Posterior circulatory stroke with basilarjuction occlusion
Reading File
Finding Sources
Finding Sources
Searching PubMed
"basilar artery occlusion" AND "posterior circulation stroke"
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed for a comprehensive answer. Let me compose the full response.
Posterior Circulation Stroke with Basilar Junction Occlusion
Anatomy and Vascular Territory
The posterior circulation consists of the paired vertebral arteries, the basilar artery, and the paired posterior cerebral arteries (PCAs). The vertebral arteries unite to form the basilar artery at the pontomedullary junction; the basilar then bifurcates into the two PCAs in the interpeduncular fossa. The basilar artery supplies the pons, midbrain, cerebellum, thalami, hippocampi, and medial occipital and temporal lobes via three groups of branches:
| Branch Group | Number | Territory |
|---|---|---|
| Paramedian perforators | 7-10 | Wedge of pons on each side of midline |
| Short circumferential | 5-7 | Lateral two-thirds of pons, middle and superior cerebellar peduncles |
| Long circumferential (SCA, AICA) | Bilateral | Cerebellar hemispheres |
Atheromatous lesions occur most often at the proximal basilar and distal vertebral segments. Emboli from the heart or proximal vertebrobasilar segments are the most common cause of "top of the basilar" syndromes. - Harrison's Principles of Internal Medicine 22E, p. 3477
Clinical Presentation
Because the brainstem packs many structures in close apposition, basilar occlusion produces a diversity of clinical syndromes reflecting combined corticospinal, corticobulbar, ascending sensory tract, and cranial nerve involvement.
Cardinal Features of Complete Basilar Occlusion
- Bilateral long-tract signs (motor + sensory)
- Cranial nerve deficits (multiple levels: V, VI, VII, VIII, III/IV)
- Cerebellar/vestibular signs: vertigo, nausea, vomiting, nystagmus, ataxia
- Altered consciousness (reticular activating system involvement)
- Pontine myoclonus: spontaneous repetitive, multifocal posturing movements that mimic seizure but are NOT epileptic
The hallmark of brainstem stroke is the crossed syndrome - ipsilateral cranial nerve palsy + contralateral long-tract (motor/sensory) signs. - Bradley and Daroff's Neurology in Clinical Practice, p. 353
