carcinoma breast
Reading File
Finding Sources
Searching PubMed
"breast cancer" AND "management"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material from the textbooks. Let me compile a thorough, well-organized answer.
Carcinoma of the Breast
Epidemiology
Breast cancer is the most common malignancy globally in females and the leading cause of cancer death in women worldwide. In 2020, it surpassed lung cancer as the most common cancer overall, accounting for ~12% of all new cancer diagnoses (an estimated 2.3 million new cases). The lifetime risk for an American woman is 1 in 8 (living to age 90).
- 75% of breast cancers are diagnosed after age 50
- Incidence is highest in North America, Northern/Western Europe, and Australia/New Zealand
- Overall risk of death from invasive breast cancer is ~20%, with gradual decline due to improved screening and adjuvant therapy
- Females of African descent have the highest mortality rate, partly due to higher rates of biologically aggressive subtypes (e.g., TNBC)
Risk Factors
(Robbins, Cotran & Kumar Pathologic Basis of Disease)
| Risk Factor | Relative Risk |
|---|---|
| Female sex, increasing age, germline high-penetrance mutations (BRCA1/2), strong family history, personal history of breast cancer, high breast density | >4.0 |
| Germline moderate-penetrance mutations, high-dose chest radiation at <18 years, family history (1 first-degree relative) | 2.1-4.0 |
| Early menarche (<12 yrs), late menopause (>55 yrs), late first pregnancy (>35 yrs), nulliparity, no breastfeeding, exogenous hormone therapy, postmenopausal obesity, physical inactivity, high alcohol intake | 1.1-2.0 |
~20% of breast cancers are attributable to modifiable risk factors (obesity, alcohol, physical inactivity).
Factors that decrease risk: Early first pregnancy (before age 20), prolonged breastfeeding, bilateral prophylactic mastectomy (~90% risk reduction), chemoprevention with ER antagonists (for high-risk women).
Genetic predisposition: ~12% of all breast cancers arise from germline mutations. BRCA1 and BRCA2 account for ~50% of single-gene mutation cases. Other high-risk genes include PALB2 and TP53.
Classification
1. Histological Classification
In Situ Carcinoma:
- Ductal Carcinoma In Situ (DCIS): Precursor to invasive ductal carcinoma. Most often detected on mammography as microcalcifications. If untreated, progression leads to invasive ductal carcinoma in the same breast.
- Lobular Carcinoma In Situ (LCIS): A marker of increased risk and a precursor lesion. When carcinoma subsequently develops, 2/3 are in the same breast and 1/3 in the contralateral breast.
Invasive Carcinoma:
The classic Foote-Stewart classification (Schwartz's Principles of Surgery):
| Type | Frequency |
|---|---|
| Invasive ductal carcinoma, no special type (NST) | ~80% |
| Invasive lobular carcinoma | ~10% |
| Medullary carcinoma | ~4% |
| Mucinous (colloid) carcinoma | ~2% |
| Papillary carcinoma | ~2% |
| Tubular carcinoma | ~2% |
| Paget's disease of the nipple | Rare |
| Rare: adenoid cystic, squamous cell, apocrine | Rare |
Invasive carcinoma of no special type (NST) - the most common subtype - typically presents as a hard, irregular, radiodense mass with a desmoplastic stromal reaction. When cut, it produces a characteristic grating sound.
Paget's disease of the nipple presents as chronic eczematous eruption of the nipple progressing to ulceration. Pathognomonic: large pale vacuolated Paget cells in the rete pegs. Differentiated from melanoma by carcinoembryonic antigen staining (vs. S-100 in melanoma).
