describe the physiological principles of cardiopulmonary bypass Anaesthesiology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive, authoritative content from multiple anaesthesia textbooks. I have enough to write a thorough answer covering all the key physiological principles of CPB. Let me compile the response now.
Physiological Principles of Cardiopulmonary Bypass
Cardiopulmonary bypass (CPB) diverts venous blood away from the heart and lungs, performs gas exchange extracorporeally, and returns oxygenated blood to the systemic circulation - thereby providing both artificial ventilation and circulation simultaneously. This creates profoundly non-physiological conditions that require careful management.
The Basic Circuit
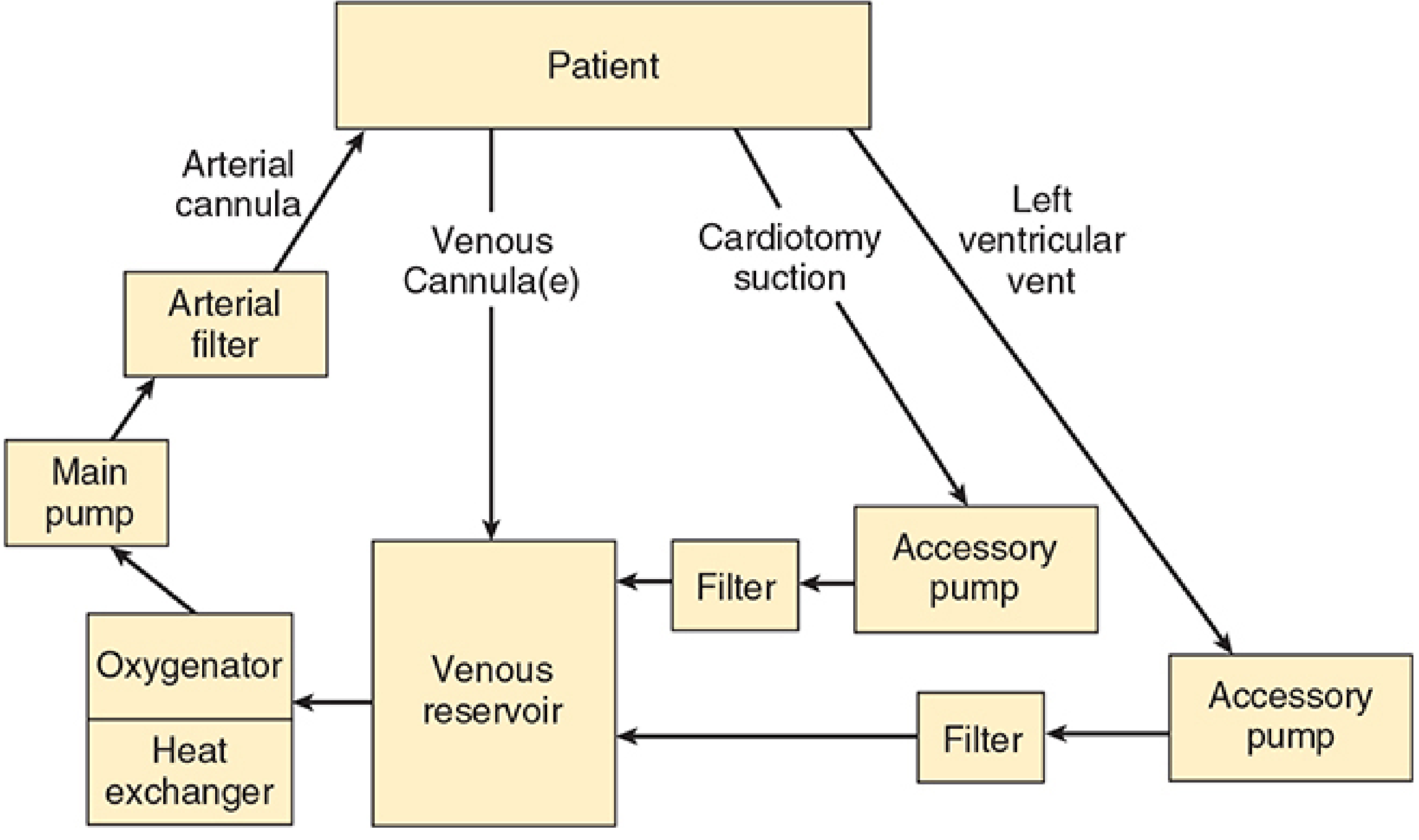
Basic design of the cardiopulmonary bypass circuit (Morgan & Mikhail's Clinical Anesthesiology, 7e)
The circuit has six essential components:
| Component | Function |
|---|---|
| Venous cannula(e) | Drain blood from the right atrium/venae cavae |
| Venous reservoir | Collects drained blood; serves as safety buffer |
| Oxygenator | Gas exchange (O₂ and CO₂) |
| Heat exchanger | Controls core temperature |
| Main pump | Propels blood through the circuit |
| Arterial filter | Traps air, fat, and particulate emboli |
Blood drains by gravity from the right atrium into the reservoir, driven by the height difference between patient and reservoir. From there it passes through the oxygenator, heat exchanger, main pump, arterial filter, and back via an arterial cannula (usually the ascending aorta or femoral artery).