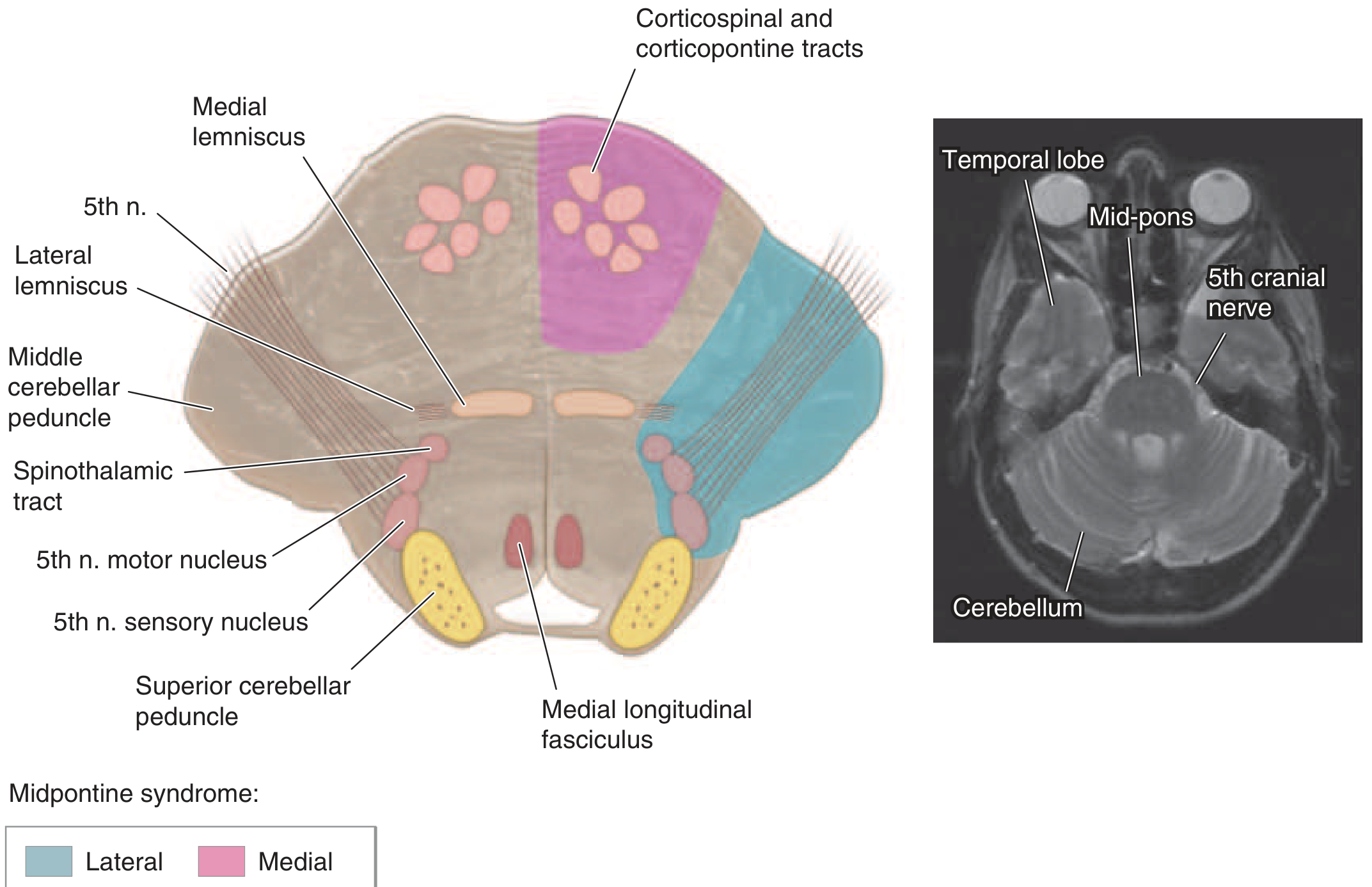
Axial midpons section - medial (pink) and lateral (blue) stroke syndrome territories. Medial: corticospinal/corticopontine tracts, medial lemniscus, MLF. Lateral: spinothalamic tract, CN V nuclei, middle cerebellar peduncle.
Locked-In Syndrome
The most devastating outcome of bilateral basilar/pontine infarction:
- Quadriplegia (corticospinal tract bilateral involvement)
- Anarthria (corticobulbar tract)
- Consciousness preserved (reticular activating system spared)
- Voluntary eye movements and blinking may be the only motor output remaining
- Caused by basis pontis lesion
This is the "locked-in state of preserved consciousness with quadriplegia and cranial nerve signs" that indicates complete pontine and lower midbrain infarction. - Harrison's, p. 3477; Bradley and Daroff's, p. 353
Level-Specific Syndromes at Basilar Junction
Pontine (Mid-basilar occlusion):
- Ipsilateral CN VI/VII palsy + contralateral hemiparesis
- Internuclear ophthalmoplegia (MLF involvement)
- Gaze palsy (ipsilateral pontine gaze center)
- Bilateral involvement → locked-in syndrome
- Pain/temperature loss (spinothalamic)
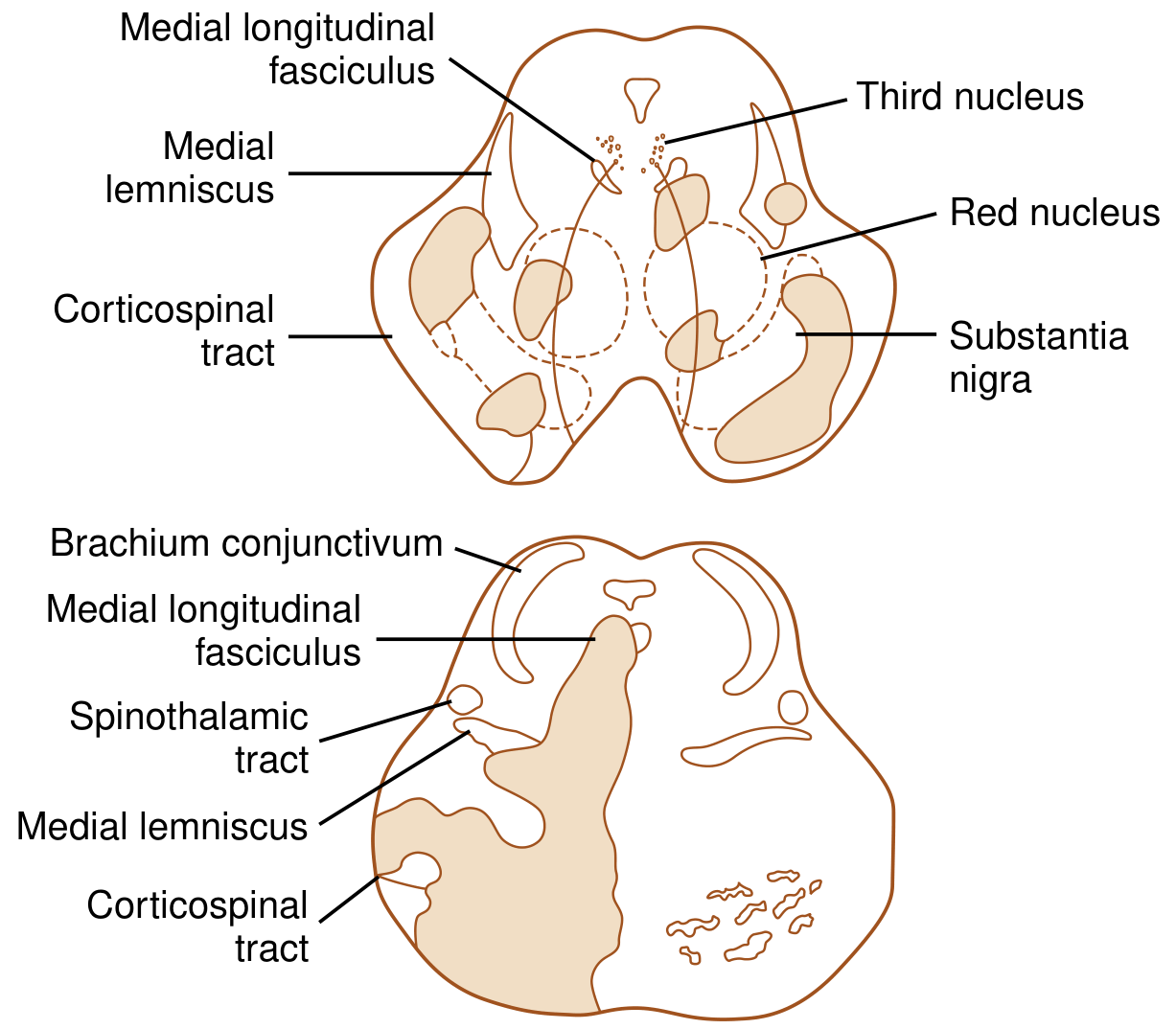
Midbrain (Basilar tip / Top of basilar):
- CN III palsy + contralateral hemiparesis = Weber's syndrome (cerebral peduncle)
- CN III palsy + contralateral ataxia = Claude's syndrome (red nucleus involvement)
- Bilateral CN III palsy, coma, pupils fixed and dilated
- Vertical gaze palsy (rostral interstitial nucleus of MLF)
Thalamic (P1 segment involvement / paramedian perforators):
- Memory disturbance (bilateral thalamic infarction - "thalamic dementia")
- Hypersomnia, altered alertness
- Bilateral involvement of Percheron's artery territory
Superior Cerebellar Artery (SCA) Occlusion
When the SCA (arising near the basilar junction) is occluded:
- Ipsilateral: severe cerebellar ataxia, dysarthria, Horner's syndrome, palatal myoclonus
- Contralateral: loss of pain and temperature (spino- and trigeminothalamic tracts)
- Large SCA infarcts may cause brainstem compression and require neurosurgical decompression
Etiology