2. Clinical Subtypes (Biomarker-Based) & Molecular Subtypes
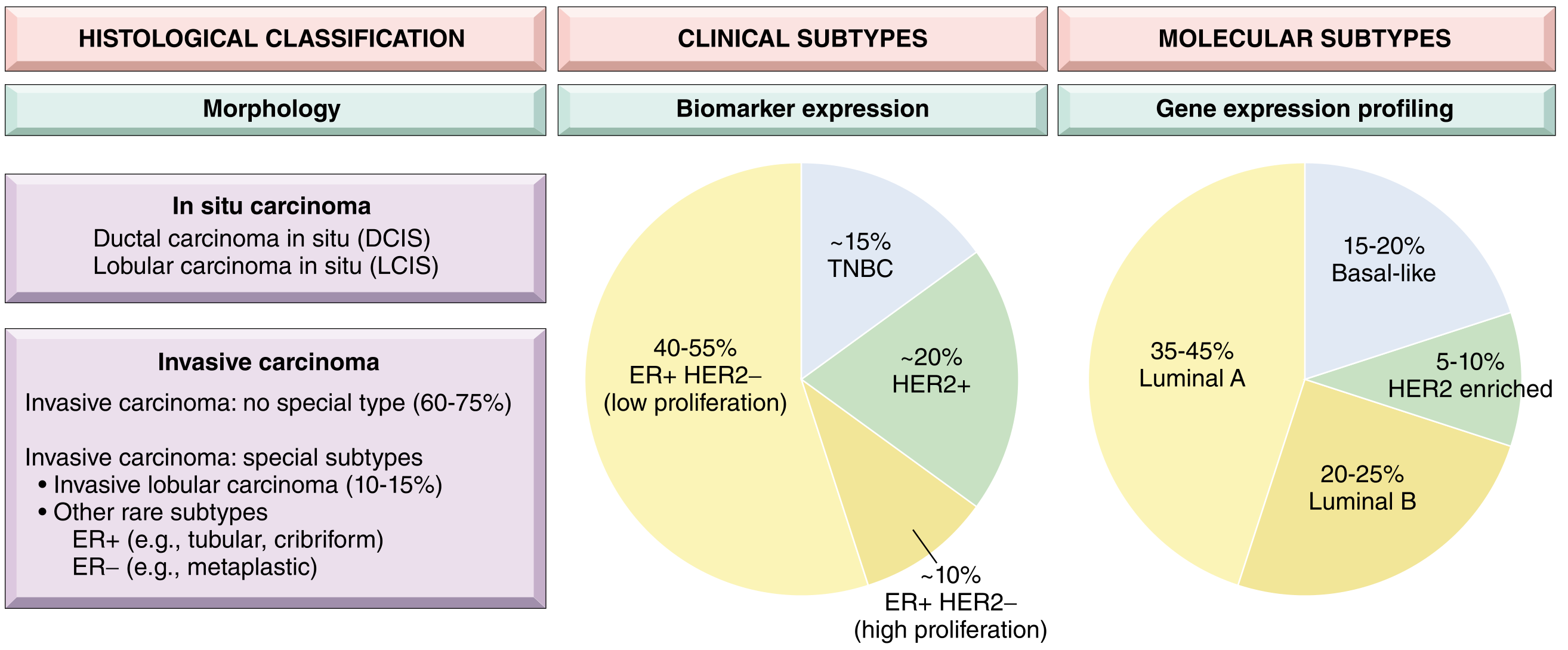
(Fig. 23.15 - Robbins, Cotran & Kumar Pathologic Basis of Disease)
| Clinical Subtype | Biomarker Profile | Molecular Subtype | Frequency |
|---|---|---|---|
| Luminal | ER+/HER2- (low proliferation) | Luminal A | 35-45% |
| Luminal | ER+/HER2- (high proliferation) | Luminal B | 20-25% |
| HER2 | HER2+ (ER+/- ) | HER2-enriched | ~20% |
| Triple Negative (TNBC) | ER-/PR-/HER2- | Basal-like | ~15% |
Key molecular subtype features:
- Luminal A: Low grade, ER-positive, best prognosis, responds to endocrine therapy
- Luminal B: Higher proliferation, worse prognosis than A
- HER2-enriched: HER2 gene amplification/overexpression; responds to HER2-targeted therapy (trastuzumab, pertuzumab); high proliferation, often ER-negative
- TNBC/Basal-like: Associated with BRCA1 mutations and TP53 mutations; high-grade, most aggressive, poorest prognosis; only systemic option was chemotherapy (immunotherapy now plays a role)
Pathogenesis
Two major pathways (Robbins, Cotran & Kumar):
Low-grade pathway (ER-positive): Columnar cell lesions → flat epithelial atypia → atypical ductal/lobular hyperplasia → low-grade DCIS / classic LCIS → low-grade invasive carcinoma. Genetically defined by loss of 16q.
High-grade pathway (ER-negative/TNBC): Often driven by BRCA1 loss-of-function and TP53 mutations. High-grade DCIS → high-grade invasive carcinoma.
