I now have comprehensive content from Gray's Anatomy for Students to deliver a thorough and well-illustrated answer. Let me compile the full response.
Anatomy of the Abdomen
Source: Gray's Anatomy for Students
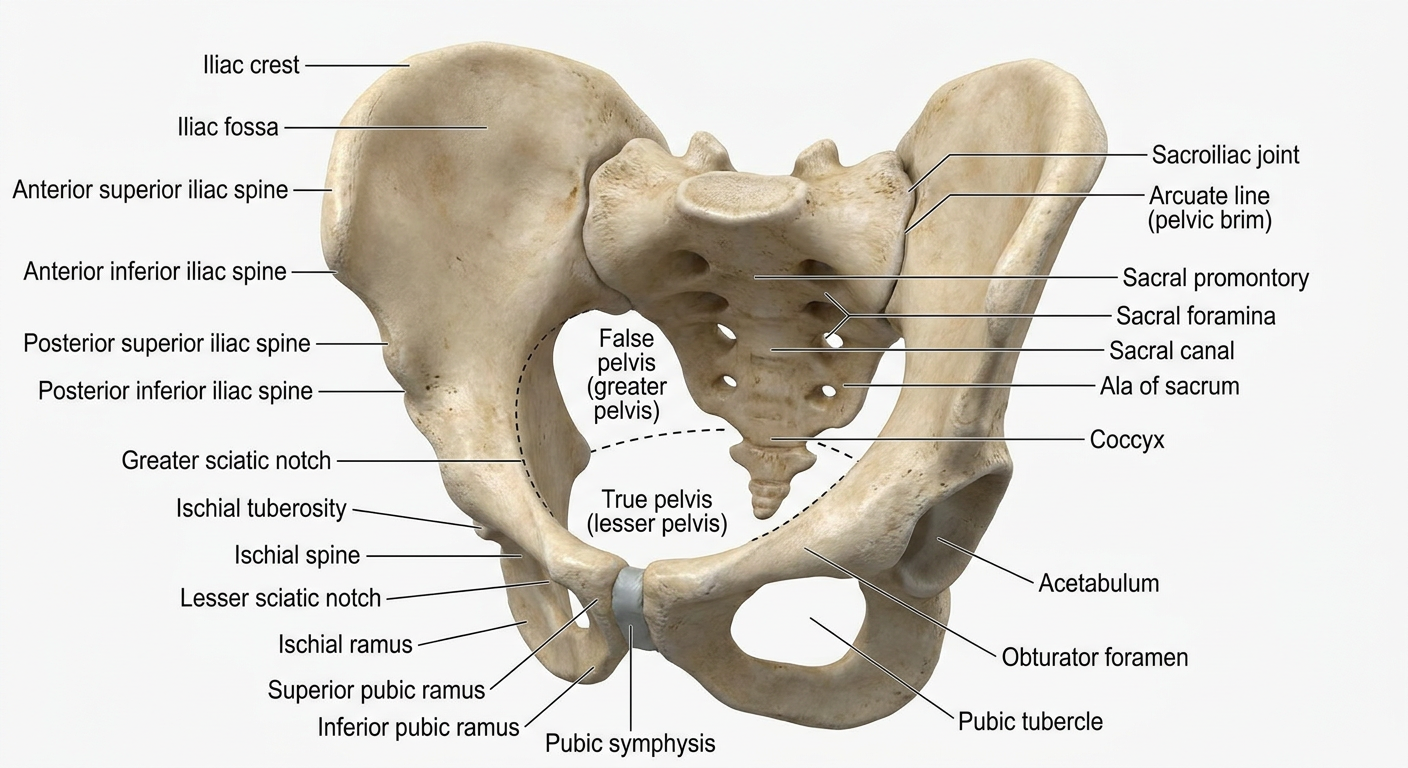
1. Boundaries and Surface Landmarks
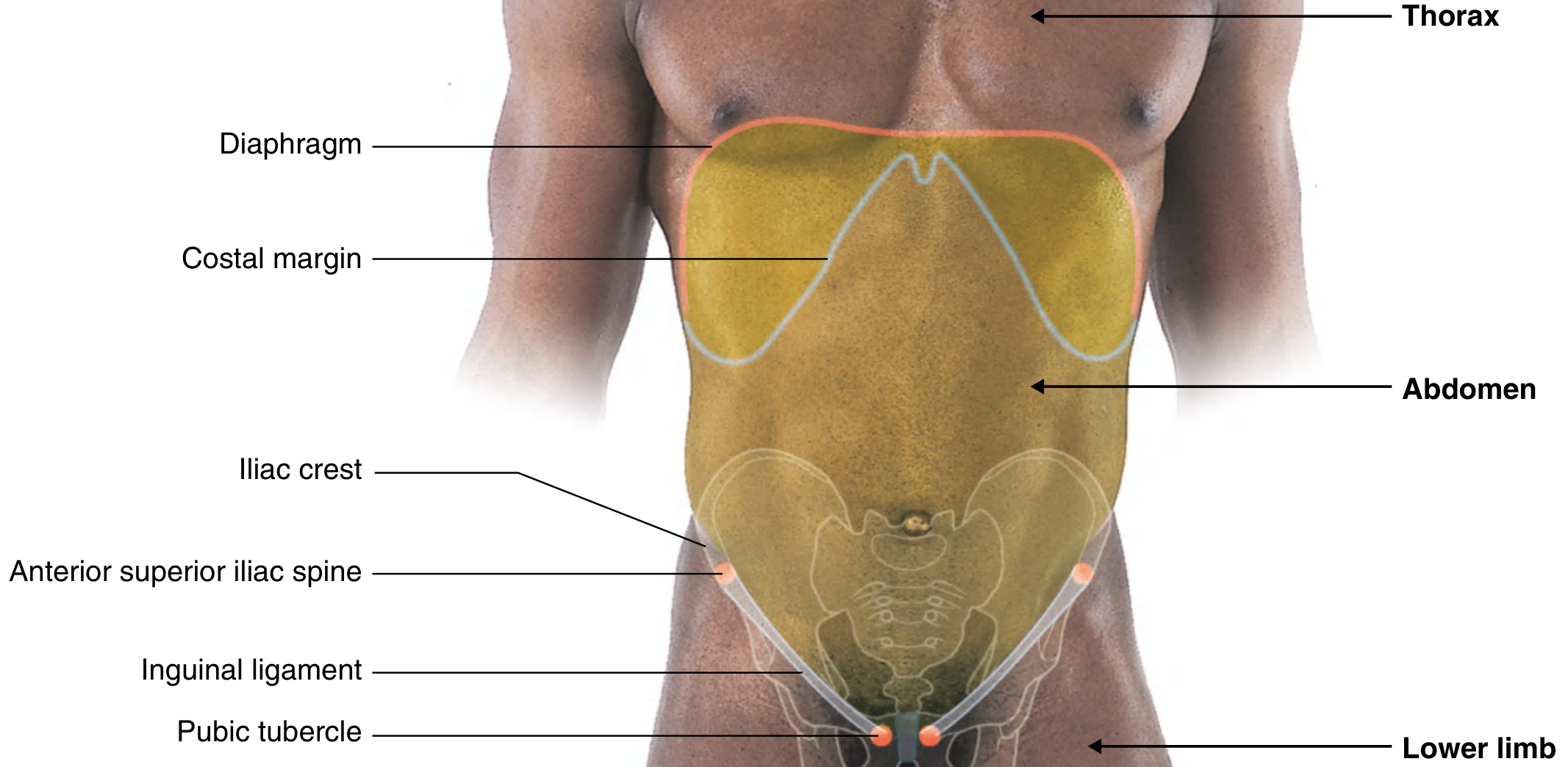
The abdomen is the region between the thorax above and the pelvis below. Its surface boundaries are:
- Superior: xiphoid process and costal margins (separates abdomen from thorax)
- Posterior: vertebral column
