" phenotype of predominant chronic bronchitis - cyanotic, overweight, productive cough, hypercarbic, prone to cor pulmonale.
Pulmonary Function Tests (PFTs)
| Parameter | Finding in Emphysema |
|---|---|
| FEV1 | Reduced |
| FVC | Normal or near-normal |
| FEV1/FVC ratio | Reduced (<0.70 - the hallmark of obstruction) |
| TLC | Increased (air trapping, hyperinflation) |
| RV | Increased |
| DLCO | Decreased (loss of capillary bed = reduced diffusion surface) |
A reduced DLCO is particularly characteristic of emphysema and helps distinguish it from asthma (where DLCO is normal).
Blood Gases
- Early/mild disease: relatively normal ABGs (hyperventilation compensates)
- Late/severe disease: hypoxemia, eventually hypercapnia and respiratory acidosis
- Until very late, many emphysema patients maintain adequate gas exchange due to increased respiratory drive
Imaging
- CXR: Hyperinflated lungs, flattened diaphragm (the classic sign), increased retrosternal air space, hyperlucency, small heart
- CT chest: Gold standard for assessing type and extent of emphysema; can show bullae, cysts, and distribution (upper vs. lower lobe predilection)
8. Complications
| Complication | Mechanism |
|---|---|
| Cor pulmonale | Pulmonary HTN from hypoxia + capillary loss → right heart failure (20-30% of patients) |
| Pneumothorax | Rupture of bullae (especially paraseptal type) |
| Respiratory failure | Loss of functional lung + exacerbation by infection |
| Polycythemia | Secondary to chronic hypoxemia |
| Obstructive sleep apnea | Comorbid in 10-30%; mechanisms incompletely understood |
9. Other Forms (Non-COPD Emphysema)
| Type | Description |
|---|---|
| Compensatory hyperinflation | Alveolar dilation compensating for lung loss (e.g., post-lobectomy) - not true emphysema |
| Obstructive overinflation | Air trapping due to subtotal airway obstruction (tumor, foreign body) - reversible |
| Bullous emphysema | Large subpleural bullae (>1 cm); can rupture causing pneumothorax |
| Interstitial emphysema | Air enters connective tissue stroma/mediastinum/subcutaneous tissue; from alveolar tears during coughing |
10. Management Overview
| Category | Approach |
|---|---|
| Smoking cessation | Single most important intervention; slows disease progression |
| Bronchodilators | SABAs (albuterol), LABAs (salmeterol), LAMAs (tiotropium) - relieve dynamic hyperinflation |
| Inhaled corticosteroids | Added in frequent exacerbators |
| Pulmonary rehabilitation | Improves exercise tolerance and quality of life |
| Long-term oxygen therapy | If PaO2 ≤55 mmHg or SaO2 ≤88%; shown to improve survival in hypoxemic COPD |
| A1AT replacement therapy | For A1AT deficiency-related emphysema (weekly IV infusions) |
| Lung volume reduction surgery (LVRS) | Resection of most diseased lung (upper lobe predominant disease); improves mechanics in selected patients |
| Lung transplantation | End-stage disease |
| Endobronchial valves | Minimally invasive LVRS alternative for appropriate candidates |
11. Quick Summary Table
| Feature | Centriacinar | Panacinar |
|---|---|---|
| Location | Respiratory bronchioles | Entire acinus |
| Distribution | Upper lobes | Lower lobes |
| Association | Smoking | A1AT deficiency |
| Relative frequency | ~20x more common | Less common |
| COPD association | Yes | Yes (+ genetic) |
Key References:
- Robbins & Kumar Basic Pathology (10th ed.), pp. 447-451
- Robbins, Cotran & Kumar Pathologic Basis of Disease (10th ed.), pp. 634-639
- Fishman's Pulmonary Diseases and Disorders
Recent evidence note: A 2026 systematic review/meta-analysis (PMID: 41939923) on pulmonary function decline in A1AT deficiency confirms the accelerated emphysema course in this genetic subgroup, consistent with textbook teaching.
This is a shared conversation. Sign in to Orris to start your own chat.