Paragonimus lung diseases for md exam answer 10 marks from fishman and Murray only
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from both Fishman's and Murray & Nadel's. I have everything needed for a thorough 10-mark MD exam answer. Let me compose it.
Paragonimiasis (Lung Fluke Disease) - 10 Mark Answer
Sources: Fishman's Pulmonary Diseases and Disorders, 5e & Murray & Nadel's Textbook of Respiratory Medicine, 7e
Definition and Etiology
Paragonimiasis is a parasitic lung infection caused by trematodes (flukes) of the genus Paragonimus. The principal pathogen in humans is P. westermani (the Oriental lung fluke), responsible for >90% of cases worldwide, predominantly in Asia. In North America, P. kellicotti is the only indigenous species and causes most locally acquired infections through crayfish ingestion. Other species - P. africanus, P. uterobilateralis, P. heterotremus - cause disease in Africa and Southeast Asia. An estimated 25 million people are infected globally, with 300 million at risk.
(Fishman's, p. 1219; Murray & Nadel's, p. 1347)
Life Cycle and Pathogenesis
The life cycle is complex, requiring two intermediate hosts:
- Definitive host: Humans, cats, dogs, wild boar, and other mammals
- First intermediate host: Freshwater snails (cercariae develop here)
- Second intermediate host: Crustaceans - crabs or crayfish (metacercariae encyst here)
Infection route: Humans are infected by eating raw, partially cooked, or pickled crustaceans containing encysted metacercariae. The metacercariae excyst in the duodenum, penetrate the duodenal/intestinal wall, cross the peritoneal cavity, migrate through the diaphragm, and enter the pleural space and lung parenchyma, where they mature to adult worms.
Adult worm behavior: Pairs of adult worms live in cystic cavities near bronchial passages and produce large, thick-shelled operculated eggs (~80 x 50 μm). Cystic cavities eventually rupture into bronchioles, allowing eggs to be expectorated or swallowed and passed in feces. Unembryonated eggs released into freshwater infect snails, completing the cycle.
Extrapulmonary migration: Paragonimus has a unique tropism for the lung, but aberrant migration can occur to the brain (most common extrapulmonary site), skin, and peritoneum.
(Murray & Nadel's, p. 1347-1348; Fishman's, p. 1219)
Clinical Features
The clinical syndrome reflects the parasite's migratory path and host immune interaction. Symptoms typically begin 2-16 weeks after ingesting infective larvae.
Acute Phase
- Fever, abdominal pain, diarrhea, urticaria
- Chest pain, cough
- Peripheral eosinophilia and elevated serum IgE (present in 80% of infected patients)
- Many acute infections are asymptomatic
Chronic/Late Phase (5-10 years after exposure)
- Chronic cough productive of thick, rusty-colored or blood-tinged sputum containing Charcot-Leyden crystals
- Hemoptysis - may be frank and resemble that seen in tuberculosis (this is the classic TB mimic)
- Fever and eosinophilia are often absent at this stage
- Pleuritic chest pain
- Pneumonia, bronchiectasis, and vasculitis may be present
Pleural Disease
Pleural involvement is common - in a series of 71 patients, 61% had pleural disease:
- Unilateral pleural effusion (most common)
- Bilateral effusion
- Unilateral or bilateral hydropneumothorax
- Pleural thickening
Characteristic pleural fluid in paragonimiasis (unique and diagnostically important):
- Exudative
- Glucose < 10 mg/dL (very low - < 0.56 mmol/L)
- LDH > 3 times upper limit of normal for serum
- pH < 7.10
- High percentage of eosinophils on cell differential
- May contain cholesterol crystals or chyle
This combination of low pH + low glucose + eosinophilia is found in only TWO conditions: (1) Paragonimiasis, and (2) Eosinophilic granulomatosis with polyangiitis (EGPA). This is a classic exam fact.