- Inferior: pubic tubercle, anterior superior iliac spine (ASIS), and iliac crest
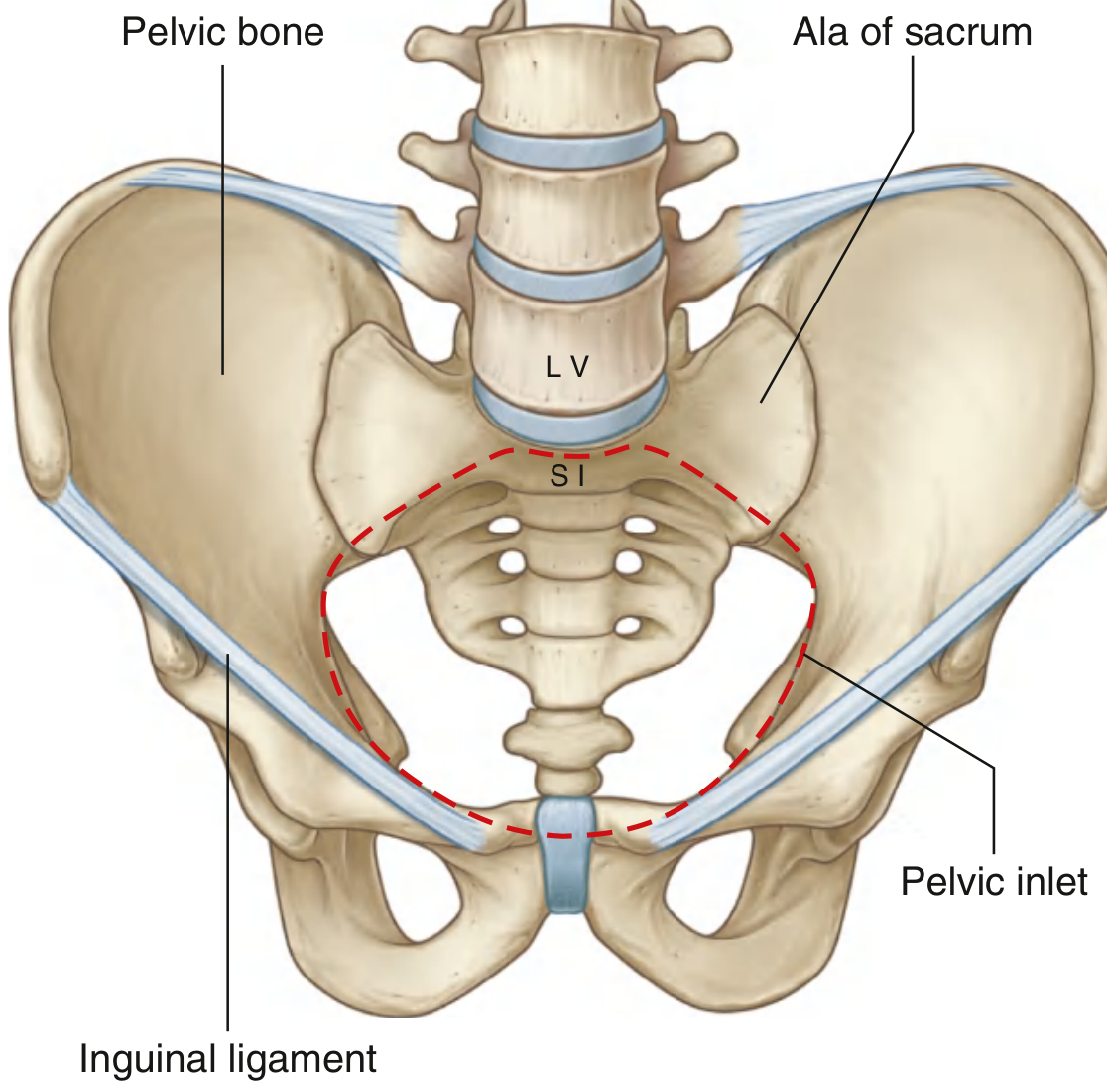
The inguinal ligament runs between the ASIS and the pubic tubercle, forming the boundary between the anterior abdominal wall and the thigh.
The upper part of the abdominal cavity projects above the costal margin to the diaphragm - abdominal viscera in this region are protected by the thoracic wall. The dome of the right diaphragm can reach as high as the 4th costal cartilage during forced expiration.
Fig. 4.180 - Surface landmarks of the abdominal region (Gray's Anatomy for Students)
