Pap smear
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cervical cancer screening" AND "Pap smear"
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive textbook content on the Pap smear. Let me compile a thorough, well-organized answer.
Pap Smear (Papanicolaou Test)
Overview
The Pap smear, named after its developer George Papanicolaou who introduced it in the 1920s, is a cervical cancer screening test that uses exfoliated cells scraped from the cervix to detect dysplastic or malignant changes under microscopy. It has been one of the most successful cancer screening tools in history - observational studies show a 60-90% reduction in cervical cancer incidence and 20-60% reduction in mortality in populations with widespread screening programs. - Junqueira's Basic Histology, p. 1151; Symptom to Diagnosis, p. 34
Anatomy and the Transformation Zone
The area of greatest clinical importance is the transformation zone (TZ) - where the squamous epithelium of the ectocervix meets the mucus-secreting columnar epithelium of the endocervix at the squamocolumnar junction (SCJ). This zone must be completely sampled for an adequate Pap smear. The SCJ location changes with age:
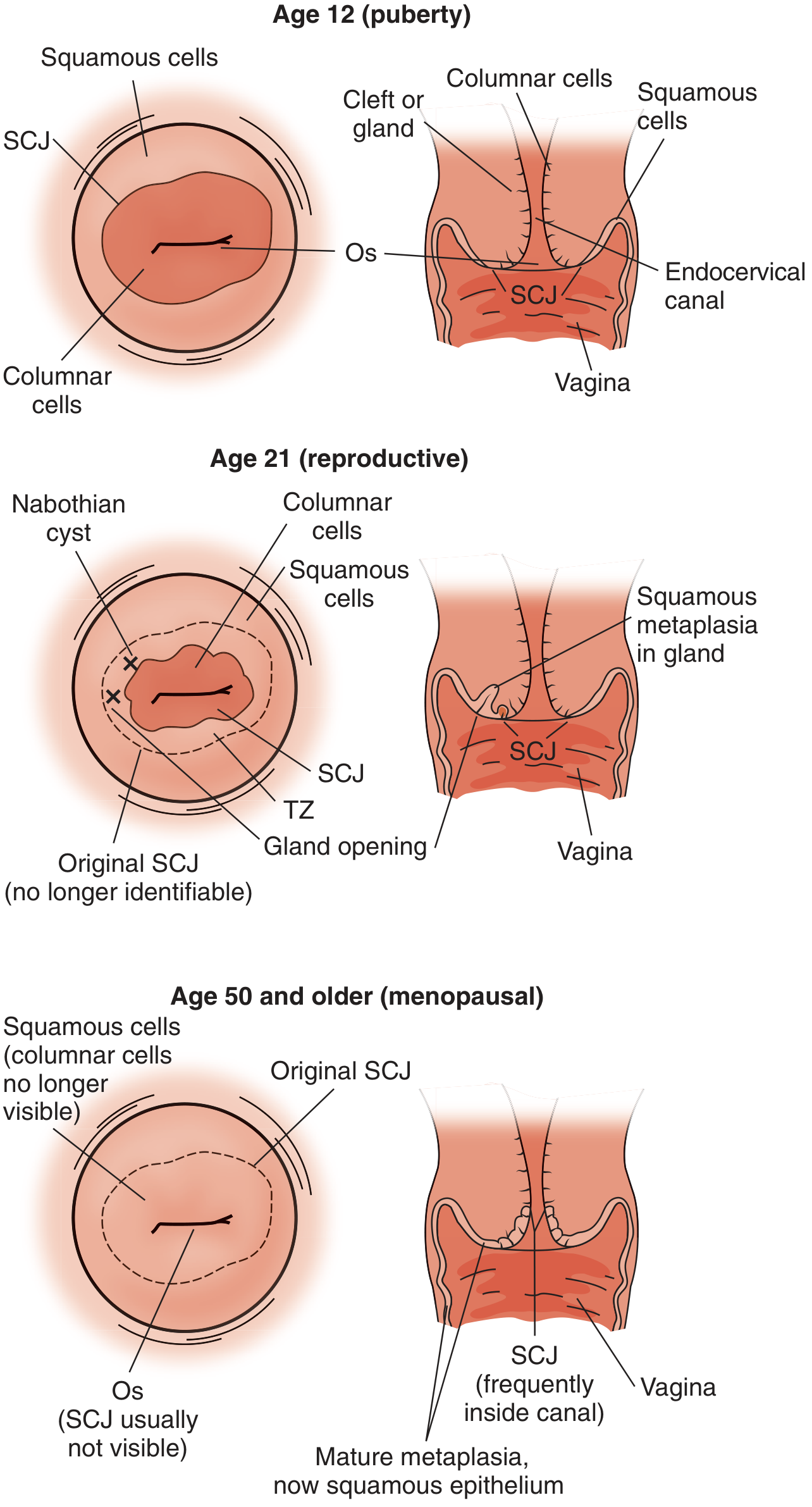
- At puberty: SCJ is large and visible on the ectocervix
- Reproductive age: SCJ migrates, TZ is identifiable but the original SCJ is no longer visible
- Menopause and older: SCJ migrates into the canal and is no longer visible - this can limit sampling
Epithelial dysplasia begins in metaplastic cells of the TZ, typically occurring at a mean age of 54 for squamous cell neoplasia. HPV infection is strongly implicated. - Pfenninger and Fowler's Procedures for Primary Care, p. 1053
Technique
Equipment
- Speculum and exam gloves