1. Circuit Priming and Hemodilution
Before use, the circuit is primed with 1200-1800 mL of fluid (typically lactated Ringer's solution), which may include colloid, mannitol (to promote diuresis), heparin (500-5000 units), and bicarbonate. When CPB is initiated in adults, this crystalloid prime typically dilutes the hematocrit to approximately 22-27%. Blood is added to the prime for neonates, infants, and severely anemic adults to prevent excessive hemodilution.
Hemodilution reduces blood viscosity - an advantage during hypothermia when viscosity would otherwise rise markedly - but at the cost of reduced oxygen-carrying capacity. Adequate DO₂ is maintained by compensatory increases in cardiac output (pump flow rate) and by the shift of the oxyhemoglobin dissociation curve.
2. Pump Mechanics: Non-Pulsatile Flow
Roller Pumps
Roller pumps are positive-displacement pumps that compress large-bore tubing as the roller heads turn, producing nearly continuous, non-pulsatile flow. Flow is directly proportional to RPM. The rollers are set to subtotal occlusion to minimize red cell trauma. A critical hazard: if the reservoir empties, a roller pump will pump air directly into the patient.
Centrifugal Pumps
A series of spinning cones generate centrifugal force to propel blood. Unlike roller pumps:
- Flow is pressure-sensitive and must be monitored with a flowmeter
- They are nonocclusive - less traumatic to blood elements
- They cannot pump air into the patient - a significant safety advantage
- Located between the venous reservoir and oxygenator (vs. after the oxygenator for roller pumps)
Non-pulsatile flow is a fundamental departure from physiology. Mean arterial pressure is typically maintained at 50-70 mmHg with a pump output of approximately 2.2-2.4 L/min/m². The physiological consequences of non-pulsatile perfusion include altered baroreceptor activity, increased systemic vascular resistance, and activation of the renin-angiotensin-aldosterone system. Some evidence suggests pulsatile flow better preserves organ function, though non-pulsatile bypass is widely used with acceptable outcomes.
3. Oxygenation and Gas Exchange
Modern CPB uses membrane oxygenators - a thin, gas-permeable silicone membrane creates a blood-gas interface. The membrane design separates blood from gas flow, greatly reducing plasma protein denaturation, platelet activation, and microembolization compared to older bubble oxygenators.
Key control:
- PaO₂ is set by the inspired O₂ fraction
- PaCO₂ is controlled by the total gas flow rate past the oxygenator (sweep gas flow)
- A volatile anesthetic agent can be delivered via a vaporizer in the gas circuit
4. Systemic Hypothermia
Hypothermia is the single most powerful physiological tool for organ protection during CPB.
Temperature ranges used:
| Depth | Temperature | Application |
|---|---|---|
| Mild ("tepid") | 30-35°C | "Drift" hypothermia; commonly used |
| Moderate | 20-32°C | Standard CPB with cardiac surgery |
| Deep | 15-18°C | Complex repairs requiring circulatory arrest |
Mechanism: Metabolic oxygen requirements are halved for every 10°C reduction in temperature (Q₁₀ effect). At 15-18°C, total circulatory arrest for up to 60 minutes is feasible. The brain and heart are the organs most vulnerable to ischemia, and cooling extends their tolerance.
Adverse effects of hypothermia:
- Platelet dysfunction and coagulopathy
- Increased blood viscosity (partially offset by hemodilution)
- Depression of myocardial contractility
- Altered drug pharmacokinetics
- Electrolyte shifts (particularly potassium)
Rewarming occurs via the heat exchanger at the end of bypass. Because gas solubility decreases as temperature rises, a bubble trap is built into the heat exchanger unit to catch emboli that form during rewarming.