2. Layers of the Abdominal Wall
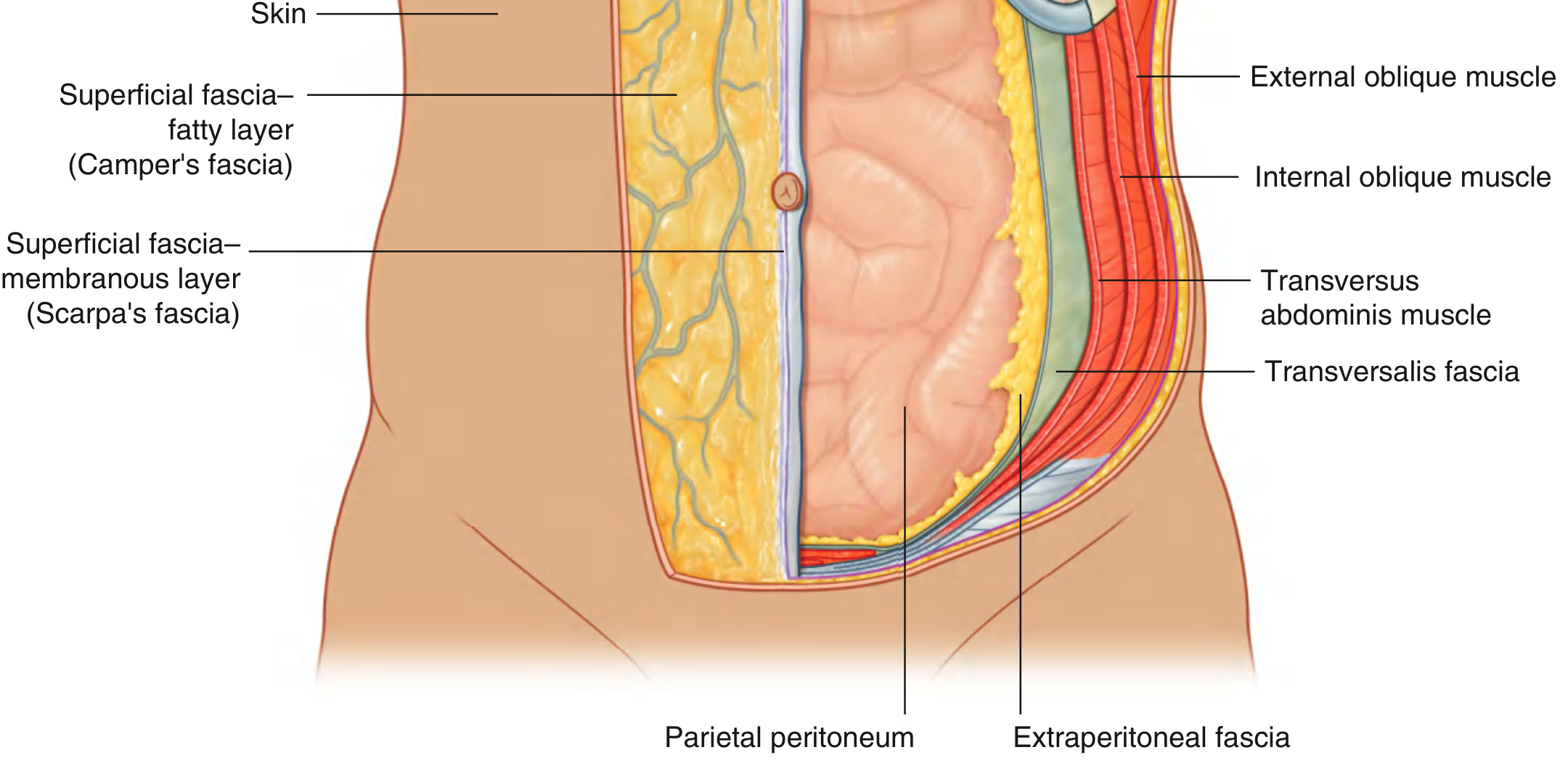
From superficial to deep, the anterolateral abdominal wall has the following layers:
- Skin
- Superficial fascia (subcutaneous tissue) - two layers below the umbilicus:
- Camper's fascia - superficial fatty layer; continuous with superficial fascia of the thigh and perineum
- Scarpa's fascia - deeper membranous layer with little fat; fuses with fascia lata just below the inguinal ligament
- Muscles and their aponeuroses
- Transversalis fascia