Histological Grading (Nottingham Score)
All invasive carcinomas are graded by:
- Tubule/gland formation
- Nuclear pleomorphism
- Mitotic rate
- Grade 1 (well differentiated): Tubular/cribriform pattern, small uniform nuclei, low mitotic rate
- Grade 2 (moderately differentiated): Solid clusters or single cells, greater nuclear pleomorphism, more mitoses
- Grade 3 (poorly differentiated): Ragged nests/sheets, enlarged irregular nuclei, high mitotic rate, frequent necrosis
Clinical Features
- Painless breast lump (most common presentation)
- Skin dimpling or retraction (due to involvement of Cooper's ligaments)
- Nipple retraction or discharge
- Peau d'orange appearance (lymphedema of skin)
- Axillary lymphadenopathy
- In inflammatory breast carcinoma: warm, erythematous, edematous breast with rapid onset - a clinical diagnosis
Diagnosis
Triple assessment:
- Clinical: History and physical examination
- Imaging: Mammography (principal screening tool), ultrasound (especially useful in young/dense breasts and axillary staging), MRI for high-risk screening
- Pathology: Fine needle aspiration (FNA), core needle biopsy (preferred - provides histology + receptor status)
Mammographic signs of malignancy:
- Spiculated/irregular mass
- Asymmetric density/architectural distortion
- Clustered microcalcifications (especially in DCIS)
Biomarker testing on all invasive cancers:
- ER and PR (immunohistochemistry)
- HER2 (IHC + FISH for gene amplification)
- Ki-67 (proliferation index)
- Gene expression assays (Oncotype DX, MammaPrint) to guide adjuvant chemotherapy decisions in certain ER+/HER2- cases
Staging (AJCC 8th Edition TNM)
The 8th edition uniquely incorporates both anatomic stage and biologic factors (ER, PR, HER2, grade, Oncotype DX score) to create prognostic stage groups.
T - Primary Tumor:
- TX: Cannot assess
- T0: No evidence
- Tis: In situ (DCIS or Paget's without invasive tumor)
- T1: ≤2 cm (T1mi ≤0.1 cm, T1a >0.1-0.5 cm, T1b >0.5-1 cm, T1c >1-2 cm)
- T2: >2-5 cm
- T3: >5 cm
- T4: Any size with chest wall or skin involvement (T4d = inflammatory carcinoma)
N - Regional Lymph Nodes:
- N0: No regional node metastasis
- N1: Movable ipsilateral axillary nodes (level I/II)
- N2: Fixed ipsilateral axillary nodes OR internal mammary nodes without axillary
- N3: Ipsilateral infraclavicular (level III) / supraclavicular / internal mammary + axillary
M - Distant Metastasis:
- M0: No distant metastasis
- M1: Distant metastasis (bone, liver, lung, brain commonest)
Overall Stage Groups: Stage 0 to IV. Number of positive axillary lymph nodes is one of the most important predictors of 10- and 20-year survival.
Surgical Management
Breast Surgery Options
- Breast-conserving surgery (BCS/lumpectomy): Wide local excision + radiation therapy; equivalent survival to mastectomy for appropriate candidates (tumor <4-5 cm, favorable tumor-to-breast ratio, no multicentric disease, no contraindication to radiotherapy)
- Mastectomy: Simple/total, modified radical (with axillary dissection), skin/nipple-sparing for reconstruction candidates
- Oncoplastic techniques: Combine resection and immediate reconstruction
Axillary Staging
- Sentinel lymph node biopsy (SLNB): Standard for clinically node-negative patients; avoids full axillary clearance and its morbidity (lymphedema)
- Axillary lymph node dissection (ALND): For positive sentinel nodes (per institutional/clinical trial criteria), clinically node-positive, or when SLNB not feasible
Systemic Treatment
Adjuvant Chemotherapy
- Used in: HER2+, TNBC, high-grade luminal B, high-risk luminal cancers
- Common regimens: AC (doxorubicin + cyclophosphamide) → Taxane (paclitaxel/docetaxel)
- Gene expression assays (Oncotype DX Recurrence Score) guide chemotherapy decisions in ER+/HER2-/node-negative patients
Endocrine Therapy
