Neonatal jondice in explain in detail
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
I now have comprehensive, well-sourced information and both clinical charts. Let me compile the detailed answer.
Neonatal Jaundice (Neonatal Hyperbilirubinemia)
Neonatal jaundice is the yellow discoloration of the skin and sclera in newborns caused by elevated serum bilirubin. It is one of the most common clinical problems in the newborn period, affecting approximately 50% of term newborns in the first week of life. While most cases are benign and self-limited, severe hyperbilirubinemia can cause permanent brain injury.
1. Bilirubin Metabolism - The Basics
Bilirubin is the end-product of heme breakdown, primarily from hemoglobin. The pathway:
- Heme (from RBC breakdown) → biliverdin → unconjugated (indirect) bilirubin
- Unconjugated bilirubin binds to albumin in blood and is carried to the liver
- In the liver, it is conjugated by the enzyme glucuronyl transferase (UGT1A1) → conjugated (direct) bilirubin
- Conjugated bilirubin is excreted into bile and then the intestine
Three physiologic factors combine in neonates to cause hyperbilirubinemia:
- Increased bilirubin production (fetal Hb breakdown, larger RBC mass, shorter RBC lifespan ~70-90 days vs 120 in adults)
- Decreased hepatic clearance (immature glucuronyl transferase activity)
- Increased enterohepatic resorption (gut bacteria not yet established; beta-glucuronidase deconjugates bilirubin back to unconjugated form)
Jaundice in adults is usually a conjugated hyperbilirubinemia from primary hepatobiliary disease. Neonatal jaundice is usually unconjugated from extrahepatic causes. Conjugated hyperbilirubinemia in neonates is always pathologic. - Rosen's Emergency Medicine, p. 3225
2. Types of Neonatal Jaundice
A. Physiologic Jaundice (Most Common - ~50% of term newborns)
- Appears between days 2-3 of life (never on day 1)
- Peaks at day 4-5 (~6 mg/dL in healthy term infants)
- Resolves by 2 weeks of age in term infants, by 3 weeks in preterm
- Bilirubin rarely rises faster than 5 mg/dL/day
- Caused by immature hepatic conjugation + increased RBC breakdown
B. Breast Milk Jaundice (2nd most common)
- Peaks later: around 10-21 days of life
- Levels may persist 3-10 weeks before gradually declining
- Exact mechanism uncertain - may be hormonally mediated, or due to fatty acids in breast milk inhibiting UGT1A1, or increased enterohepatic circulation
- Mild unconjugated hyperbilirubinemia; benign
C. Pathologic Jaundice
- Jaundice appearing within the first 24 hours of life - almost always pathologic
- TSB > 5 mg/dL in first 24 hours
- Rising faster than 5 mg/dL/day
- Persisting beyond 3 weeks of age
- Conjugated (direct) bilirubin elevated (always pathologic)
- Associated with a sick-appearing infant
3. Causes - Differential Diagnosis
Unconjugated (Indirect) Hyperbilirubinemia
| Category | Examples |
|---|---|
| Benign/physiologic | Physiologic jaundice, breast milk jaundice |
| Hemolysis | ABO incompatibility, Rh incompatibility (HDFN), cephalhematoma breakdown, G6PD deficiency, hereditary spherocytosis, elliptocytosis, sickle cell, thalassemia, pyruvate kinase deficiency |
| Infectious | TORCHS infections, UTI, sepsis |
| Obstructive (bowel) | Meconium ileus, Hirschsprung disease, duodenal/pyloric stenosis |
| Metabolic/genetic | Galactosemia, congenital hypothyroidism, Crigler-Najjar syndrome (types I & II), Gilbert syndrome |
| Polycythemia | Twin-twin transfusion, delayed cord clamping |
Conjugated (Direct) Hyperbilirubinemia - Always Pathologic
| Category | Examples |
|---|---|
| Infectious | TORCHS, gram-negative sepsis, hepatitis B, HIV |