- Extraperitoneal fascia
- Parietal peritoneum
Fig. 4.24 - Layers of the Abdominal Wall (Gray's Anatomy for Students)
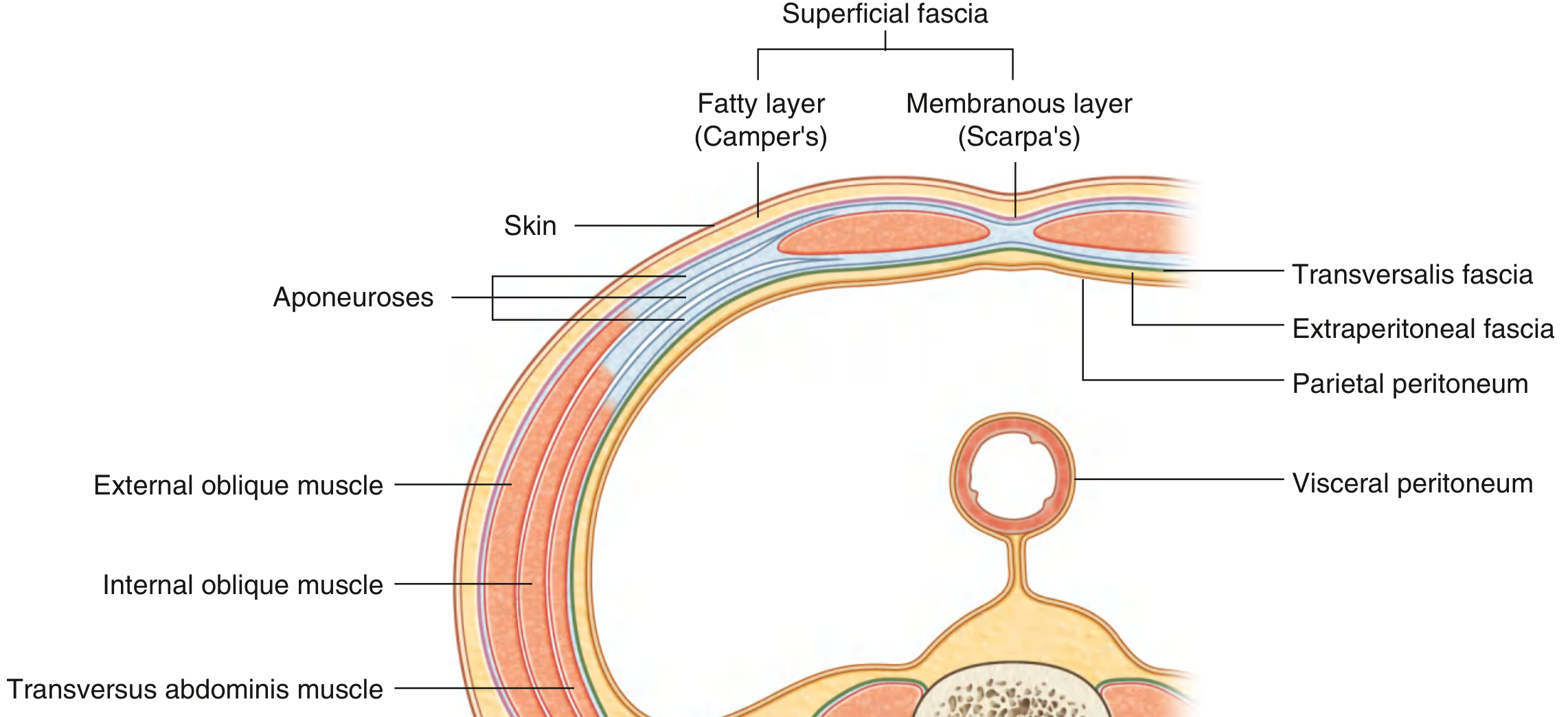
Fig. 4.34 - Transverse section showing layers including parietal and visceral peritoneum
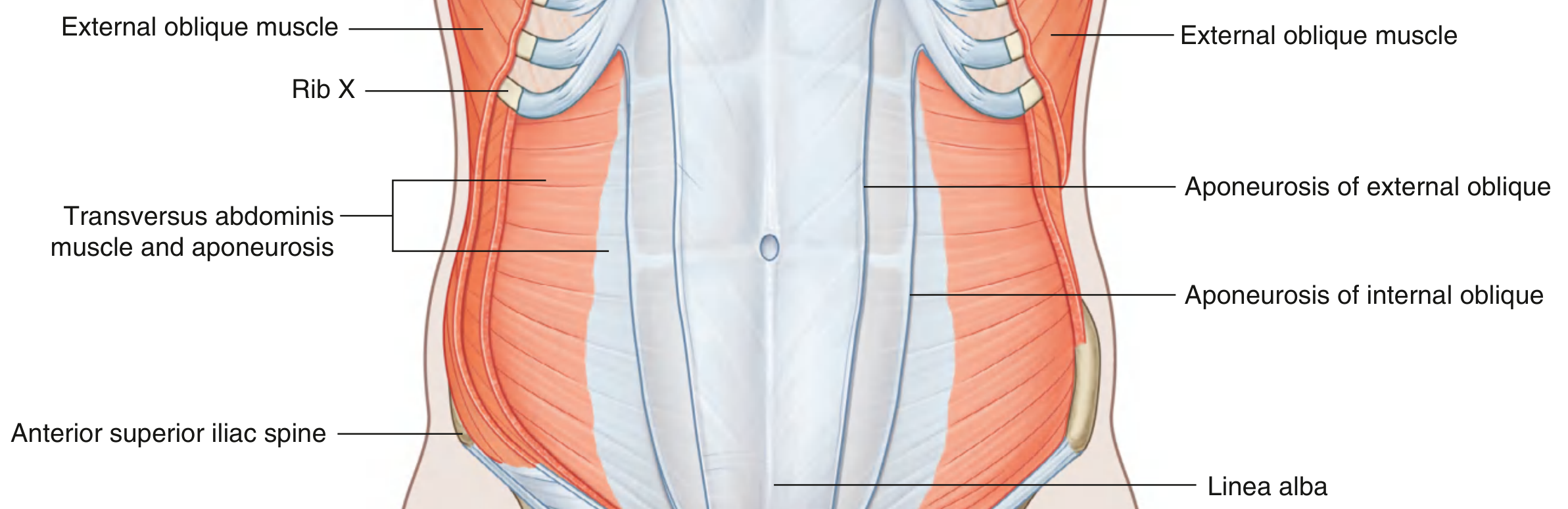
3. Muscles of the Anterolateral Abdominal Wall
Three flat muscles and one vertical muscle form the anterolateral wall:
Flat Muscles (lateral to medial)
| Muscle | Fiber Direction | Key Features |
|---|
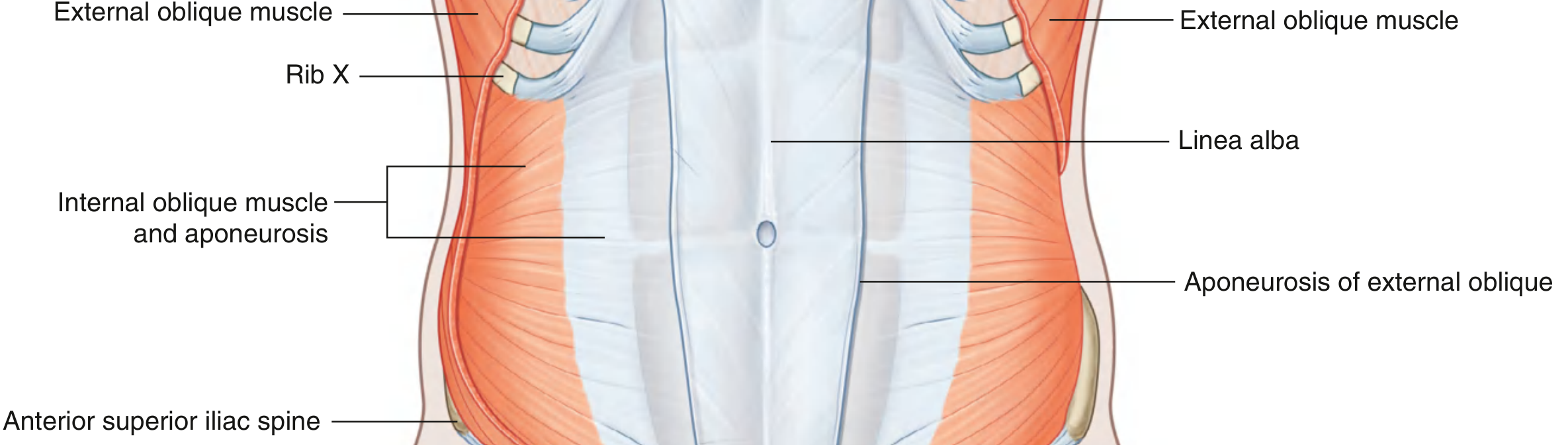
| External oblique | Inferomedial | Most superficial flat muscle; aponeurosis forms the inguinal ligament |
| Internal oblique | Superomedial | Smaller and thinner than external oblique |
| Transversus abdominis | Transverse | Deepest flat muscle; ends in anterior aponeurosis |
Fig. 4.30 - Internal Oblique Muscle and Aponeurosis
Fig. 4.31 - Transversus Abdominis Muscle and Aponeurosis
Vertical Muscle
- Rectus abdominis: Paired vertical muscles running from the pubis to the costal cartilages of ribs 5-7, enclosed in the rectus sheath formed by the aponeuroses of the three flat muscles.