- For ER+ and/or PR+ tumors (all subtypes)
- Premenopausal: Tamoxifen (SERM) ± ovarian suppression for 5-10 years; aromatase inhibitors (AIs) + ovarian suppression for high-risk
- Postmenopausal: Aromatase inhibitors (anastrozole, letrozole, exemestane) preferred over tamoxifen; extended therapy (up to 10 years) for high-risk disease
- CDK4/6 inhibitors (palbociclib, ribociclib, abemaciclib) + AI for metastatic ER+/HER2- disease, and abemaciclib now approved adjuvantly in high-risk early breast cancer
Anti-HER2 Therapy
- Trastuzumab (Herceptin): Monoclonal antibody against HER2; adjuvant + neoadjuvant; combined with chemotherapy
- Pertuzumab: Combined with trastuzumab + docetaxel (neoadjuvant/metastatic)
- T-DM1 (ado-trastuzumab emtansine): Antibody-drug conjugate for residual disease after neoadjuvant therapy
- Lapatinib, neratinib, tucatinib: Oral HER2-targeted tyrosine kinase inhibitors
TNBC Treatment
- Chemotherapy remains backbone
- Immunotherapy: Pembrolizumab (anti-PD-1) + chemotherapy for PD-L1 positive metastatic TNBC and for early high-risk TNBC (neoadjuvant)
- PARP inhibitors (olaparib, talazoparib): For BRCA1/2 mutant HER2-negative metastatic breast cancer
- Antibody-drug conjugates: Sacituzumab govitecan (anti-Trop-2) for metastatic TNBC
Radiation Therapy
- After BCS: Whole-breast irradiation ± boost to tumor bed (standard)
- Post-mastectomy radiation (PMRT): For ≥4 positive nodes, T3/T4 tumors, positive margins
- Regional nodal irradiation for node-positive disease
Neoadjuvant Therapy
- Allows tumor downstaging for BCS eligibility
- Pathologic complete response (pCR) is a surrogate for improved outcomes
- HER2+ and TNBC show highest pCR rates
- Enables tailoring of adjuvant therapy based on residual disease
Prognosis
Prognosis depends on:
- Biologic subtype - Luminal A best; TNBC worst
- Anatomic stage - Tumor size and nodal status
- Grade
- Response to treatment
Luminal cancers show a prolonged risk of late recurrence (beyond 5 years), while TNBCs recur early. HER2 cancers, once the worst prognosis group, have been transformed by targeted therapy.
The AJCC 8th edition prognostic stage groups combine anatomic and biologic factors, providing more accurate survival estimates than anatomy alone.
Sources:
- Robbins & Kumar Basic Pathology, Ch. on Breast Carcinoma
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Ch. 23 (Breast)
- Schwartz's Principles of Surgery, 11th Ed., Ch. 17 (Breast)
- Bailey and Love's Short Practice of Surgery, 28th Ed., Ch. on Breast
tubercular peritonitis
Reading File
Finding Sources
Searching PubMed
"tuberculous peritonitis" AND diagnosis
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive, well-sourced content from five textbooks. Let me compile the full answer.
Tubercular (Tuberculous) Peritonitis
Definition and Overview
Tuberculous peritonitis (TBP) is a form of extrapulmonary tuberculosis involving the peritoneal cavity, caused by Mycobacterium tuberculosis. It is the sixth most common site of extrapulmonary TB, accounting for 0.5% of new TB cases. The abdomen is involved in approximately 11% of patients with extrapulmonary TB overall. The condition is common in resource-poor countries but its incidence is rising in resource-rich nations due to migration, HIV co-infection, and immunosuppression.
Pathogenesis / Routes of Spread
TB reaches the peritoneum by four main routes (Bailey and Love, 28th Ed.):
- Gastrointestinal tract - through the ileocaecal region (the most common GI site of abdominal TB) via mesenteric lymph nodes
- Haematogenous spread - from miliary TB (most common) or cavitating pulmonary TB
- Lymphatic spread - from involved retroperitoneal or mesenteric nodes
- Direct spread - from the Fallopian tubes (in women)
50-80% of patients with abdominal TB have peritoneal involvement.