- Sampling devices: Cytobrush, Cervex-Brush (broom), or Papette - the cotton swab and tongue blade are discouraged
- Glass slides + fixative spray, or liquid-based transport medium (ThinPrep, SurePath)
Step-by-Step Procedure
- Insert speculum, visualize the cervix - note the TZ, SCJ, and any gross lesions
- Gently blot (do not rub) excess mucus only if truly necessary - it may contain exfoliated cells needed for analysis
- Endocervical sampling: Insert the Cytobrush into the canal, rotate 90-180 degrees only (more rotation causes bleeding that can wash away or obscure abnormal cells)
- Ectocervical/TZ sampling: Rotate a spatula 360 degrees over the entire TZ; or use broom devices (Cervex-Brush, Papette) which sample both areas simultaneously with 5 rotations of 360 degrees
- Glass slide method: Apply ectocervical spatula sample first, then roll the Cytobrush material over it, spray with cytofixative within 5 seconds to prevent drying artifact
- Liquid-based method: Rinse the device into a vial of transport liquid (ThinPrep or SurePath) instead of applying to glass slides
- Obtain cervical cultures after cytologic sampling if indicated
- Pfenninger and Fowler's Procedures for Primary Care, pp. 1054-1058
Methods: Conventional vs. Liquid-Based Cytology
| Feature | Conventional | Liquid-Based (ThinPrep/SurePath) |
|---|---|---|
| Cell application | Spread directly on glass slide by examiner | Cells rinsed into vial, processed in lab |
| FDA approval | Standard | Both approved as alternatives |
| HPV reflex testing | Not available | ThinPrep only (FDA-approved for reflex HPV) |
| Sensitivity/specificity | Similar | Similar (no advantage in detection of high-grade CIN) |
| Advantage | Lower cost | Allows "reflex" HPV testing on same specimen; fewer inadequate samples |