| Biliary obstruction | Biliary atresia, choledochal cyst, inspissated bile syndrome, Alagille syndrome |
| Metabolic | Galactosemia, tyrosinemia, alpha-1-antitrypsin deficiency, glycogen storage disease |
| Other | Parenteral nutrition, Dubin-Johnson syndrome, Rotor syndrome, neonatal hepatitis |
- Quick Compendium of Clinical Pathology, 5th ed., p. 288-291
4. Risk Factors for Severe Hyperbilirubinemia
- Prematurity (most important - immature BBB + less albumin)
- Isoimmune hemolysis (ABO or Rh incompatibility)
- Sepsis or infection
- Cephalhematoma or bruising (birth trauma hematoma)
- Dehydration (inadequate feeding)
- G6PD deficiency
- Hereditary spherocytosis
- Positive family history of neonatal jaundice
- East Asian or Mediterranean ethnicity
- Albumin < 3.0 g/dL
- Rosen's Emergency Medicine, p. 3226; Creasy & Resnik's Maternal-Fetal Medicine
5. Clinical Features
- Jaundice is clinically visible when TSB > ~5 mg/dL
- Progresses in a cephalocaudal pattern (face → trunk → extremities → palms/soles)
- Bilirubin level can be roughly estimated by extent:
- Face: ~5 mg/dL
- Trunk: ~10-12 mg/dL
- Below knees: ~15 mg/dL
- Palms/soles: >20 mg/dL (unreliable clinically; always confirm with lab)
Bilirubin-Induced Neurologic Dysfunction (BIND)
When TSB exceeds approximately 20-25 mg/dL, unconjugated bilirubin crosses the immature blood-brain barrier and damages neurons, especially in the basal ganglia, cerebellum, and brainstem nuclei.
Acute Bilirubin Encephalopathy (ABE) - Early (potentially reversible):
- Poor feeding, lethargy, hypotonia
- High-pitched cry
- Somnolence
ABE - Late (severe, may be irreversible):
- Hypertonia, retrocollis (neck arching backward), opisthotonos (body arching)
- Fever, irritability
- Apnea
- Seizures, death
Kernicterus (chronic, irreversible sequelae):
- Choreoathetosis, spastic quadriplegia
- Sensorineural hearing loss
- Upward gaze palsy (Parinaud syndrome)
- Mental retardation, cerebral palsy
- Learning disabilities
"Kernicterus is a neurologic syndrome resulting from neural necrosis and deposition of unconjugated bilirubin in the basal ganglia and brainstem nuclei. Clinical features may be acute or chronic, resulting in tone and movement disorders such as choreoathetosis and spastic quadriplegia, mental retardation, and sensorineural hearing loss." - Creasy & Resnik's Maternal-Fetal Medicine, p. 1791
6. Diagnosis and Workup
Initial assessment:
- Visual inspection + transcutaneous bilirubinometry (TcB) - screening tool
- Total serum bilirubin (TSB) - confirmatory, most reliable
Indications for full laboratory evaluation (Box 166.1, Rosen's):
- Jaundice appearing within 24 hours of birth
- Elevated direct (conjugated) bilirubin
- Rapidly rising TSB unexplained by history/exam
- TSB approaching exchange level or not responding to phototherapy
- Jaundice persisting beyond 3 weeks of age
- Sick-appearing infant
Labs to order:
- TSB (total and direct/conjugated fraction)
- Blood type and Rh (mother and baby)
- Direct antiglobulin test (Coombs test) - for hemolytic disease
- CBC with differential and reticulocyte count
- Peripheral blood smear (spherocytes, elliptocytes)
- G6PD assay
- Serum albumin
- If sepsis suspected: blood culture, urinalysis, urine culture
- If metabolic cause suspected: TFTs, metabolic screen (galactosemia)
- Liver function tests if direct hyperbilirubinemia present
Plotting bilirubin on the Bhutani nomogram by hour of life is key to risk stratification.
7. Treatment
A. Phototherapy - First-Line
Phototherapy converts unconjugated bilirubin into water-soluble photoisomers (lumirubin, configurational isomers) that are excreted directly into bile without requiring hepatic conjugation.