5. Anticoagulation
Contact of blood with the artificial surfaces of the CPB circuit activates the coagulation cascade and complement system. Heparin is the primary anticoagulant used:
- Dose: 300-400 units/kg IV bolus before cannulation
- Target: Activated clotting time (ACT) >400-480 seconds (vs. normal ~100-120 s)
- Reversal: Protamine sulfate (1 mg per 100 units of heparin given) after separation from bypass
ACT is the standard point-of-care monitoring test for heparin effect during CPB. Inadequate anticoagulation during bypass is catastrophic, leading to massive intravascular clotting.
6. Myocardial Protection
The heart must be protected during the period of aortic cross-clamping, when coronary blood flow is absent.
Cardioplegia
Cardioplegic solutions arrest the heart in diastole by depolarizing myocardial cell membranes. The key components are:
- High potassium (15-30 mmol/L): raises resting membrane potential and stops electrical activity
- Cold temperature (4°C): reduces metabolic demand
- Additional agents: magnesium (membrane stabilization), buffers (correct ischemic acidosis), glucose/glutamate (substrate preservation), calcium channel blockers
Cardioplegia can be delivered:
- Antegrade: into the aortic root (and thus coronary ostia) - simpler and most common
- Retrograde: via the coronary sinus - useful when antegrade delivery is unreliable (severe aortic regurgitation, ostial stenosis)
- Repeated doses every 20-30 min to maintain arrest and top up the protective effect
Pathophysiology of Inadequate Protection
When cross-clamp time is prolonged, ischemia depletes ATP, activates anaerobic glycolysis, causes intracellular acidosis, and leads to calcium overload. On reperfusion, free radical generation, calcium overload, and neutrophil-endothelial interactions cause reperfusion injury. The result ranges from reversible myocardial stunning (systolic and diastolic dysfunction that recovers with inotropic support) to irreversible myocardial necrosis.
7. pH Management During Hypothermia
Two strategies exist for managing acid-base status during hypothermic CPB:
| Strategy | Principle | Application |
|---|---|---|
| Alpha-stat | pH maintained at 7.40 when corrected to 37°C (ignores actual hypothermic pH) | Standard adult cardiac surgery; maintains autoregulation |
| pH-stat | CO₂ added to maintain pH 7.40 at actual body temperature | May be preferred for paediatric cases requiring deep hypothermic circulatory arrest (DHCA); promotes more uniform brain cooling |
Alpha-stat management preserves cerebrovascular autoregulation and is standard in most adult centres. pH-stat causes cerebral vasodilation and increased CBF, which may improve cerebral cooling in DHCA but risks more embolic delivery.
8. Systemic Inflammatory Response
Exposure of blood to the artificial surfaces of the CPB circuit triggers a whole-body inflammatory response involving:
- Complement activation (C3a, C5a) - anaphylatoxin release
- Neutrophil activation - elastase and oxygen radical release
- Cytokine cascade - TNF-α, IL-1, IL-6, IL-8
- Platelet activation and consumption
- Kallikrein-bradykinin activation - causing vasodilation and increased capillary permeability
Consequences include capillary leak, interstitial oedema, coagulopathy, and post-bypass organ dysfunction. Strategies to mitigate this include circuit miniaturisation, heparin-coated circuits, leukocyte filters, aprotinin (serine protease inhibitor), methylprednisolone, and modified ultrafiltration (especially in paediatric cases to remove inflammatory cytokines).
9. Organ Perfusion Targets During CPB
| Parameter | Target |
|---|---|
| Mean arterial pressure | 50-70 mmHg |
| Pump flow | 2.2-2.4 L/min/m² |
| SvO₂ (mixed venous O₂ saturation) | >65-70% |
| Haematocrit | >21% (adults); higher in infants |
| Temperature gradient (arterial-venous) | <10°C during rewarming |
| ACT | >400-480 s |
| Blood glucose | 6-10 mmol/L |
10. Weaning from CPB
Separation from bypass requires:
- Core temperature normalised (>36°C)
- Stable cardiac rhythm (pacing if needed)
- Adequate heart rate and rhythm
- Acceptable blood gas values and electrolytes
- Gradual reduction of pump flow as the heart resumes ejection, assessed by TEE
Failure to wean prompts re-examination of the surgical repair (by TEE and pressure measurements), and consideration of inotropic support (epinephrine, dobutamine, milrinone) or mechanical assist (intra-aortic balloon pump, LVAD).
Sources:
- Morgan & Mikhail's Clinical Anesthesiology, 7e - Chapter 22
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e - Chapter 39
- Miller's Anesthesia, 10e - Chapter 50
This is a shared conversation. Sign in to Orris to start your own chat.