The linea alba is a midline fibrous band formed by the interlacing aponeuroses of the three flat muscles on both sides.
Transversalis Fascia
A continuous layer of deep fascia lining the entire abdominal cavity; it continues into the pelvis and is continuous with the inferior surface of the diaphragm. Below the iliac crest, it becomes the parietal pelvic (endopelvic) fascia.
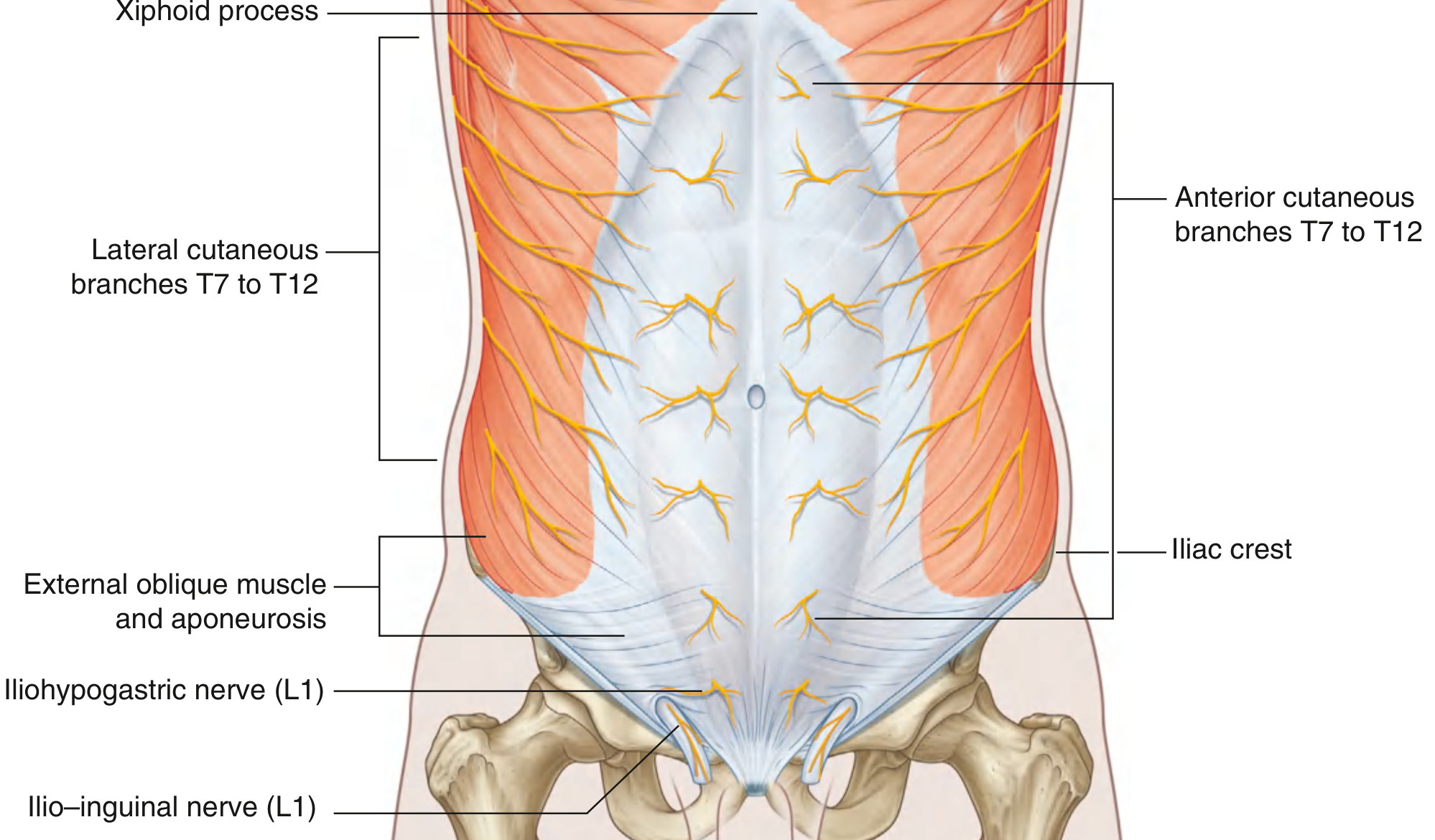
4. Innervation of the Abdominal Wall
The skin, muscles, and parietal peritoneum of the anterolateral wall are supplied by T7 to T12 and L1 spinal nerves. These anterior rami pass inferiorly and medially, giving off:
- Lateral cutaneous branches (T7-T12)
- Anterior cutaneous branches (T7-T12)
L1 contributes via:
- Iliohypogastric nerve (L1)
- Ilio-inguinal nerve (L1)
The intercostal nerves (T7-T11) leave their intercostal spaces, pass between the internal oblique and transversus abdominis, enter the rectus sheath, and pierce through as anterior cutaneous branches.