- Blue-green light spectrum (430-490 nm) is most effective
- "Intensive phototherapy": irradiance ≥ 30 μW/cm²/nm
- Eyes must be covered; genitals shielded
- Continue until TSB falls below threshold
AAP Guidelines for Phototherapy (infants ≥ 35 weeks):
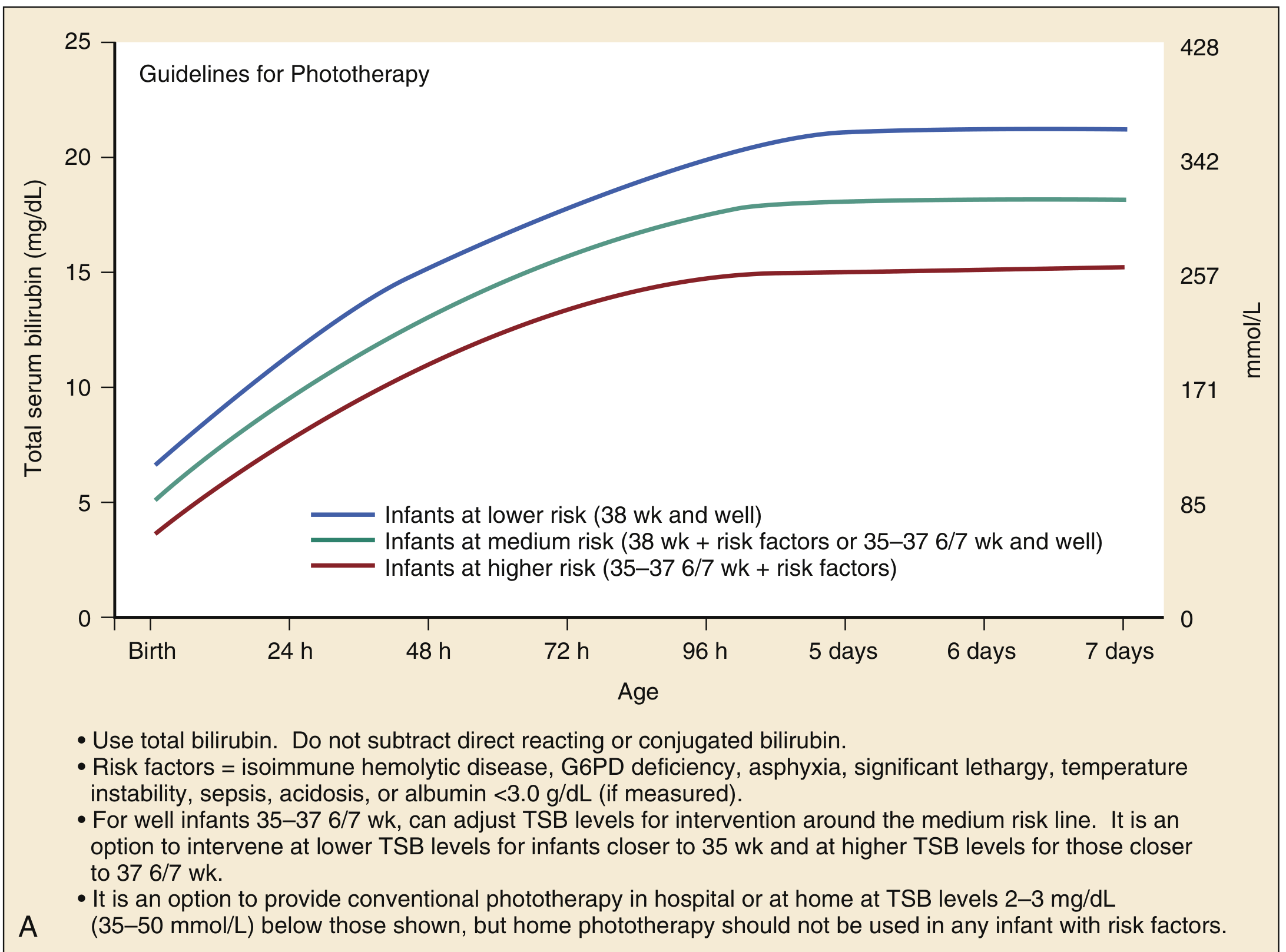
- Lower risk (38 wk and well): phototherapy threshold ~15-21 mg/dL depending on age
- Medium risk (38 wk + risk factors, or 35-37 6/7 wk and well): lower thresholds apply
- Higher risk (35-37 6/7 wk + risk factors): phototherapy started at lower TSB levels
Risk factors for guideline purposes: isoimmune hemolytic disease, G6PD deficiency, asphyxia, significant lethargy, temperature instability, sepsis, acidosis, albumin < 3.0 g/dL
B. Exchange Transfusion - For Severe Cases
AAP Guidelines for Exchange Transfusion (infants ≥ 35 weeks):
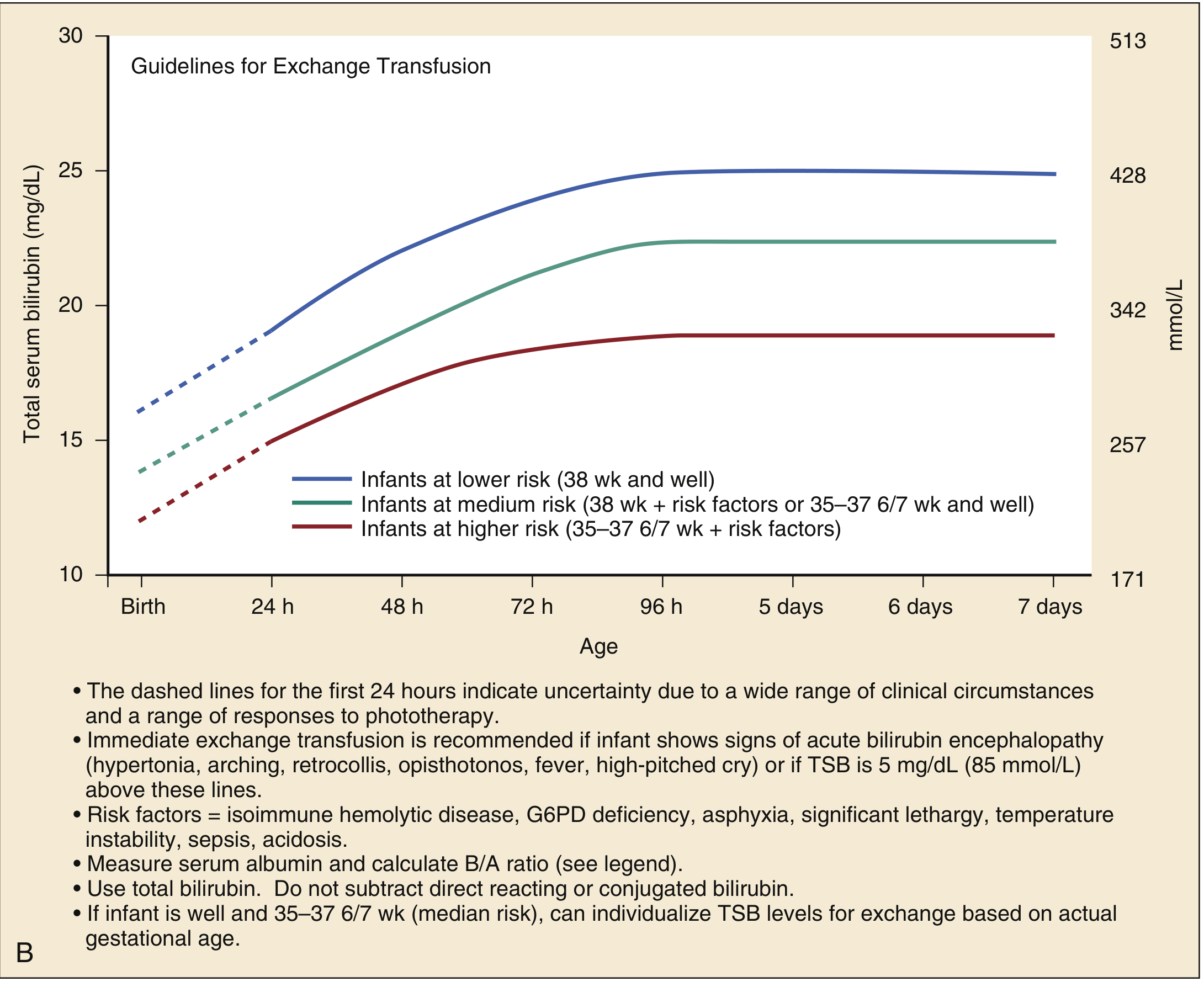
Indications:
- TSB above age- and risk-specific threshold (as per nomogram above)
- Failure of phototherapy (TSB continues to rise)
- Signs/symptoms of acute bilirubin encephalopathy
- Immediate exchange if TSB is 5 mg/dL above exchange lines + signs of ABE
Procedure:
- Double-volume exchange (180-190 mL/kg packed RBCs)
- Replaces approximately 85% of infant's blood volume
- Reduces TSB by at least 50%
- Serial small aliquots of 5-10 mL/kg removed and replaced