Liquid-based Pap smear testing is neither more sensitive nor more specific for high-grade CIN compared to the conventional Pap. The clearer advantage is the ability to perform reflex HPV DNA testing from the same vial. - Pfenninger and Fowler's Procedures for Primary Care, p. 1054
Test Characteristics
-
Sensitivity for HSIL: ~56%; for LSIL: ~77%
-
Specificity for HSIL: ~97%; for LSIL: ~80%
-
HPV testing is more sensitive but less specific for CIN 2/3; false-positive rates are higher in women under 35
-
Symptom to Diagnosis, p. 34
Bethesda 2001 Classification System
Pap smear results are reported using the Bethesda 2001 terminology:
1. Negative for Intraepithelial Lesion or Malignancy (NILM)
- Normal, including benign cellular changes
2. Epithelial Cell Abnormalities - Squamous
| Bethesda Term | Histologic Equivalent | Meaning |
|---|---|---|
| ASC-US | Variable | Atypical squamous cells of undetermined significance |
| ASC-H | Variable | Atypical squamous cells, cannot exclude HSIL |
| LSIL | CIN 1 (mild dysplasia), HPV effect | Low-grade squamous intraepithelial lesion; ≤1/3 of epithelium involved |
| HSIL | CIN 2/3, CIS | High-grade squamous intraepithelial lesion; >1/3 to entire epithelium involved |
| Squamous cell carcinoma | Frankly invasive cancer | Invasion >3 mm below basement membrane |
3. Epithelial Cell Abnormalities - Glandular
- AGC (atypical glandular cells) - previously called AGC-US, but the "US" was dropped because 10% harbor cancer and 25% harbor high-grade lesions; all AGC reports require further investigation
- Atypical endocervical/endometrial cells, favor neoplasia
- Endocervical adenocarcinoma in situ (AIS)
- Adenocarcinoma
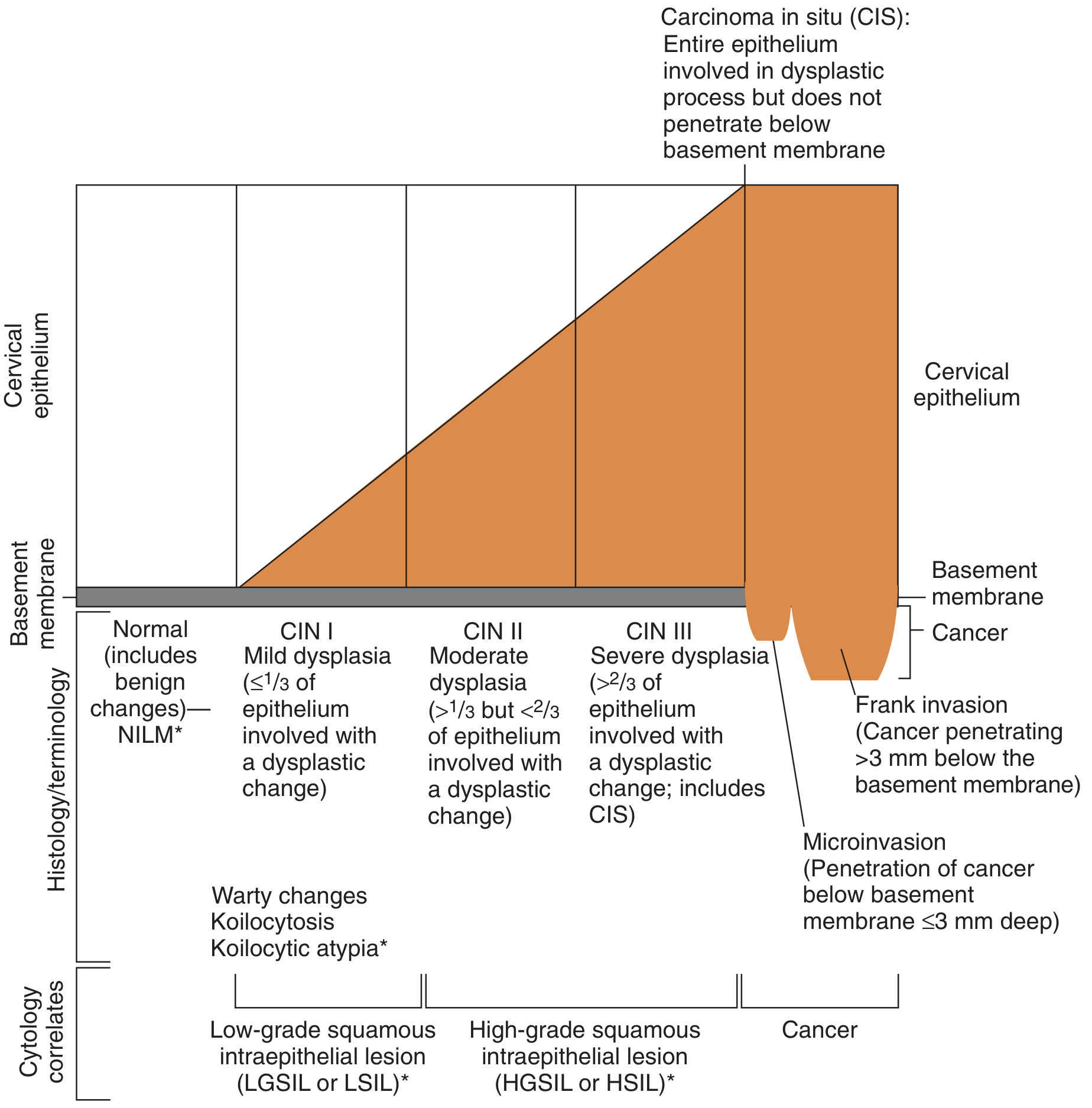
The diagram above shows the correlation between the degree of epithelial involvement and cytologic findings. Invasion below the basement membrane signals invasive cancer.