Fig. 4.36 - Innervation of the Anterolateral Abdominal Wall
5. Peritoneum
The peritoneum is a thin serous membrane with two layers:
- Parietal peritoneum - lines the walls of the abdominal cavity; supplied by somatic afferents (well-localized pain)
- Visceral peritoneum - covers the abdominal viscera; supplied by visceral afferents (poorly localized, referred pain)
The peritoneal cavity is the potential space between the two layers. It is:
- Closed in men
- Semi-closed in women (the uterine tubes provide two openings to the outside)
Intraperitoneal vs. Retroperitoneal Organs
- Intraperitoneal: suspended in the cavity by mesenteries (e.g., stomach, small intestine, transverse colon, spleen)
- Retroperitoneal: outside the peritoneal cavity, only partially covered by peritoneum (e.g., kidneys, duodenum 2nd-4th parts, pancreas, ascending/descending colon, aorta, IVC)
Omenta and Mesenteries
- Greater omentum: large apron-like peritoneal fold hanging from the greater curvature of the stomach; derived from the dorsal mesentery
- Lesser omentum: connects the liver to the stomach and the first part of the duodenum; derived from the ventral mesentery
- Mesentery of the small intestine: connects the jejunum and ileum to the posterior abdominal wall
- Transverse mesocolon: connects the transverse colon to the posterior wall
- Sigmoid mesocolon: connects the sigmoid colon to the posterior wall
Peritoneal ligaments connect organs to each other or to the body wall (e.g., splenorenal ligament, gastrophrenic ligament).
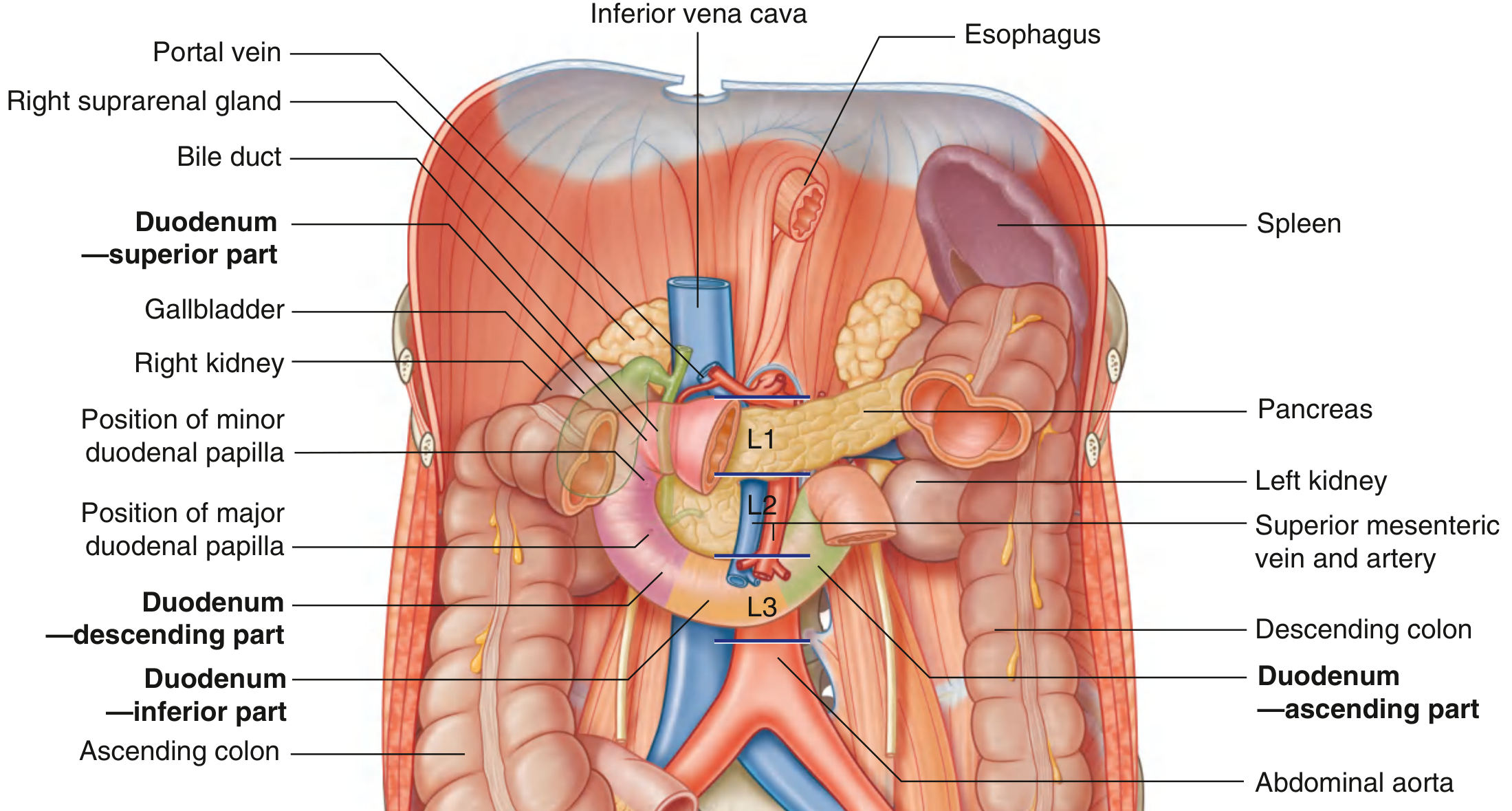
6. Abdominal Viscera
Gastrointestinal Tract
Abdominal esophagus
Emerges through the right crus of the diaphragm at vertebra TX; arterial supply from the left gastric artery (celiac trunk) and left inferior phrenic artery.
Stomach
J-shaped, most dilated GI structure; located in epigastric, umbilical, and left hypochondrium regions. Divided into:
- Cardia (near esophageal inlet)
- Fundus (dome-shaped upper portion)
- Body (main portion)
- Pyloric part (exits into duodenum via pyloric orifice)
Duodenum
C-shaped, 20-25 cm long, the first part of the small intestine. Divided into four parts:
- Superior (1st part): at vertebra LI; duodenal cap (most common site of duodenal ulcers)
- Descending (2nd part): to the right of midline, L1-L3; contains the major duodenal papilla (entry of bile and pancreatic ducts) and minor duodenal papilla; foregut-midgut junction just below the major papilla
- Inferior (3rd part): crosses the IVC, aorta, and vertebral column; crossed anteriorly by superior mesenteric vessels