- Atherothrombosis - most common at proximal basilar/distal vertebral junction; may be preceded by TIAs or a slowly progressive fluctuating deficit
- Cardioembolism - more typical for "top of the basilar" (distal occlusion)
- Vertebral artery dissection - may extend into the basilar; produces multiple penetrating artery strokes depending on true/false lumen location
- Fibromuscular dysplasia
A series of TIAs and a slowly progressive, fluctuating stroke are extremely significant because they often herald an atherothrombotic occlusion of the distal vertebral or proximal basilar artery. - Harrison's, p. 3477
Diagnosis
- Noncontrast CT: may show basilar hyperdensity sign ("dense basilar sign") - highly specific but poorly sensitive
- CT Angiography (CTA): rapid detection of basilar thrombosis - first-line confirmation; can also assess pc-ASPECTS (posterior circulation ASPECTS score) on CTA source images
- MRI/DWI: best for brainstem infarct detection; CT underestimates posterior fossa ischemia
- CT Perfusion or MR Perfusion: identifies salvageable penumbra to extend time window
- pc-ASPECTS: scoring system on CTA/DWI - each point loss (from 10) corresponds to ischemia in thalamus, cerebellum, or posterior white matter territories
Management
Acute Reperfusion
IV Thrombolysis (IV tPA / Alteplase)
- Standard window: within 4.5 hours of symptom onset (AHA criteria)
- For basilar artery occlusion: IV tPA may be attempted in patients with coma of brief duration and without extensive thrombosis
- The BASICS trial (2022) extended thrombolysis to 24 hours for basilar occlusion - [referenced in Goldman-Cecil Medicine]
- Dose: 0.9 mg/kg (max 90 mg), 10% as bolus, 90% over 60 min
- Tenecteplase (0.25 mg/kg bolus) is now preferred as an alternative given simpler administration for bridging to thrombectomy
Endovascular Mechanical Thrombectomy (EVT)
- For basilar artery occlusion: EVT is the most important intervention
- Several major RCTs (BEST, BASILAR, ATTENTION, BAOCHE) have now demonstrated benefit of EVT over medical therapy alone
- The 2026 meta-analysis by Bouslama et al. (PMID 37005965) confirmed mechanical thrombectomy superiority over medical management for acute basilar artery occlusions