Important: Active pulmonary TB is uncommon in patients with TBP - only about one-third have clinical or radiographic evidence of pulmonary disease. (Frameworks for Internal Medicine)
Pathological Types (Morphological Classification)
(Bailey and Love)
| Type | Features | Frequency |
|---|---|---|
| Wet (Ascitic) type | Generalised or loculated ascites; multiple tubercle deposits on both peritoneal layers | ~90% (most common) |
| Dry (Plastic/Fibrotic) type | Fibrotic fixed loops of bowel and omentum matted together; no ascites; may cause subacute intestinal obstruction | Less common |
| Mixed type | Features of both wet and dry forms | Less common |
The dry type typically presents with intestinal obstruction rather than ascites, and can be clinically indistinguishable from carcinomatosis or Crohn's disease.
Risk Factors
- HIV co-infection (most significant immunosuppressive risk)
- Liver cirrhosis (ascites masks TB symptoms; also reduces host immune response)
- Diabetes mellitus
- Underlying malignancy
- Chronic renal failure / peritoneal dialysis
- Immunosuppressive therapy
- Residence in or migration from endemic countries
Clinical Features
Presentation is typically insidious, with symptoms present for weeks to months before diagnosis. (Yamada's Textbook of Gastroenterology)
Systemic symptoms (constitutional):
- Low-grade fever and night sweats
- Weight loss and anorexia
- Malaise and fatigue
Abdominal symptoms:
- Abdominal pain (most common presenting symptom) - often diffuse and dull
- Abdominal distension / swelling (due to ascites)
- Abdominal tenderness - present in less than half of patients
Other features:
- Doughy feel of the abdomen (due to omental thickening and matted bowel loops)
- Features of intestinal obstruction (in fibrotic/dry type)
- Acute presentation resembling bacterial peritonitis (rare but occurs)
Note: The co-existence of TBP with cirrhosis is particularly deceptive - TB symptoms may be completely masked by the underlying liver disease. A high index of suspicion is needed in any patient with ascites + fever + abdominal tenderness. (Murray & Nadel's)
Diagnosis
1. Ascitic Fluid Analysis (Paracentesis)
This is the first-line investigation. Key characteristics:
| Parameter | Finding in TBP |
|---|---|
| Appearance | Straw-coloured exudate |
| Protein | >25-30 g/L (>3 g/dL) - exudative |
| WBC count | >500 cells/mL (typically 50-10,000 leukocytes/µL) |
| Cell differential | Lymphocytic predominance (>40-70%) |
| SAAG | Low (<1.1 g/dL) in non-cirrhotic patients |
| Glucose | Low |
| AFB smear | Positive in <3% of cases |
| AFB culture | Positive in ~40-50%; takes 4-8 weeks |
SAAG caveat: In cirrhotic patients with TBP, the SAAG may be high (>1.1 g/dL) due to concurrent portal hypertension, making the diagnosis even harder. (Yamada's)
Lymphocytic ascites differential: Cancer causes lymphocytic ascites ~10 times more often than TB. Key distinguishing feature: if peritoneal carcinomatosis is present, cytology is positive in >90% of cases. If cytology is negative and fever is present, TB is the likely diagnosis. (Sleisenger & Fordtran's; Yamada's)
2. Adenosine Deaminase (ADA) in Ascitic Fluid
This is the most useful rapid, non-invasive diagnostic test.