- Ascending (4th part): ascends to the left of the aorta, terminates at the duodenojejunal flexure (supported by the ligament of Treitz)
Most of the duodenum is retroperitoneal (except the beginning, which is intraperitoneal).
Jejunum and Ileum: Intraperitoneal; arterial supply from branches of the superior mesenteric artery.
Fig. 4.67 - Abdominal Viscera Overview (note the four parts of the duodenum and adjacent structures)
7. Key Vascular Anatomy
Arterial Supply
The abdominal aorta enters through the aortic hiatus of the diaphragm at T12 and bifurcates into the common iliac arteries at L4. Its major branches supply the abdominal organs:
| Artery | Vertebral Level | Territory |
|---|
| Celiac trunk | T12/L1 | Foregut (distal esophagus to 2nd part duodenum, liver, gallbladder, pancreas, spleen) |
| Superior mesenteric | L1 | Midgut (distal duodenum to 2/3 transverse colon) |
| Renal arteries | L1/L2 | Kidneys and suprarenal glands |
| Inferior mesenteric | L3 | Hindgut (distal transverse colon to rectum) |
Venous Drainage
- The portal vein drains blood from the GI tract, spleen, pancreas, and gallbladder to the liver
- The inferior vena cava receives hepatic veins, renal veins, and drains below the diaphragm
8. Regions of the Abdomen
The abdomen is divided into 9 regions by two horizontal and two vertical planes:
| Left | Central | Right |
|---|
| Upper | Left hypochondrium | Epigastric | Right hypochondrium |
| Middle | Left lumbar (lateral) | Umbilical | Right lumbar (lateral) |
| Lower | Left iliac (inguinal) | Hypogastric (pubic) | Right iliac (inguinal) |
Alternatively, two planes divide it into 4 quadrants: right upper, left upper, right lower, left lower.
Summary of Key Clinical Points
- Umbilical hernias: usually congenital (failure of bowel to return from umbilical cord); most close in the first year of life
- Incisional hernias: through a defect in a surgical scar; wide necks, low risk of strangulation
- Spigelian hernia: passes through the arcuate line into the lateral border of the lower posterior rectus sheath
- Perforated duodenal ulcer: releases gas into the peritoneal cavity visible as subdiaphragmatic gas on erect chest X-ray
- Peritoneal dialysis: uses the large surface area of the peritoneum as a dialysis membrane
- Referred pain: visceral peritoneum pain is poorly localized (visceral afferents); parietal peritoneum pain is sharp and well-localized (somatic afferents)
All content sourced from Gray's Anatomy for Students and the Color Atlas of Human Anatomy, Vol. 2 (Internal Organs) - from the medical textbook library.