(Murray & Nadel's, p. 1348-1349; block 25)
Diagnostic Investigations
Laboratory
- Blood eosinophilia and raised IgE - present in ~80%
- Definitive diagnosis: Detection of Paragonimus eggs in sputum, stool, BAL fluid, gastric aspirate, or pleural fluid - however, eggs are detected in only 11.7% of cases (Japan series)
- Bloody sputum is most likely to yield positive results
- Eggs are operculated, golden-brown, ~80 x 50 μm (see Fig. 58.4D in Murray & Nadel's)
- ELISA and immunoblot assays: Most sensitive; used when egg detection fails
- Complement fixation titer > 1:8 for P. westermani is strongly suggestive
Pathology
- Lung biopsy: Fibrous cysts (1-3 mm) adjacent to or communicating with airways, containing adult worms
- Granulomas with eggs at the center (see Fig. 58.4B)
- Acute and chronic changes may coexist within the same lesion
Radiology
Chest X-Ray may show:
- Minimal perihilar linear/reticular opacities (early)
- Consolidation or focal parenchymal infiltrates
- Cavitary lesions up to 4 cm in diameter
- Small cysts; calcified or non-calcified nodules
- Pleural effusion, pneumothorax, pleural thickening (minority)
CT Scan (more sensitive, Fishman's):
- Pleural effusion - most common CT finding
- Early: parenchymal consolidations (during lung penetration)
- Late: peripheral nodules or worm-containing cysts
- Serpentine worm migration tracks
- Pneumothorax, lymphadenopathy
(Fishman's, p. 1219; Murray & Nadel's, p. 1347-1349)
Pathology Image (Murray & Nadel's, Figure 58.4)
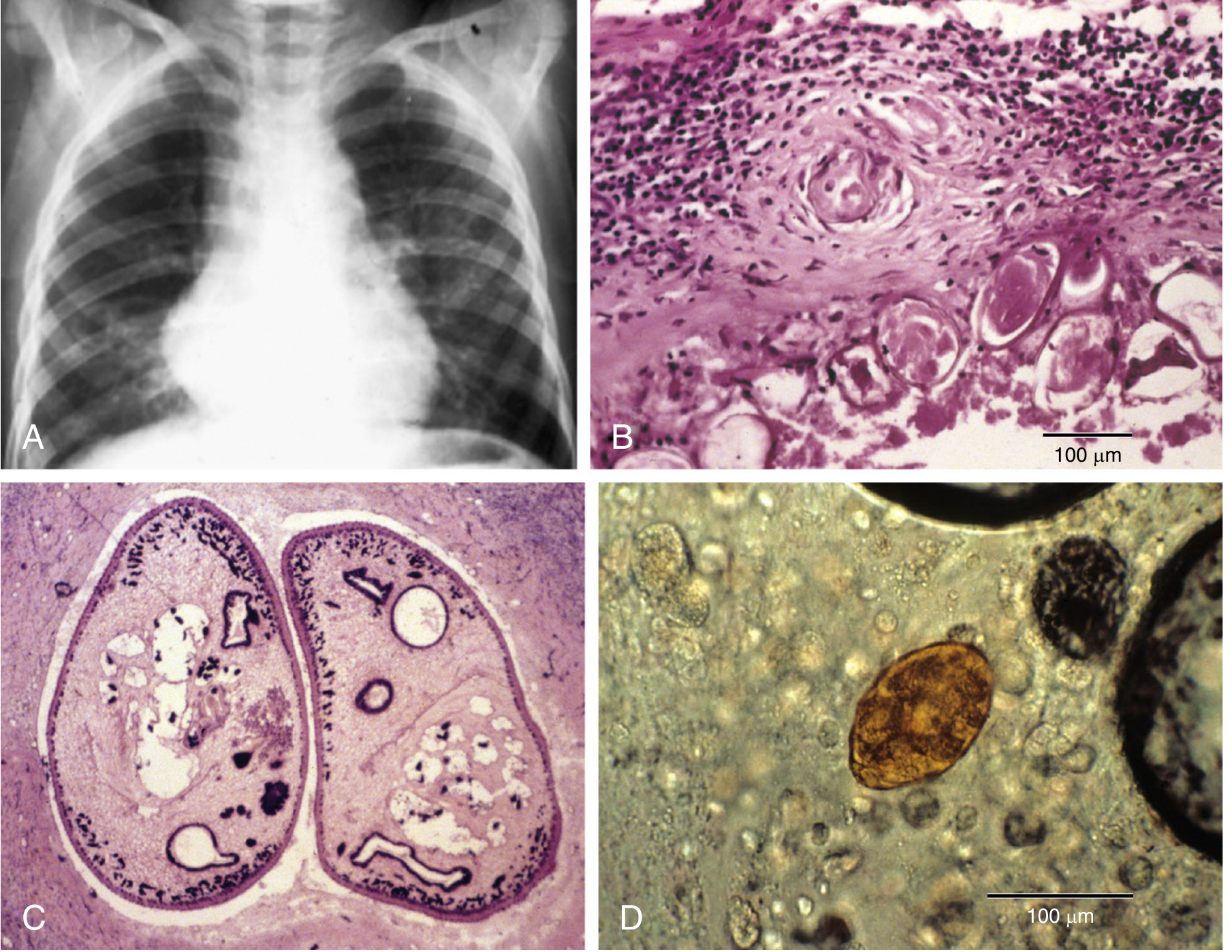
Figure 58.4 (Murray & Nadel's): (A) CXR showing perihilar linear and reticular opacities in a patient with hemoptysis; (B) Granuloma surrounding ova; (C) Cross-section of a pair of adult worms in the lung; (D) Operculated ovum in sputum.
Differential Diagnosis
The chief differential is pulmonary tuberculosis - paragonimiasis can be mistaken for TB due to:
- Similar geographic distribution (Asia)
- Chronic cough, hemoptysis, cavitary lesions on CXR
- Night sweats and constitutional symptoms
Other differentials: lung abscess, bronchiectasis, lung cancer (when nodules/cavities are present).
Treatment
- Drug of choice: Praziquantel - 75 mg/kg/day in 3 divided doses for 2 days
- Treatment failure is rare
- Untreated pulmonary paragonimiasis may resolve within 5-10 years (the lifespan of adult worms), but chronic infection may lead to extensive pulmonary fibrosis
(Fishman's, p. 1219; Murray & Nadel's, p. 1349)
Prevention
- Avoid eating raw, undercooked, or pickled crustaceans (crabs, crayfish)
- Adequate cooking destroys metacercariae
Summary Table
| Feature | Details |
|---|---|
| Causative agent | Paragonimus westermani (Asia), P. kellicotti (North America) |
| Mode of infection | Eating raw/undercooked crabs or crayfish |
| Site of adult worm | Cystic cavities near bronchi in lung parenchyma |
| Egg size | ~80 x 50 μm, operculated, thick-shelled |
| Classic presentation | Hemoptysis + Rust-colored sputum + Eosinophilia |
| TB mimic | Yes - chronic hemoptysis + cavitation |
| Pathognomonic pleural fluid | Low glucose (<10) + Low pH (<7.1) + Eosinophils |
| Diagnosis | Eggs in sputum/stool; ELISA; complement fixation >1:8 |
| CT finding | Pleural effusion, nodules, worm cysts, serpentine tracks |
| Treatment | Praziquantel 75 mg/kg/day x 2 days |
| Extrapulmonary sites | Brain > skin > peritoneum |
Sources:
- Murray & Nadel's Textbook of Respiratory Medicine, 7e - Chapter 58 (Parasitic Infections), p. 1347-1349
- Murray & Nadel's Textbook of Respiratory Medicine, 7e - Chapter (Pleural Disease), p. (block 25, pleural paragonimiasis section)
- Fishman's Pulmonary Diseases and Disorders, 5e - p. 1219-1220
This is a shared conversation. Sign in to Orris to start your own chat.