- ADA sensitivity: 100%, specificity: 97% (meta-analysis of 12 studies, n=264 patients)
- Optimal cut-off: 39 IU/L (range 36-40 IU/L used across studies)
- High sensitivity and specificity for differentiating TBP from peritoneal carcinomatosis
- Limitations:
- False negatives in HIV co-infection and cirrhosis
- False positives in malignant ascites
- Recommended in all cases of suspected TBP given diagnostic accuracy and wide availability (Yamada's)
(Murray & Nadel's confirms: ADA sensitivity 93%, specificity 96% for TBP)
3. Molecular Tests
- Xpert MTB/RIF (GeneXpert PCR): Rapid molecular test; highly sensitive and specific for M. tuberculosis in ascitic fluid; provides results in hours and detects rifampicin resistance
- PCR for MTB: Highly sensitive and specific; results in days vs. weeks for culture (Frameworks for Internal Medicine)
- ELISPOT: Novel, rapid, immunological test - detects interferon-gamma release (Sleisenger & Fordtran's)
- Serum QuantiFERON-TB Gold: Poor test characteristics for diagnosing active TBP, especially in TB-endemic countries with BCG vaccination (Sleisenger & Fordtran's)
4. Imaging
-
Ultrasonography / CT abdomen:
- Detection of free or loculated ascites
- Lymphadenopathy (mesenteric/retroperitoneal)
- Diffuse thickening of peritoneum, mesentery, and omentum
- "Omental caking" can mimic malignancy
- TBP may appear as a pelvic mass with elevated CA-125, closely mimicking metastatic ovarian cancer (Sleisenger & Fordtran's)
-
Chest X-ray / CT chest: To detect concurrent pulmonary TB (present in ~30%)
5. Laparoscopy + Peritoneal Biopsy
The gold-standard investigation. (Yamada's)
- Near 100% sensitivity for detecting TBP
- Characteristic macroscopic appearances: scattered whitish/miliary peritoneal nodules (tubercles), thickened peritoneum
- All nodules should be biopsied
- Histology: Caseating granulomas in >90% of cases
- Allows simultaneous culture of biopsy tissue
- Should be performed at an early stage whenever TBP is suspected and non-invasive tests are inconclusive
Summary of diagnostic algorithm:
- Paracentesis → ascitic fluid analysis (protein, SAAG, cell count, cytology, ADA, AFB smear + culture)
- If cytology positive → peritoneal carcinomatosis diagnosis made
- If cytology negative + fever + lymphocytic ascites → proceed to ADA / Xpert MTB/RIF
- If still inconclusive → laparoscopy + peritoneal biopsy
Differential Diagnosis
- Peritoneal carcinomatosis (most important - especially ovarian, GI malignancy)
- Spontaneous bacterial peritonitis (in cirrhosis)
- Cirrhotic ascites
- Fat necrosis of pancreatitis (caseating nodules can mimic)
- Mesothelioma
- Familial Mediterranean fever
- Other granulomatous peritonitis (fungal, sarcoidosis, Crohn's disease)
Treatment
Anti-TB Drug Regimen
(Consistent across Sleisenger & Fordtran's, Yamada's, and Bailey and Love)
Standard 6-month regimen:
| Phase | Duration | Drugs |
|---|---|---|
| Intensive phase | 8 weeks (2 months) | Isoniazid (H) + Rifampicin (R) + Pyrazinamide (Z) + Ethambutol (E) → 2HRZE |
| Continuation phase | 16 weeks (4 months) | Isoniazid (H) + Rifampicin (R) → 4HR |
- Total duration: 6 months for uncomplicated TBP
- May be extended to 9-12 months depending on local drug susceptibility patterns and emergence of resistant strains
- Multi-drug resistant TB (MDR-TB) may be more common in abdominal than pulmonary TB - drug susceptibility testing is essential
- All treatment must be directly observed (DOT) by public health/clinical staff - erratic treatment leads to resistance
Special situations:
- Cirrhotic patients: Hepatotoxicity of first-line drugs (isoniazid, rifampicin, pyrazinamide) may necessitate modification of regimen - requires careful monitoring of LFTs
- HIV co-infection: Manage with specialist involvement; rifampicin interactions with antiretrovirals require attention
Supportive Management
- Nutritional support and hydration
- Corticosteroids: Controversial; may be considered in severely symptomatic or complications cases to reduce inflammation - evidence limited
Surgical Management
Surgery is not primary but may be required for complications:
- Intestinal obstruction (may respond to anti-TB treatment without surgery first)
- Bowel perforation
- Fistula formation
- Abscesses not responding to medical therapy
Prognosis
- Generally good with prompt diagnosis and appropriate treatment
- Delayed diagnosis significantly increases morbidity and mortality
- Late diagnosis is common due to the insidious nature and frequent absence of pulmonary TB
- Complications (intestinal obstruction, adhesions) may persist even after successful treatment of infection
Sources:
- Bailey and Love's Short Practice of Surgery, 28th Ed. - Ch. 65 (Peritoneum)
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease - Tuberculous Peritonitis
- Yamada's Textbook of Gastroenterology, 7th Ed. - Evaluation of Peritoneal Tuberculosis
- Murray & Nadel's Textbook of Respiratory Medicine - Peritoneal Tuberculosis
- Frameworks for Internal Medicine - Peritoneal Tuberculosis Diagnostics
This is a shared conversation. Sign in to Orris to start your own chat.