ABG
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Now I have all the content needed for a thorough answer. Let me compile it.
ABG: Acid-Base Disorders
Normal ABG Values
| Parameter | Normal Range |
|---|---|
| pH | 7.35 - 7.45 |
| PaCO2 | 35 - 45 mmHg |
| HCO3- | 22 - 26 mEq/L |
| PaO2 | 80 - 100 mmHg |
| Base excess | -2 to +2 mEq/L |
- pH < 7.35 = Acidemia
- pH > 7.45 = Alkalemia
The HCO3- on an ABG is a calculated value (via Henderson-Hasselbalch); the measured serum bicarb from a simultaneous chemistry panel should match within 2-3 mEq/L. A discrepancy suggests a lab error or non-simultaneous draws.
The Henderson-Hasselbalch Framework
Blood pH is determined by the ratio of HCO3- to CO2:
pH = 6.1 + log([HCO3-] / 0.03 × PaCO2)
This means pH is disturbed by changes in either HCO3- (metabolic) or PaCO2 (respiratory).
The Four Primary Disorders
| Disorder | Primary Change | pH | Compensatory Response |
|---|---|---|---|
| Metabolic Acidosis | HCO3- falls | Falls | Hyperventilation (PCO2 falls) |
| Metabolic Alkalosis | HCO3- rises | Rises | Hypoventilation (PCO2 rises) |
| Respiratory Acidosis | PCO2 rises | Falls | Renal HCO3- retention |
| Respiratory Alkalosis | PCO2 falls | Rises | Renal HCO3- excretion |
Key rule: The compensatory response always goes in the same direction as the original disturbance. Compensation normalizes pH but does not overcorrect it.
- Respiratory disorders: compensated renally (hours to days)
- Metabolic disorders: compensated respiratorily (minutes to hours)
Step-by-Step ABG Interpretation
Step 1 - pH: Is the patient acidemic (< 7.35) or alkalemic (> 7.45)?
Step 2 - Identify the primary process:
- pH ↓ + PaCO2 ↑ = Respiratory acidosis
- pH ↓ + PaCO2 ↓ = Metabolic acidosis
- pH ↑ + PaCO2 ↓ = Respiratory alkalosis
- pH ↑ + PaCO2 ↑ = Metabolic alkalosis
Step 3 - Assess compensation (is it appropriate?):
- Metabolic acidosis: expected PaCO2 = (1.5 × HCO3 + 8) ± 2 (Winter's formula)
- Metabolic alkalosis: expected PaCO2 = 40 + 0.7 × (HCO3 - 24)
- Acute respiratory acidosis: HCO3 rises ~1 mEq/L per 10 mmHg rise in PaCO2
- Chronic respiratory acidosis: HCO3 rises ~3.5 mEq/L per 10 mmHg rise in PaCO2
If compensation is not appropriate, a mixed disorder is likely.
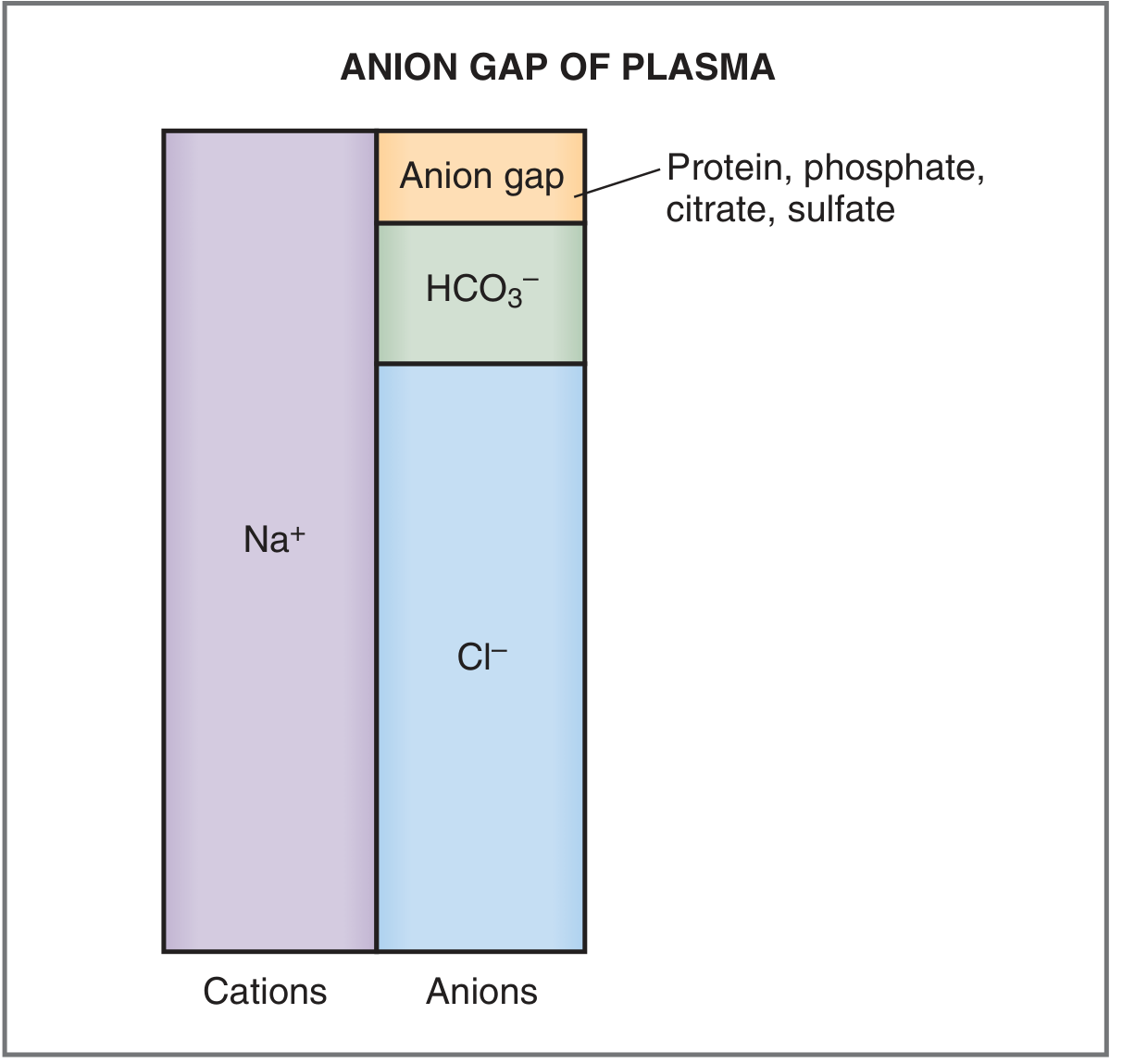
Step 4 - Anion gap (for any metabolic acidosis or suspected mixed disorder):
AG = Na+ - (HCO3- + Cl-) Normal = 8-12 mEq/L
Correct for albumin: Add 2.5 × (4 - observed albumin) to the measured AG. Always calculate the AG even when pH and PaCO2 appear near-normal, as a high AG may unmask a mixed disorder.
Step 5 - If AG is elevated, calculate the Delta-Delta ratio (Δ/Δ):
Δ/Δ = (AG - 12) / (24 - HCO3)
| Δ/Δ | Interpretation |
|---|---|
| < 1.0 | Concurrent non-AG metabolic acidosis |
| 1.0 - 2.0 | Pure AG metabolic acidosis |