- Time is critical: odds of good outcome >3× if groin puncture within 2 hours; only ~1/3 achieve good outcome if 6 hours elapse
- Collateral status matters: Meta-analysis (Liu et al., 2023) confirmed good collaterals on CTA/MRA are associated with significantly better EVT outcomes
- Extended window up to 24 hours is acceptable with favorable perfusion imaging (DAWN/DEFUSE 3 criteria principles applied to posterior circulation)
Supportive and Secondary Prevention
- Blood pressure: permissive hypertension acutely (do not aggressively lower before reperfusion); target <140/90 after stabilization
- Antiplatelet therapy: aspirin +/- clopidogrel (dual antiplatelet for 21 days for minor stroke/high-risk TIA per CHANCE/POINT trials)
- Anticoagulation: if cardioembolic source (AF), initiate after hemorrhagic transformation window
- Statin: high-intensity statin regardless of baseline LDL
- Temperature management: avoid hyperthermia
- Neurosurgical consult: for large cerebellar infarcts causing brainstem compression or obstructive hydrocephalus
Key Clinical Pearls
- Complete basilar occlusion = neurological emergency with very high mortality if untreated - rapid CTA is mandatory
- The symptom pattern of INO + gaze palsy + bilateral motor signs is pathognomonic for posterior circulation stroke
- Pontine myoclonus (repetitive multifocal movements) in the context of brainstem stroke must NOT be treated as seizures
- Unilateral basilar branch occlusion reduces concern for imminent total occlusion; bilateral signs escalate urgency dramatically
- Vertigo + headache + ataxia (the "posterior circulation triad") should prompt CTA even in young patients - do not dismiss as labyrinthitis without imaging
- Locked-in syndrome is not brain death - these patients are conscious and require communication assessment (eye coding)
Sources: Harrison's Principles of Internal Medicine 22E (2025), p. 3477-3478 | Bradley and Daroff's Neurology in Clinical Practice, pp. 353-355 | Adams and Victor's Principles of Neurology 12E, p. 821 | Neuroanatomy through Clinical Cases 3rd Edition | Recent evidence: Bouslama et al., Interv Neuroradiol 2026, PMID 37005965 | Liu et al., Int J Stroke 2023, PMID 36655949
This is a shared conversation. Sign in to Orris to start your own chat.