- Must be performed in NICU/PICU setting with hemodynamic monitoring
- Complications include: hypocalcemia, thrombocytopenia, hypothermia, cardiac arrhythmia, infection, air embolism
- Rosen's Emergency Medicine, p. 3228
C. Other Measures
- IV hydration: for dehydrated infants; helps increase bilirubin excretion
- Adequate feeding: encourages gut motility and reduces enterohepatic circulation
- Tin-mesoporphyrin: inhibits heme oxygenase (reduces bilirubin production) - not widely used
- IVIG: in isoimmune hemolytic disease (ABO/Rh incompatibility), reduces hemolysis
- Breast milk interruption: temporarily stopping breastfeeding for 24-48 hours can lower bilirubin in breast milk jaundice (rarely needed)
8. Disposition
- Home phototherapy: option for well-appearing infants with reliable caregivers and follow-up within 24 hours
- Hospital admission indicated for:
- Ill-appearing infant
- Inadequate oral intake or weight loss
- TSB approaching exchange level
- Direct hyperbilirubinemia (always admit - needs workup)
- Exchange transfusion needed
9. Prevention
- Universal bilirubin screening before hospital discharge
- Follow-up within 24-48 hours of discharge (especially if discharged early)
- Support and encourage breastfeeding
- Parental education on signs of jaundice and when to return