| > 2.0 | Concurrent metabolic alkalosis (or chronic resp. acidosis) |
The Four Disorders in Detail
1. Metabolic Acidosis (HCO3- < 22)
High AG causes - MUDPILES:
- M - Methanol
- U - Uremia (renal failure)
- D - DKA / ketoacidosis
- P - Propylene glycol / Paraldehyde
- I - Isoniazid, Iron
- L - Lactic acidosis (most common perioperatively)
- E - Ethylene glycol
- S - Salicylates, Short gut
If osmol gap is elevated (measured osmolality - calculated osmolality > 10), consider methanol or ethylene glycol poisoning.
Normal AG (hyperchloremic) causes:
- Diarrhea / GI bicarbonate loss
- Renal tubular acidosis (RTA)
- Excessive normal saline administration (dilutional hyperchloremic acidosis)
- GI fistulas, nasogastric suctioning
Treatment: Correct the underlying cause. Bicarbonate administration is reserved for severe acidosis (pH < 7.15) as a bridge only - it does not address the root cause.
2. Metabolic Alkalosis (HCO3- > 26)
Causes:
- Vomiting / nasogastric suctioning (loss of H+ as HCl)
- Diuretics
- Hypovolemia (contraction alkalosis - renal Na+/H+ exchange retains HCO3-)
- Hypokalemia
- Classic example: Hypochloremic, hypokalemic metabolic alkalosis in pyloric stenosis
Treatment: Address the underlying cause; chloride repletion (normal saline) for chloride-responsive alkalosis; potassium supplementation; stop offending diuretics.
3. Respiratory Acidosis (PaCO2 > 45)
Causes:
- Hypoventilation: CNS depression (sedatives, opioids, stroke, trauma)
- Airway obstruction
- Neuromuscular failure (paralysis, hypophosphatemia)
- Chronic: COPD, obesity hypoventilation, neuromuscular disorders
Treatment: Increase minute ventilation (raise tidal volume or respiratory rate on ventilator); treat the underlying cause. Non-invasive ventilation (BiPAP) for COPD exacerbations. Caution: do not overcorrect a patient with chronic hypercapnia to a "normal" PaCO2 - this causes a sudden metabolic alkalosis.
4. Respiratory Alkalosis (PaCO2 < 35)
Causes:
- Hyperventilation (anxiety, pain, fever)
- Hypoxemia (stimulates respiratory drive)
- Pulmonary embolism
- Salicylate toxicity (early stage)
- Iatrogenic (ventilator settings)
- Hepatic encephalopathy
- Classic use: intentional hyperventilation to induce cerebral vasoconstriction in acute TBI (short-term only)
Treatment: Correct the underlying trigger.
Buffering Systems
The body has three layers of defense against pH changes:
- Chemical buffers (immediate, minutes): Bicarbonate-CO2 system (ECF), phosphate, proteins, and hemoglobin (ICF)
- Respiratory compensation (minutes to hours): Adjusts PaCO2
- Renal compensation (hours to days): Adjusts HCO3- reabsorption/excretion and H+ secretion
Sources: Costanzo Physiology 7th Ed., p. 330-331; Current Surgical Therapy 14e, p. 1607; Barash Clinical Anesthesia 9e, p. 1158-1159
This is a shared conversation. Sign in to Orris to start your own chat.