- Pfenninger and Fowler's Procedures for Primary Care, Box 151-2; Swanson's Family Medicine Review
Screening Guidelines
USPSTF 2018 (Grade A)
| Age Group | Recommendation |
|---|---|
| < 21 years | No screening (Grade D) |
| 21-29 years | Cytology (Pap smear) every 3 years |
| 30-65 years | Cytology every 3 years, OR HPV alone every 5 years, OR co-testing (cytology + HPV) every 5 years |
| > 65 years | Discontinue if adequate prior screening (3 consecutive negative cytology or 2 negative HPV results within last 10 years, most recent within 5 years) |
| Post-hysterectomy (benign, no CIN 2/3 history) | Discontinue (Grade D) |
ACOG 2016
- Cytology every 3 years for women ages 21-65, or
- Cytology every 3 years (ages 21-29) + co-testing (cytology + HPV) every 3 years for ages 30-65
Special Situations
-
Post-dysplasia treatment: Continue Pap smears at least annually for life (significant recurrence risk)
-
After hysterectomy for dysplasia/cancer: Continue annually after 3-4 normal smears at 4-6 month intervals
-
DES-exposed offspring: Require modified protocols and colposcopic evaluation
-
Immunocompromised women: Continue screening beyond age 65
-
Rape/abuse victims: Pap smear is part of the initial work-up
-
Symptom to Diagnosis, p. 34; Pfenninger and Fowler's Procedures for Primary Care, pp. 1052-1053
Management of Abnormal Results
| Result | Management |
|---|---|
| ASC-US | (1) Repeat cytology at 6-month intervals x2; or (2) Reflex HPV DNA testing - colposcopy if high-risk HPV+; or (3) Immediate colposcopy. HPV-based triage has 90-96% sensitivity vs. 75-85% for repeat Pap. HPV-negative ASC-US has ≥98% negative predictive value. |
| ASC-H | Colposcopy |
| LSIL | Colposcopy (majority resolve spontaneously - ablative/excisional therapy NOT acceptable without first doing colposcopy) |
| HSIL | Colposcopy with endocervical curettage |
| AGC | Colposcopy + endocervical sampling; if no lesion found, endometrial sampling |
| Any gross cervical lesion | Pap smear is NOT diagnostic - biopsy directed by colposcope is required regardless of Pap result |
- Swanson's Family Medicine Review, pp. 1757-1779
Risk Factors for Cervical Neoplasia
- HPV infection (necessary precursor; HPV 16 carries the greatest risk)
- Most HPV infections (90%) resolve within 2 years; the persistent 10% have potential to progress
- Smoking
- Immunocompromised state
- Early age of first intercourse
- Multiple sexual partners
- Alcohol use is not an associated risk factor
Relative Contraindications
There are no absolute contraindications to obtaining a Pap smear. Relative contraindications include active vaginitis, cervicitis, PID, or menses - where sample collection or interpretation may be difficult. However, the Pap smear should still be obtained if clinically warranted.
- Pfenninger and Fowler's Procedures for Primary Care
Recent Evidence (2024-2026)
A 2026 systematic review and meta-analysis (PMID 42142346) examined liquid-based cytology vs. conventional Pap smear in cervical cancer screening - supporting the continued role of both methods. A 2024 systematic review (PMID 39558397) assessed AI in cytopathology, noting promising accuracy for automated Pap smear reading - though this is not yet standard of care.
This is a shared conversation. Sign in to Orris to start your own chat.