- Pre-discharge risk stratification using the Bhutani nomogram (TSB by hour of life)
- Identify Rh/ABO incompatibility antenatally
"Kernicterus is largely preventable. Close collaboration between prenatal and postnatal caretakers ensures accurate dissemination of information regarding risk factors... predicting nonhemolytic neonatal hyperbilirubinemia can be based upon readily available maternal and obstetric risk factors." - Creasy & Resnik's Maternal-Fetal Medicine, p. 1792
10. Summary Table
| Feature | Physiologic | Pathologic |
|---|---|---|
| Onset | Day 2-3 | First 24 hours |
| Peak | Day 4-5 | Variable |
| Resolution | By 2 weeks | Variable |
| TSB | < 15 mg/dL (term) | Often > 15 mg/dL |
| Bilirubin type | Unconjugated | Conjugated = always pathologic |
| Rise rate | < 5 mg/dL/day | > 5 mg/dL/day |
| Associated illness | None | May be present |
| Treatment | Observation ± phototherapy | Phototherapy + specific treatment |
Sources:
- Rosen's Emergency Medicine, 9th Ed. - Chapter 166 (Neonatal Jaundice), pp. 3225-3228
- Creasy & Resnik's Maternal-Fetal Medicine - Chapter 73, pp. 1791-1792
- Quick Compendium of Clinical Pathology, 5th Ed., pp. 288-311
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025), pp. 1054-1065
- Harriet Lane Handbook, 23rd Ed. (Johns Hopkins Hospital)
This is a shared conversation. Sign in to Orris to start your own chat.